Fisioter Bras.
2023;24:(5):519-31
ORIGINAL ARTICLE
Acute effect of open and closed kinetic chain training
on lower limb muscle strength in young adults
Efeito
agudo de um treino em cadeia cinética aberta e fechada na força muscular de
membros inferiores em adultos jovens
Carlos Brendo Ferreira Reis, Gabrielle Lopes Teixeira, Matheus
Jonas Santos, Leonardo Araújo Vieira, Natalia Madalena Rinaldi
Universidade
Federal do Espírito Santo, Vitória, ES, Brasil
Received: March18, 2022; Accepted: August 20, 2023.
Correspondence: Natalia Madalena Rinaldi, natalia.rinaldi@ufes.br
How to cite
Reis CBF, Teixeira GL, Santos MJ, Vieira LA, Rinaldi NM. Acute effect of open and closed kinetic chain training on lower limb muscle strength in young adults. Fisioter Bras. 2023;24(5):519-31. doi: 10.33233/fb.v24i5.5131
Resumo
Dentre
as variações de prescrição de treinamento para melhoria da força muscular,
podemos destacar os exercícios de cadeia cinética aberta (CCA) e cadeia
cinética fechada (CCF). O objetivo deste estudo foi investigar o efeito agudo
dos exercícios em CCA e CCF na força muscular de membros inferiores em adultos
jovens. Dez adultos jovens sedentários foram convidados a participar de um
treinamento agudo composto por três exercícios em CCA e três exercícios em CCF
e realizaram três séries de dez repetições. Para avaliar o torque e a potência
muscular foram utilizados um dinamômetro isocinético
e uma plataforma de força. As variáveis analisadas foram: pico de torque, tempo
para pico de torque, potência média e potência média. Análises univariadas foram utilizadas para comparar o desempenho dos
participantes nos exercícios em CCA e CCF nos testes de torque e potência. O
pico de torque foi maior nos movimentos extensor e flexão plantar do que nas
articulações do joelho e tornozelo, respectivamente. Ao comparar os exercícios
em CCA e CCF, os exercícios CCA produziram maior pico de torque e potência
média em todas as articulações do que CCF. Concluímos que os exercícios em CCA
podem ser usados para melhorar a força em adultos jovens.
Palavras-chave: treino agudo; cadeia cinética aberta;
cadeia cinética fechada; torque; potência.
Abstract
Among training prescription variations for improving
muscle strength, we can highlight open kinetic chain (OKC) and closed kinetic
chain (CKC) exercises. The aim of this study was to investigate the acute
effect of OKC and CKC exercises on lower limb muscle strength in young adults.
Subjects were invited to participate in an acute training consisting of three
OKC exercises and three CKC exercises and performed three sets of ten
repetitions. To evaluate the torque and muscle power, an isokinetic dynamometer
and a force platform were used. The analyzed variables were: peak of torque,
time to peak torque, mean power and average power. Univariate analyses were
used to compare the performance of participants in OKC and CKC exercises in
torque and power tests. Peak torque was higher in the extensor and plantar
flexion movements than knee and ankle joints, respectively. When comparing OKC
and CKC exercises, OKC exercises produced a higher peak of torque and mean
power in all the joints than CKC. We concluded that OKC exercises can be used
for improving strength in young adults.
Keywords: acute training; open kinetic
chain; closed kinetic chain; torque; power.
Introduction
Skeletal muscle is a dynamic tissue
sensitive to acute and chronic adaptations promote by exercise. Closed and open
kinetic chain exercises should be considered in exercise prescription, once
there is a variation in muscle recruitment and joint moment patterns between
these types of exercise [1]. Although, there is no yet consensus on the
definition and use of the terms open and closed kinetic chain [2]. Closed
Kinetic Chain (CKC) exercises can be characterized by multi-joint movements
performed with the distal segment supported on a solid surface and supported by
body weight [1,3,4,5]. Open kinetic chain (OKC) exercises can be characterized
by single joint movements distal segment of the body being free to move in
space and not supporting body weight [1,3,5]. The difference between CKC and
OKC exercises has been constantly studied in the context of resistance training
(RT) and rehabilitation [1,5,6,7].
In rehabilitation context, the
difference between OKC and CKC exercises in different clinical cases is
discussed, such as after anterior cruciate ligament (ACL) reconstruction
[5,8,9], osteoarthritis [3] and patellar chondropathy
[4]. OKC exercises are usually prescribed after the inflammation period,
without additional external load or isometric exercise to minimize muscle
atrophy. CKC exercises are often applied for their functionality in daily life
and sports activities that improve balance, proprioception, muscle
co-contraction, q-angle reduction, joint crackling, pain sensation, increased
strength and muscle circumference [3,4,8]. Therefore, in rehabilitation CKC
exercises decrease the risks of shear forces, increases proprioception, muscle
coordination, joint stability and appears to be clinically safer than OKC
exercises [6].
