ARTIGO ORIGINAL
Intra and inter-rater reliability of ultrasonographic evaluation of longus colli
muscle in women with migraine
Confiabilidade intra e interexaminadores da
avaliação ultrassonográfica do músculo longo do pescoço em mulheres com
migrânea
Camila Carolinne
Silva de Almeida*, Thaís Ferreira Lopes Diniz Maia*, Débora Wanderley**, Gisela
Rocha de Siqueira***, Claudia Regina Oliveira de Paiva Lima****, Maria Cristina
Falcão Raposo*****, Joaquim José de Souza Costa Neto******, Daniella Araújo de Oliveira******
*MD
student, Postgraduate Program in Physical Therapy, Universidade Federal de
Pernambuco, Recife/PE, Brazil, **MD, Postgraduate Program in Physical Therapy,
Universidade Federal de Pernambuco, Recife/PE, Brazil, ***PhD, Mother and Child
Health at Instituto de Medicina Integral Professor Fernando Figueira (IMIP),
Universidade Federal de Pernambuco, Recife/PE, Brazil, ****PhD, Statisitics,
Universidade de Sao Paulo, São Paulo/SP, Brazil, *****PhD, Economy, Universidde
Federal de Pernambuco, Recife/PE, Brazil, ******PhD, Neuropsychiatry and
Behavioral Science, Universidade Federal de Pernambuco, Recife/PE, Brazil
Recebido 9 de novembro de 2016; aceito em 25 de maio de 2017.
Corresponding
author:
Daniella Araújo de Oliveira, Departamento de Fisioterapia, Universidade Federal
de Pernambuco (UFPE), Av. Jornalista Anibal Fernandes, s/n, Cidade
Universitária, 50740-560 Recife PE, E-mail: sabinodaniellaufpe@gmail.com;
Camila Carolinne Silva de Almeida: kamilla0110@gmail.com; Thaís Ferreira Lopes Diniz
Maia: thais_maia4@hotmail.com; Débora Wanderley: deborawanderley84@hotmail.com;
Gisela Rocha de Siqueira: giselarsiqueira@gmail.com; Claudia Regina Oliveira de
Paiva Lima: claudia@de.ufpe.br; Maria Cristina Falcão Raposo:
cristina@de.ufpe.br; Joaquim José de Souza Costa Neto: joaqcosta@yahoo.com.br
Resumo
Objetivo: Determinar a
confiabilidade intra e interexaminadores das medidas ultrassonográficas do
músculo longo do pescoço em mulheres com e sem migrânea. Métodos: Trata-se de um estudo transversal, avaliando 20 mulheres
com idade entre 20 e 24 anos (22 ± 2). Foram realizadas duas avaliações
ultrassonográficas da área de secção transversa (cm2) do músculo
longo do pescoço, em repouso e em contração com intervalo de uma semana entre
elas, por dois examinadores cegos. Para análise estatística, foram utilizados o
coeficiente de correlação intraclasse (ICC) e os limites de concordância. Resultados: A confiabilidade
intraexaminador do grupo com migrânea, em repouso e contração, foi excelente à
direita e moderada à esquerda; no grupo sem migrânea variou de excelente (0,93)
no repouso, à pobre (0,35) na contração. A confiabilidade interexaminadores foi
excelente (ICC > 0,75) à direita e à esquerda, no repouso, em ambos os
grupos. Na contração, variou de moderada (ICC = 0,71), no lado esquerdo no
grupo sem migrânea, à excelente (ICC > 0,75) nas demais mensurações. Foram
observados baixos limites de concordância dos intervalos de confiança em todas
as medidas. Conclusão: Foram
observados baixos limites de concordância, de acordo com o intervalo de
confiança, na confiabilidade das medidas ultrassonográficas do músculo longo do
pescoço em mulheres com migrânea.
Palavras-chave: transtornos da
enxaqueca, músculos do pescoço, ultrassonografia, reprodutibilidade.
Abstract
Objective: To determine
intra and inter-rater reliability of ultrasonographic
measures of the longus colli muscle in women with and
without migraine. Methods: This is a
cross-sectional study involving 20 women aged between 20 and 24 years (22 ± 2).
