ARTIGO ORIGINAL
Relationship between the joint mobility index and the
presence of injury and pain among ballet students in Brazil
Relação entre o índice de mobilidade
articular e a presença de lesões e dor entre estudantes de balé no Brasil
Fernando Eduardo Zikan, PT, D.Sc.*
*Professor of Manual Therapy, Physiotherapy Department
– Faculty of Medicine, Federal University of Rio de Janeiro (UFRJ)
Recebido em 1 de outubro de 2018; aceito em 7 de janeiro de 2019.
Corresponding author adress: Prof. Dr. Fernando
Eduardo Zikan, Coordenação do Curso de Fisioterapia,
Faculdade de Medicina, Rua Professor Rodolpho Paulo Rocco, 255, 8º andar, Ala E,
Sala 03, Hospital Universitário Clementino Fraga Filho da UFRJ, Cidade Universitária,
Ilha do Fundão, 21941-913 Rio de Janeiro RJ, E-mail: fernandozikan@hucff.ufrj.br
Abstract
Dance is a unique blend of art and athleticism, which makes its
practitioners particularly susceptible to skeletal muscle injuries and pain.
Dancers are subjected to intense training, which contributes towards increasing
the severity of injury. Injuries occur significantly more frequently in
hypermobile dancers than in the non-hypermobile individuals. The present study
aimed to correlate the Joint Mobility Index, obtained through Carter and
Wilkinson’s Joint Mobility Scale, as modified by Beighton,
with the prevalence of musculoskeletal injuries among students at vocational
schools for classical ballet in Brazil, and to make a correlation with
self-reported presence of pain and muscle fatigue. This study indicates that
there is a real association between hypermobility as a risk factor for lesions,
which were more present in hypermobile individuals. On the other hand, pain was
inversely presented, such that it was more present in non-hypermobile dancers,
perhaps because of skeletal muscle overload to meet the physical and esthetic
needs of ballet. Fatigue was not an important variable in the analyses between
the groups, and was similar between them. It is especially important to
establish a relationship regarding the need for intensive therapeutic care for
treating of skeletal muscle injuries among hypermobile individuals.
Key-words: classical
ballet, musculoskeletal system, injuries, joint mobility index, physiotherapy.
Resumo
A dança é uma mistura
única de arte e performance, o que torna seus
praticantes particularmente suscetíveis a lesões e dores musculares
esqueléticas. Dançarinos são submetidos a treinamento intenso, o que contribui
para aumentar a gravidade da lesão. Lesões ocorrem significativamente mais
frequentemente em bailarinos hipermóveis do que nos
indivíduos não hipermóveis. O presente estudo teve
como objetivo correlacionar o Índice de Mobilidade Articular, obtido pela
escala de Carter e Wilkinson, conforme modificado por Beighton,
com a prevalência de lesões musculoesqueléticas entre os estudantes das escolas
profissionais de balé clássico no Brasil, e ainda correlacionar com o autorrelato da presença de dor e fadiga muscular. Este
estudo indica que existe uma associação real entre a hipermobilidade
como fator de risco para lesões, que estavam mais presentes em indivíduos hipermóveis. Por outro lado, a dor foi inversamente
apresentada, sendo mais presente nos bailarinos não hipermóveis,
talvez pela sobrecarga musculoesquelética para atender às necessidades físicas
e estéticas do balé. Fadiga não foi uma variável importante nas análises entre
os grupos, sendo semelhante entre eles. É especialmente importante estabelecer
uma relação com a necessidade de cuidados terapêuticos intensivos para lesões
musculares esqueléticas entre indivíduos hipermóveis.
Palavras-chave: balé clássico,
sistema musculoesquelético, lesões, índice de mobilidade articular,
Fisioterapia.
Introduction
For artists, their occupation is not just a way to earn a living: it is
their passion, and to fulfill this passion, they make great sacrifices, both
physically and mentally, to bring this immeasurable beauty into the world [1].
Dance is a unique blend of art and athleticism, which makes its
practitioners particularly susceptible to skeletal muscle injuries [2,3] and pain [4]. Dancers are subjected to intense training,
which contributes towards increasing the severity of injury and the possibility
of it becoming incapacitating [5], given the repetitive movements and the
exercises with excessive range of motion to which they are subjected [6].
One of the attributes for being good dancer, prescribed by Balanchine in
the twentieth century, is that in addition to having a lean and long body, the
individual should have a wide range of active and passive movement around the
hips, dexterity when the leg is in a high position and a high vertical jump. Wyon [7] further stated that flexibility is a vital
component of classical ballet.