Two ultrasonographic assessments, conducted one week
apart by two blind examiners, were made of the cross-sectional area (cm2)
of the longus colli muscle, at rest and in
contraction. Statistical analysis used the intraclass
correlation coefficient (ICC) and limits of agreement. Results: Intra-rater reliability in the group with migraine, at
rest and in contraction, was excellent on the right and moderate on the left;
in the group without migraine it ranged from excellent (0.93) at rest to poor
(0.35) in contraction. Inter-rater reliability was excellent (ICC > 0.75) at
rest on the right and left, in both groups. In contraction, it ranged from
moderate (ICC = 0.71) on the left in the group without migraine to excellent
(ICC > 0.75) in the other measurements. Low limits of agreement were
observed for the confidence intervals in all the measures. Conclusion: According to the confidence interval, low limits of
agreement were observed, regarding the reliability of ultrasonographic
measures of the longus colli muscle in women with
migraine.
Key-words: migraine
disorders, neck muscles, ultrasonography, reliability.
Introduction
Ultrasonography image processing is a noninvasive low-cost method
commonly used in clinical practice that analyzes muscle dimensions at rest and
in contraction [1,2], providing support for clinical
decisions [3,4]. For this reason, this method was used in a number of studies
to determine the association between the presence of chronic neck pain and
alterations in dimensions and neck muscle activation [5,6].
However, no studies were found until this moment assessing the reliability of
the data obtained from neck muscles of individuals with migraine using this
tool.
In this respect, evidence shows the involvement of peripheral nociceptive
stimuli in migraine pathogenesis. Nociceptive sensory stimuli from convergent afferences of a range of tissues, including tense and
painful muscles in the neck region, innervated by cervical nerve roots, could
contribute to activation of the trigeminovascular
inflammatory cascade [7,8] and trigger migraine [9].
From a biomechanical viewpoint, the deep neck flexor muscles, primarily
the long muscle of the head and the neck, play an important role in stabilizing
this segment. Thus, imbalances between these muscles and superficial neck
muscles make the spine less stable and more vulnerable to other balance forces
that act in maintaining posture, thereby generating overload in other muscles
[10] and consequently changes in muscle trophism.
Thus, the development of studies with the inclusion of ultrasound
evaluation is increasing. Despite the findings, and since it is an
operator-dependent assessment instrument whose results can vary in repeated
measures or with a change in examiner, it is necessary to assess the intra and
inter-rater reliability of this resource. Therefore, the present study aims to
determine the intra and inter-rater reliability of ultrasonographic
measures of the longus colli muscle in women with and
without migraine.
Methods
Design and study site
This cross-sectional study was conducted at the Department of
Physiotherapy of Universidade Federal de Pernambuco,
between March and December 2013, after approval was obtained from the Research
and Ethics Committee (CAAE: 02219412.5.0000.5208). The sample size was not
calculated because this is a pilot study. All participants gave their informed
consent, in accordance with resolution 466/12 of the National Research Ethics
Commission of the Ministry of Health.
Participants
The sample was composed of 20 female students from the Physiotherapy
Program at Universidade Federal de Pernambuco, aged
between 20 and 30 years, avoiding the biases related to the process of muscle
changes resulting from natural biological aging. Furthermore, only nulliparous
and nulligravida women were included in the sample,
once the existence of a relationship between hormones and the presence of
headache is well-established [11]. The women were diagnosed by a neurologist,
in accordance with International Classification of Headache Disorders, 2nd
edition criteria (2004) [12], and separated into a migraine and control group
(women without migraine).
The migraine group was composed of women with episodic migraine (less
than 15 days per month with headache), with the following characteristics: pure
migraine (with aura, without aura or both), whose pain has pulsed character,
unilateral location, intensity ranging from moderate severe, lasting 4-72
hours, that worsens with physical activity and may be associated with the
presence of nausea, photophobia or both and phonophobia.
The control group included participants diagnosed with other types of headache
or had intermittent headache attacks over their lifetime that
were not associated with features of migraine [12].