Injuries occur significantly more frequently in hypermobile dancers than
in the non-hypermobile individuals [8]. Hypermobility is defined as the ability
to have the widest range of joint movement which allows a broader range and variety
of movements. In dancers’ profession, this is often promoted for esthetic
reasons inherent to dance, especially in classical ballet [9].
Joint hypermobility is a phenotypic characteristic shared by most, if
not all hereditary diseases of connective tissue, and there are abundant
reasons for demanding reliable and precise criteria for its competent
diagnosis. It is identified by using Beighton’s
nine-point scale, on which obtaining a score greater than four out of the total
of nine points constitutes as one of the major (primary) criteria for the
diagnosis [10-12]. Currently, it is the most commonly used test for identifying
and diagnosing Benign Joint Hypermobility Syndrome (BJHS) [13].
Hypermobility and BJHS are common both in general male and female
students and in dancers and professional dancers. Declining prevalence, and
more reports of arthralgia with other features of BJHS in young dancers,
suggests that BJHS may have a negative influence with important implications
for their training. The same pattern has not been observed in men, thus
suggesting that the reports of presence of pain and injuries relate to factors
other than BJHS [14].
The generalized joint laxity, also known as systemic joint laxity, was
defined by Boyle [15] as a condition in which synovial joints have a range of
movement beyond the normal limit. The potential consequence of this is
hypermobility syndrome. Some studies have reported an association between
generalized joint laxity and skeletal muscle complaints such as arthralgia,
joint subluxation, dislocation and sprains.
Steinberg [16] concluded in their study that dancers need to understand
that the range of passive movement, i.e. movements without voluntary muscle
contraction, will probably not increase with age. Therefore, the main objective
of a dance program should focus on exercises that maintain the natural
flexibility of the dancers’ joints, instead of trying to improve it and always
make gains. Maintenance of activities that aim to achieve excessive gains in
joint mobility may promote biomechanical changes such as twisting of the femur,
as identified by Hamilton [17], in excessive training to increase the range of
motion of passive external rotation of the hip.
Joint mobility in professional dancers was the reason for the study by Espelo [18], with the aim of correlating their changes with
the most frequent injuries among these professionals. Khan [19] found that the
dancers, when compared with a control group, showed a greater degree of joint
motion for external rotation movements and a smaller degree for internal
rotation movements of the hip. Another study along these lines was conducted by
Nilsson [20], who assessed the degree of mobility of the spine among first-year
students at the Swedish Ballet School. In comparison with a control group, they
had a higher rate of joint hypermobility.
Garrick [21] considered that dancing, and especially classical ballet,
was a career presenting risks. They reported that the practice of dancing promoted
a variety of damage due to "overuse". Thus, it would be important to
have specific treatment that included maintenance of good postural balance,
extreme flexibility and stretching, which are the minimum needs for proper
monitoring of dancers for injury prevention. Since hypermobility has been
associated with fatigue in the general population, hypermobile dancers need to
be careful, given the association between fatigue and etiology of injury in
dancing [9,22,23].
Gannon [11] and O'Loughlin [24] quantified
joint laxity of dancers and gymnasts, which is an aggravating factor for
injuries. These authors evaluated the range of motion of the dancers and
gymnasts and observed a large difference between the passive and active ranges
of motion, thus confirming that their samples presented a high degree of joint
instability, which explained their subjects’ propensity to injury.
Students with hypermobility require additional strength to accomplish
their training, which reflects the seriousness of the issue [25]. The most
commonly reported symptoms are instability and pain relating to tendinitis
[26], in which the need for joint stabilization leads to muscle overuse, thus
causing injuries and muscle fatigue [27].
The present study aimed to correlate the Joint Mobility Index, obtained
through Carter and Wilkinson’s Joint Mobility Scale, as modified by Beighton, with the prevalence of musculoskeletal injuries
among students at vocational schools for classical ballet in Brazil, and to
make a correlation with self-reported presence of pain and muscle fatigue.
Methods
This was a descriptive study using quantitative methodology, while
highlighting the epidemiological method. It was conducted in three schools that
have a recognized role in training professional dancers in Brazil. We used a
semi-open questionnaire that registered students’ information such as personal,
professional and social characteristics, physical assessment information
(anthropometric and morphofunctional data) and scores
on Carter and Wilkinson’s Joint Mobility Scale, as modified by Beighton.
This project was approved by the Research Ethics Committee of UFRJ and
each potential participant received an informed consent statement that they
could choose to agree or disagree with, regarding their participation in the
research, in accordance with CONEP Resolution 196/96.
Quantitative data were collected and analyzed using the SPSS software,
version 17.0, in which statistical tests (chi-square) were performed in order
to obtain data for discussion and for reaching conclusions.
Results
We evaluated 100 classical ballet students (70 girls and 30 boys), of
mean age 18 years (standard deviation 2.05). Of those 83% presented a level
greater than four on Carter and Wilkinson’s Joint Mobility Scale, as modified
by Beighton, and were therefore classified as
hypermobile according to the Brighton criteria: 90% of the girls and 67% of the
boys (p=0.004) which was a statistically significant difference (see Table I).
The mean for the Joint Mobility Index (JMI) was 5.58, with a standard deviation
of 2.09.
Table I – Joint mobility and gender.

Note:
p=0.004
Among the respondents classified as hypermobile (JMI ≥ 4), 78.3%
had injuries, versus 88.2% with injuries among the non-hypermobile individuals.
Although the percentage was higher in the latter group, there was no
statistically significant difference (p = 0.351). See Table II.
Table II - Hypermobility and injury.

Note:
p = 0.351
When the lesions were grouped into categories, according to the lesion
characteristics, the most common type was joint trauma resulting from
instability, such as sprains (24%), tendinitis (17.6%) and fractures (14.4%),
thus representing 56% of the lesions. Of these instability lesions, 88.5% were
among individuals classified as hypermobile. See Table III.
Table III – Types of injury and mobility.

Graph 1 (below) shows the distribution of the JMI according to the same
injury classification. Attention is drawn to the lower levels in the group
without instability group, albeit with great variability, and to the similarity
between the groups without injury and with unstable injuries. In the group with
both stable and unstable injuries, the distribution was greater than in the
group without instability and less than in the others, thus showing the sum
total of lesions with instability and lesions without instability.
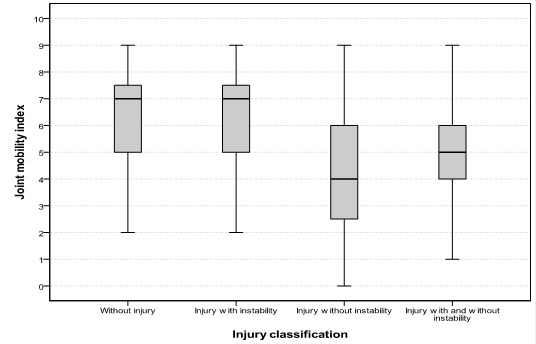
Graphic 1 – JMI and injury classification.
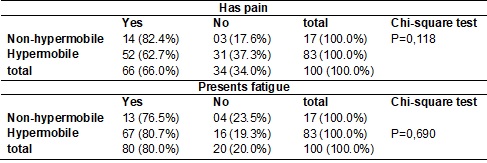
Among the interviewees, 66% reported having pain and of these, 82.4% did
not have hypermobility. The difference between the mobility groups was not
significant. The same was found with regard to the 80% who presented fatigue.
Fatigue was seen to be a little more frequent than pain: it was high in both
groups, without any difference between them. Although not statistically
significant, pain seemed to be a little more present in non-hypermobile
individuals (see Table IV).
Table IV – Joint mobility and pain/fatigue.
Discussion
Joint hypermobility has been shown to be an important factor in
evaluating injuries in dancers, and has been the purpose of several authors’
studies.
According to Stretanski [28], there is some
stigma in classical ballet, such as the notion that dancers are not real ballet
dancers unless they present extreme flexibility and hypermobility. In their
study on 377 dancers, only 4% of the professionals and 9% of the students were
considered to be hypermobile using Beighton's
modification of the Carter and Wilkinson method for evaluating joint
hypermobility.
This point of view is contrary to the study by McCormack [14], on students
and professional dancers at the Royal Ballet School, using the Beighton score, in which it was noted that hypermobility
and the syndrome are common in students and professional dancers. Moreover, Beighton [8] stated that injuries were significantly more
numerous among hypermobile dancers than among non-hypermobile dancers; and Day
[9] wrote: "Hypermobility ... among the dance profession is often promoted
for reasons ... inherent to dance, especially in classical ballet." In our
study, we saw that hypermobility was significantly present among our sample of
dancers: in 90% of girls and 67% boys, with is in line with the above mentioned
authors’ findings.