The following women were excluded: 1) body mass index ≥ 30,
because currently it is assumed obesity as a risk factor for triggering
migraine attacks [13]; 2) chronic migraine, chronic tension headache; chronic
neck pain; myopathies; fibromyalgia; abnormalities, fractures or history of
spinal or thoracic surgery; symptomatic herniated disc; rheumatoid arthritis;
history of spinal cord tumors; 3) score ≥ 15 on the Neck disability index
whose purpose is to assess the functionality of the cervical region and how
much pain this segment influence in carrying out daily activities. Their values
range from 0 (no disability) to 50 (full disability). Values above 15 represent
moderate disability [14]; 4) score ≥ 36 on the Beck depression inventory,
instrument whose purpose is to assess depressive symptoms in the population,
containing 21 items with scores ranging from 0 to 3 depending on the intensity
and maximum score of 63. Values represent ≥ 36 severe depression; 5)
score ≥ 30 on the Beck anxiety inventory, that is
a questionnaire composed of 21 questions related to common symptoms of anxiety
and a maximum score of 63. Values ≥ 30 indicate severe anxiety [15]. All
questionnaires present version adapted and validated for the Brazilian
population.
Procedures
Two examiners (1 and 2), blind to the diagnosis of headache, conducted ultrasonographic assessment of the
longus colli muscle. During data collection
participants could not be menstruating or using medication such as muscle
relaxants, painkillers or anti-inflammatories, in the 48 hours before the exam.
Ultrasonographic assessment
An Aloka 1500 ultrasound system with a 7.5 MHz
linear transducer was used. Images of the longus colli
muscle were obtained bilaterally, applying a gel between the transducer and the
skin. The transducer was positioned longitudinally in the anterior region of
the neck, parallel to the trachea, approximately 5 centimeters from the midline
and at the C5-C6 level [10], a position in which there is no overlap between
the longus colli and long head muscles [16]. In the
ultrasonography image the longus colli muscle is
bordered inferiorly and medially by the vertebral body, laterally by the
carotid artery, and superiorly by the retropharyngeal space [10].
Ultrasonography was performed with the participant in dorsal decubitus,
knees flexed, arms alongside the body and head positioned on the midline [6].
The B-mode was used to capture and measure the cross-sectional area (in cm2),
considered the greatest distance between the inner edge of muscle extremities,
without including facial contours in the measure [10].
Subjects were assessed by examiners 1 and 2, trained under the same
protocol and ultrasonographic measuring techniques.
For the inter- rater reliability study, three measures
of the cross-sectional area were obtained bilaterally, during rest and muscle
contraction, by examiner 1. Twenty minutes after conclusion of the test,
examiner 2 repeated the same procedure. For the intra- rater reliability study,
examiner 1 conducted a second assessment one week later, following the same
protocol, in order to decrease the possibility of data memorization.
Data processing and analysis
Using the SPSS Statistics Program, the Anova
test was applied at a 95% confidence level (p < 0.05). Analysis of inter and
intra-rater reliability was carried out using the intraclass
correlation coefficient (ICC). Values below 0.4 suggest poor reproducibility,
between 0.4 and 0.75 moderate reproducibility and above 0.75
excellent reproducibility [17]. Inter and intra-rater error was obtained
by the Bland Altman method, using the SigmaPlot
program and limits of agreement.
Results
In accordance with diagnosis of headache, 12 participants were assigned
to the migraine group, 10 of whom suffered from migraine without aura, one from
migraine with aura and another from migraine without aura and tension headache.
The control group was composed of women with episodic tension headache (n = 4)
and without primary headache (n = 4). The characteristics of the study
population are presented in Table I.
Table II shows that the dimensions of the longus colli
muscle did not differ between groups (p > 0.05).
Table III shows the intra-rater reliability of the longus colli muscle at rest and in contraction in the groups with
and without migraine. Excellent reliability (ICC > 0.75) was observed for
the right cross-sectional section, at rest and in contraction, in both groups.
The left side exhibited moderate reliability in the migraine group. In the
group without migraine, reliability was weak during contraction (ICC = 0.35)
and excellent at rest (ICC = 0.93).
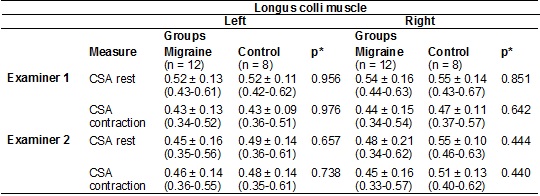
The results of inter-rater reliability are described in Table IV. At
rest, reliability was excellent on the right and left, in both groups (ICC >
0.75). However, during contraction reliability was moderate (ICC = 0.71) on the
left side in the group without migraine and excellent for the other measures.
The results of intra and inter-rater reliability are described in tables
III and IV. Low levels of agreement were observed in both analyses.
Table I - Characteristics of
participants.

*Anova. M ± SD/ IC (mean ± standard
deviation/confidence interval); m (meters); kg (kilograms); BMI (Body mass
index).
Table II - Intergroup analysis of the
cross-sectional area of the longus colli muscle
during rest and contraction.
*Anova. Data are expressed as M±SD/ IC (mean± standard deviation/ confidence
interval); CSA (cross sectional area - cm²).
Table III - Intra-rater reliability of the longus colli muscle cross-sectional area in women with and without
migraine. (see PDF).
Discussion
In this study, the intraclass correlation
coefficient was adequate, ranging from moderate to high. On the other hand, the
confidence intervals showed lower limits of agreement, based on the
Bland-Altman analysis. However, there is a lack of studies evaluating a priori
what are the limits that could be interpreted as acceptable.
The different methodologies used in the ultrasound evaluation of the
cervical muscles make comparisons between the studies limited. Many of them do
not present the agreement analysis values, only evaluating the intraclass correlation coefficient [18]. One study [5],
evaluating patients with chronic neck pain, corroborates our findings related
to the ICC analysis of the cross-sectional area of the longus colli muscle at rest (ICC in our study: 0.68 to 0, 93). The
results of this study [5] showed the ICC values ranging from 0.76 to 0.93,
indicating excellent reproducibility.
On the other hand, in our study the results of the limits of agreement
analysis were smaller. Similar findings were observed when assessing the
reliability and validity of ultrasonographic
measurements of the cross-sectional area of the long neck muscle in healthy
volunteers [16].
Given that it is an operator-dependent assessment, ultrasonography is
subject to bias, which may be one of the reasons for the low limits of
agreement observed in this study, especially inter-rater agreement. These
biases include equipment resolution, examiner training, accurate identification
of anatomic sites [1,19], levels of participant
adiposity [20] and a number of individual factors that can influence the
accuracy of the measures, such as adequate muscle relaxation [19].
Due to the complexity in obtaining ultrasonographic
images, even though the examiners received identical training to apply the
test, the fact that they were not specialists in image diagnosis may have
contributed to the low limits of agreement. It is probable that the reliability
of the measures potentially improves with the continuous practice of the
evaluators [4]. Furthermore, since it has been found that intra-rater
reliability is greater than inter-rater reliability, it is likely that
examiners will agree more with their own data in a same procedure than with
those of other examiners [21].
Another factor that could explain the low levels of intra-rater
reliability agreement in this study is participant stability. To control this
bias, during data collection subjects could not be menstruating or using
medication that might interfere in their mobility or the state of tension in
the cervical region. Nevertheless, after a one-week interval between the two
tests, factors such as the presence of pre-menstrual tension and acute neck
pain may have influenced the stability of participants and consequently the
different muscle measures.
On the other hand, a comparison between our findings and those of
another study [10] shows the use of reliability analysis without including
limits of agreement or calculating the reliability limits for the limits of
agreement. Moreover, a number of current studies report results based on
statistical significance, providing limited information on clinical relevance
[22]. This may represent a bias, since it forces a correlation which might in
fact not be true [23].
In addition, the differences in limits of agreement should be assessed
clinically [24,25]. A number of authors suggest that
an acceptable difference be established before the study [26]. In this respect,
despite the wide variation in limits of agreement, to date there are no studies
establishing a minimum important difference in neck muscle dimensions in
subjects with migraines and their healthy counterparts.