Hypermobility is more frequent among girls and has a negative influence
on their training, while among boys, the injuries and pain relate to factors
other than hypermobility [11,12,14].
Generalized joint laxity, which was defined by Boyle [15], has the
consequence of hypermobility syndrome. Some studies have reported that there is
an association between generalized joint laxity and skeletal muscle complaints
such as arthralgia, joint subluxation, dislocation and sprains.
When the injuries were grouped into categories based on their
characteristics, whether the source of the injury was instability or otherwise,
the results were different. Through this, the relationship between mobility and
the injury characteristics was clarified.
Gannon [11] and O'Loughlin [24] quantified the
joint laxity of dancers and gymnasts and confirmed that this population
presented a high degree of joint instability, which would explain their
propensity to injury. Students with hypermobility require additional strength
to accomplish their training, which reflects the seriousness of the issue [25,26]. The most commonly reported symptoms are instability
and pain relating to tendinitis, in which the need for joint stabilization
leads to muscle overuse, thereby causing injuries and muscle fatigue [2,6,22,27]. Ankle sprain injuries are the most common type
[23,24]. The most commonly reported symptoms are
lesions with instability and tendinitis [27].
Because hypermobility has been associated with fatigue in the general
population, hypermobile dancers need to be careful, given the association
between fatigue and the etiology of injury in dancing [9,23]. Hypermobility
among dancers may be present in as many as 44% of students. Its relationship
with fatigue should be a point for assessment in dealing with injuries among
dancers [3,9,11,23]. In our study, the muscle fatigue
data did not differ between the hypermobile and non-hypermobile groups, and
thus did not show any direct association.
Conclusion
This study points towards an association trend between joint
hypermobility and prevalence of skeletal muscle injuries, in line with the
findings from other authors who also identified high numbers of injuries among
individuals classified as hypermobile. This association became established when
we categorized the type of injury sustained and was not related to all types of
injury.
This study indicates that there is a real association between
hypermobility as a risk factor for lesions, which were more present in
hypermobile individuals. On the other hand, pain was inversely presented, such
that it was more present in non-hypermobile dancers, perhaps because of
skeletal muscle overload to meet the physical and esthetic needs of ballet.
Fatigue was not an important variable in the analyses between the groups, and
was similar between them.
The Beighton score, which is used in most
studies on dancers, may not provide an appropriate measurement of hypermobility
for this population. Therefore, there is a need for further studies on this
topic, thus confirming the hypothesis of Day.
It is our responsibility to take care of dancers in a broader manner,
and to inform them, as honestly as possible, about the state of their health
and of the possibility of monitoring, both for good development of their
activities and for therapeutic approaches. It is especially important to
establish a relationship regarding the need for intensive therapeutic care for
treating of skeletal muscle injuries among hypermobile individuals.
References
- Hansen PA, Reed K. Common musculoskeletal problems in the performing artist.
Phys Med Rehabil Clin N Am 2006;17(4):789-801. https://doi.org/10.1016/j.pmr.2006.08.001
- Smith TO, Medici A, Oduoza U, Hakim A, Paton B,
Retter G, Haddad FS, Macgregor A. National survey to evaluate
musculoskeletal health in retired professional ballet dancers in the United Kingdom. Phys Ther Sport 2017;23:82-85. https://doi.org/10.1016/j.ptsp.2016.07.009.
- Ekegren CL, Quested R, Brodrick A. Injuries in pre-professional ballet dancers: Incidence,
characteristics and consequences. J Sci Med Sport 2014;17(3):271-5. https:// doi.org/10.1016/j.jsams.2013.07.013.
- Hincapé CA, Morton EJ, Cassidy JD. Musculoskeletal injuries and pain in dancers: a systematic review. Arch Phys
Med Rehabil 2008;89(9):1819-29. https://doi.org/10.1016/j.apmr.2008.02.020
- Grego LG, Monteiro HL,
Gonçalves A, Aragon FF, Padovani CR. Agravos musculoesqueléticos em bailarinas clássicas,
não clássicas e praticantes de educação física. Arq Ciênc Saúde 2006;13(3):153-61.
- Sobrino FJ, Cuadra C, Guillén P. Overuse injuries
in professional ballet: injury-based differences among ballet disciplines. Orthop J Sports Med 2015;3(6):2325967115590114.https://doi.org/
10.1177/2325967115590114.
- Wyon MA, Nevill
AM, Dekker K, Brown DD , Clarke F, Pelly J, Koutedakis
Y. Effect of leg length on ROM, VJ and Leg Dexterity in dance. Int J Sports Med 2010;31:631-5.
- Beighton P. Hypermobility of joints. Fourth Edition. London: Springer; 2012.
- Day H, Koutedakis Y, Wyon
MA. Hypermobility and dance: a review. Int J Sports Med
2011;32(7):485-9. https://doi.org/10.1055/s-0031-1273690
- Grahame R. The need to take a fresh look at criteria for
hypermobility. J Rheumatol 2007;34(4):664-5.
- Gannon LM, Bird HA. The quantification of joint laxity
in dancers and gymnasts. J Sports Sci 1999;17(9):743-50. https://doi.org/10.1080/026404199365605
- Klemp P, Stevens JE, Isaacs S. A hypermobility study in ballet dancers. J Rheumatol 1984;11(5):692-6.
- Juul-Kristensen B, Rogind H, Jensen DV, Remvig
L. Inter-examiner reproducibility of tests and criteria for generalized joint hypermobility
and benign joint hypermobility syndrome. Rheumatology 2007;46:1835-41.
- McCormack M, Briggs J, Hakim A, Grahame R. Joint laxity and the benign joint
hypermobility syndrome in student and professional ballet dancers. J Rheumatol 2004;31(1):173-8.
- Boyle KL, Witt P, Riegger-Krugh C. Intrarater and interrater reliability
of the Beighton and Horan Joint Mobility Index. J Athl Train 2003;38(4):281-5.
- Steinberg N, Peleg S, Dar G, Masharawi Y, Heim M, Siev- Ner I. Range of joint movement in female dancers and nondancers aged 8 to 16 years: anatomical and clinical implications.
Am J Sports Med 2006;34(5):814-23.
- Hamilton D. Dance training intensity at 11-14 years is associated with femoral
torsion in classical ballet dancers. Br J Sports Med 2006;40(4):299-303. https://doi.org/10.1136/bjsm.2005.020941
- Espejo B. Amplitud de movimientos articulares en profesionales del ballet. Boletín de Rehabilitación Médica
1999;9(1):30-2.
- Khan K, Roberts P, Nattrass C, Bennell K, Mayes S, Way S et al. Hip and ankle range of motion
in elite classical ballet dancers and controls. Clin J
Sports Med 1997;7(3):174-9. https://doi.org/10.1097/00042752-199707000-00004
- Nilsson C, Leanderson J, Wykman
A, Strender LE. The injury panorama
in a Swedish professional ballet company. Knee Surgery Sports Traumatology
Arthroscopy 2001;9(4):242-6.
- Garrick JG, Lewis SL. Career hazards for the dancer. Occupational Medicine
2001;16(4):609-18.
- Smith TO, Davies L, Medici A, Hakim A, Haddad F, Macgregor A. Prevalence
and profile of musculoskeletal injuries in ballet dancers: A systematic review and
meta-analysis. Phys Ther Sport
2016;19:50-6. https://doi.org/10.1016/j.ptsp.2015.12.007.
- Hardaker WT, Erickson L, Myers
M. The pathogenesis of dance injury. In: Shell CG (ed): The dancer as athlete. Champaign,
IL: Human Kinetics; 1985. p. 91-4.
- O’Loughlin PF, Hodgkins CW, Kennedy JG. Ankle sprains and
instability in dancers. Clin Sports Med 2008;27(2):247-62. https://doi.org/10.1016/j.csm.2007.12.006
- Weiss DS, Rist RA, Grossman G. When can I start point work? Guidelines for initiating
pointe training. J Dance Med Sci 2009;13(3):90-2.
- Pollard-Smith T, Thomson OP. Professional ballet dancers' experience of injury
and osteopathic treatment in the UK: A qualitative study. J Bodyw
Mov Ther 2017;21(1):148-156. https://doi.org/10.1016/j.jbmt.2016.06.009.
- Ritter S, Moore M. The
relationship between lateral ankle sprain and ankle tendinitis in ballet dancers.
J Dance Med Sci 2008;12(1):23-31.
- Stretanski M, Weber G. Medical and Rehabilitation issues in classical ballet. Am J Phys Med Rehabil
2002;81(5):383-91. https://doi.org/10.1097/00002060-200205000-00013