In the present study, the sample was composed of young adult women with
primary headache, while other studies analyzed older women (30 ± 6 years)
diagnosed with chronic neck pain. It is known that after the age of 30 years
there may be a progressive reduction in the cross-sectional area of the muscle
[27-29] as a result of the aging process. Furthermore, chronic neck pain may be
accompanied by muscular atrophy [30,31], possibly
explaining the differences between the findings of our study and suggesting
greater correlation between alterations in neck muscles and the process of pain
chronification, as occurs in the aging process or in
conditions such as chronic migraine and chronic neck pain, than in headache
pathogenesis.
One of the aims of a rapid assessment, harmless and inexpensive, such as
ultrasound, is the clinical applicability. Thus, our contribution is the use of
ultrasonography in the clinical examination of neck muscles, guiding
physiotherapeutic interventions in patients with headache. The study shows the
importance of determining a priori the magnitude of changes outside the limits
of the variability of measurement from the neck muscle in women with migraine.
It also reveals the need to establish the minimum significant difference in
neck muscles dimensions in individuals with and without migraine. Furthermore,
this is a pioneering study that analyzed the reliability of ultrasonographic
measures of neck muscles in individuals suffering from migraine, including the
limits of agreement.
This study has some limitations. Due to the necessity to control some
factors that could influence participant stability and, consequently, muscle
changes during the retest, it was not possible to get a sample with larger and
more homogeneous distribution between groups. The irregular distribution of the
sample between groups was due to difficulty in forming the control group based
on the criteria established in our methodology. Added to this, because it is a
pilot study analyzes interpretations are more restricted.
Conclusion
Low levels of agreement were observed in relation to inter and
intra-rater reliability of ultrasonographic measures
of the longus colli muscle in women with and without
migraine.
Referências
- Gellhorn AC, Carlson
MJ. Inter-rater,
intra-rater, and inter-machine reliability of quantitative ultrasound
measurements of the patellar tendon. Ultrasound
Med Biol 2013;39(5):791-6.
- Wanderley D, Moura
Filho AG, Costa Neto JJS, Siqueira GR, Oliveira DA. Analysis of dimensions, activation and median frequency of cervical
flexor muscles in young women with migraine or
tension-type headache. Brazilian J Phys Ther 2015;19(3):243-50.
- König N, Cassel M, Intziegianni K MF. Inter-rater reliability and measurement error of
sonographic muscle architecture assessments. J Ultrasound Med 2014;(33):769-77.
- McGaugh J, Ellison J. Intrasession and interrater reliability of rehabilitative
ultrasound imaging measures of the deep neck flexors: A pilot study. Physiother Theory Pract 2011;27(8):572-7.
- Javanshir K, Mohseni-Bandpei MA, Rezasoltani
A, Amiri M, Rahgozar M.
Ultrasonography of longus colli muscle: A reliability
study on healthy subjects and patients with chronic neck pain. J Bodyw Mov Ther 2011;15(1):50-6.
- Jesus-Moraleida FR,
Ferreira PH, Pereira LSM, Vasconcelos CM FM. Ultrasonographic analysis of the neck
flexor muscles in patients with chronic neck pain and changes after cervical
spine mobilization. J
Manip Physiol Ther 2011;34(8):514-24.
- Florencio LL,
Oliveira AS, Lemos TW, Carvalho GF, Dach F, Bigal ME et
al. Patients with chronic, but not episodic, migraine
display altered activity of their neck extensor muscles. J Electromyogr
Kinesiol 2016;30:66-72.
- Florencio LL, De
Oliveira AS, Carvalho GF, Tolentino GDA, Dach F, Bigal ME et
al. Cervical muscle strength and muscle coactivation during isometric contractions in patients with
migraine: A cross-sectional study. Headache 2015;55(10):1312-22.
- Calhoun AH, Ford S, Millen C, Finkel AG,
Truong Y, Nie Y. The prevalence of
neck pain in migraine. Headache 2010;50(8):1273-7.
- Javanshir K, Rezasoltani A, Mohseni-Bandpei
MA, Amiri M, Ortega-Santiago R, Fernández-de-Las-Peñas C. Ultrasound assessment of bilateral longus colli muscles in subjects with chronic bilateral neck pain.
Am J Phys Med Rehabil 2011;90(4):293-301.
- Pavlović JM, Allshouse AA, Santoro NF, Crawford SL, Thurston RC,
Neal-Perry GS et al. Sex hormones in women with and without migraine: Evidence
of migraine-specific hormone profiles. Neurology 2016;87(1):49-56.
- Headache Classification Committee of the International Headache Society. The international classification of headache disorderes. Cephalalgia 2004;24(1):8-160.
- Ornello R, Ripa P,
Pistoia F, Degan D, Tiseo C, Carolei A et al. Migraine and body mass index categories: a systematic review and
meta-analysis of observational studies. J Headache Pain 2015;16(1):27.
- Cook C, Richardson JK, Braga L, Menezes A, Soler
X, Kume P, et al. Cross-cultural adaptation and
validation of the Brazilian Portuguese version of the Neck Disability Index and
Neck Pain and Disability Scale. Spine 2006;31(14):1621-7.
- Beck AT, Epstein N, Brown G, Steer RA. An inventory for measuring clinical anxiety: psychometric properties. J
Consult Clin Psychol 1988;56(6):893-7.
- Cagnie B, Derese
E, Vandamme L, Verstraete
K, Cambier D, Danneels L.
Validity and reliability of ultrasonography for the longus colli
in asymptomatic subjects. Man Ther 2009;14(4):421-6.
- Fleiss JL, Levin BPM. Statistical methods for rates
and proportions. 3rd ed. New York: John
Wiley& Sons; 2003.
- Øverås CK, Myhrvold
BL, Røsok G, Magnesen E.
Musculoskeletal diagnostic ultrasound imaging for thickness measurement of four
principal muscles of the cervical spine - a reliability and agreement study. Chiropr Man Therap 2017;25(1):2.
- Gomes PSC, Meireles
CM, Leite SPMC. Confiabilidade da medida de espessuras musculares pela
ultrassonografia. Rev Bras Med Esporte
2010;16(1):41-5.
- Wagner DR. Ultrasound as a tool to assess body fat. J Obes 2013;2013:280713.
- Vincent-Smith B, Gibbons P. Inter-examiner and intra-examiner
reliability of the standing flexion test. Man Ther
1999;4(2):87-93.
- Armijo-Olivo S, Warren S, Fuentes J, Magee DJ. Clinical relevance vs. statistical significance: Using neck outcomes in
patients with temporomandibular disorders as an example. Man Ther 2011;16(6):563-72.
- Dewitte K, Fierens C, Stöckl D, Thienpont LM. Application of the Bland-Altman plot for
interpretation of method-comparison studies: a critical investigation of its
practice. Clin Chem 2002;48(5):799-801.
- Bland JM, Altman DG. Measuring agreement in method comparison studies. Stat
Methods Med Res 1999;8(2):135-60.
- Bland J, Altman D. Agreement between methods of measurement with
multiple observations per individual. J Pharm Stat 2007;17(4):571-82.
- Giavarina D. Understanding Bland Altman analysis. Biochem Medica 2015;25(2):141-51.
- Matsudo MS, Matsudo
VKR, Barros Neto TL. Impacto do envelhecimento nas variáveis antropométricas,
neuromotoras e metabólicas da aptidão física. Rev Bras Ciênc Mov 2000;8(4):21-32.
- Okada E, Matsumoto M,
Ichihara D, Chiba K, Toyama Y, Fujiwara H, et al. Cross-sectional area of posterior extensor muscles of the cervical spine
in asymptomatic subjects: A 10-year longitudinal magnetic resonance imaging
study. Eur
Spine J 2011;20(9):1567-73.
- Vernooij CA, Rao G,
Berton E, Retornaz F, Temprado J-J. The effect of
aging on muscular dynamics underlying movement patterns changes. Front Aging Neurosci 2016;8:1-12.
- Woodhouse A, Vasseljen O. Altered motor
control patterns in whiplash and chronic neck pain. BMC Musculoskelet
Disord 2008;9(1):90.
- Pauw R, Coppieters
I, Kregel J, De Meulemeester
K, Danneels L, Cagnie B.
Does muscle morphology change in chronic neck pain patients? A systematic review.
Man Ther 2016;22:42-9.