However, the effect of OKC and CKC
exercises in RT program on muscle function performance in healthy subjects is
not totally clear. Augustsson et al. [10]
investigated the chronic effect of RT with CKC vs. OKC exercises on
3-repetition maximum (3-rm) test performance, isokinetic strength and vertical
jump. The results revelated significant improvement in the 3-rm test in both
groups, but the group that performed CKC exercise showed a greater increase
when compared to the OKC group, 31% vs. 13% respectively. For the vertical jump
test, only the CKC group showed a significant improvement, with an increase of
10% (5 cm) in the height of vertical jump. However, no significant improvement
was observed in isokinetic tests after six weeks in both groups. Yet, CKC
strength exercises of extensor lower limbs are more highly related to jumping
performance than exercises in OKC [11] and provide more simultaneous activity
in the different portions of the quadriceps muscle than OKC, with earlier onset
and greater amplitude of electromyography (EMG) activity in vastus medialis
obliquus [12]. In addition, OKC and CKC exercises promote an increase on the
overall thickness of quadriceps muscles, as an acute effect of the exercises.
However, quadriceps muscles can be selectively improved depending on the type
of the exercise, with a greatest increase on the thickness of vastus
intermedius and vastus medialis oblique, respectively in OKC and CKC exercises
[13]. Thus, it seems that CKC and OKC exercises promote different neural and
muscle adaptations, with a better coordination of muscle recruitment in CKC,
which result in a better performance of muscle function tests when compare to
OKC exercises.
Moreover, potentiation and fatigue
are coexistence acute process related from prior muscle activation [14], and
are determined by the interaction of several factors like individual
characteristics and parameters related to the exercise prescription [15].
Post-activation potentiation (pap) is the post-contraction increase in force
production, and voluntary pap refers to the increase in muscular force
production during a voluntary contraction. Previous works have already revealed
improvement in muscle function performance as acute effect related to pap
promoted by CKC exercises, with an increase of the height of vertical jump
tests and peak power output in healthy adults [16] and in the height of
vertical jump performance in athletes [17]. However, other studies revealed
that muscle damage and fatigue induce by exercise is an acute effect that promote
a decrease in muscle strength and on the performance of vertical jump tests
[18,19,20]. Thus, the acute effect of CKC and OKC exercise in muscle function
performance should be considered in RT program. In addition, CKC exercises
involve co-contraction of agonist, antagonist and synergistic muscle of
multiple joints, while OKC enable isolate specific muscle group during the
exercises [1,2]. Thus, CKC and OKC possibly induce different adaptations in
agonist and antagonist muscle and also in dominant and non-dominant limbs.
In this context, there is a need
for further studies that investigate the acute effect of CKC and OKC exercises
on muscle function performance, with an analysis on the peak of torque, time to
peak torque and muscle power of lower limbs in healthy subjects, providing
insights for better and safer RT prescription aiming performance and injuries
prevention and rehabilitation. Also, it is important to analyze asymmetry on
muscle function performance of dominant and non-dominant lower limbs and on
agonist and antagonist muscles. Thus, the aim of this study was threefold 1)
investigate the acute effect of OKC and CKC exercises on lower limb muscle
strength in young adults; 2) investigate the acute effect of OKC and CKC
exercises on muscle torque and power of dominant and non-dominant lower limbs;
3) investigate the acute effect of OKC and CKC exercises on muscle torque and
power of flexion and extension of hip, knee and ankle. Our hypothesis was: 1)
muscle torque and power in CKC is greater than OKC; 2) no difference in muscle
torque and power will be observed between dominant and non-dominant limbs; 3)
extensor muscles of hip, knee and ankle will reveal higher values of muscle
torque and power when compared to flexor muscles.
Methods
Participants
This is a cross-sectional study
with healthy male young adults, aged between 18 and 25 years. The exclusion
criteria were: history of musculoskeletal injuries in lower extremities in the
6 months preceding the experiment and obesity (body mass index above 30). The
research study was approved by the Research Ethics Committee of Universidade Federal do Espírito
Santo (process number 2.598.751). After agreeing to participate in the study,
the participants signed a consent form according to the rules established by
the resolution number 466/2012 of the National Health Council of Brazil.
Procedures
Data collection was carried out in
six days. In the first day, an anamnesis was performed to obtain
sociodemographic information, health status and physical activity level with baecke questionnaire [21]. Also, in the first day, an
anthropometric evaluation and lower limb muscle function assessment with
isokinetic and jump test were performed to collect pre-training data. In the
second visit in the laboratory, participants were familiarized with the testing
procedure, performing two CKC sessions (back squat, sumo deadlift, and seated
calf raise) and two OKC sessions (leg extension, lying leg curl, ankle
dorsiflexion). The familiarization protocol consists of one set of fifteen
repetitions, with 1-minute rest and muscle contraction phases of two seconds in
concentric and two seconds in eccentric. The 1-rm test and re-test were
performed in the third e fourth visit to the laboratory, respectively 24 and 72
hours after the familiarization session. After the maximum load determination
test, the CKC and OKC rt sessions were performed respectively in the fifth and
sixth day, with a 48-hour interval between sessions of training (figure 1).
During the OKC and CKC sessions of rt, three sets of ten repetitions were
performed, with 2 seconds of muscle contraction per each phase (60% of 1-rm)
and one-minute interval between sets and exercises. Moreover, five minutes
after both sessions, lower limb muscle function assessment were realized with
isokinetic and jump tests.
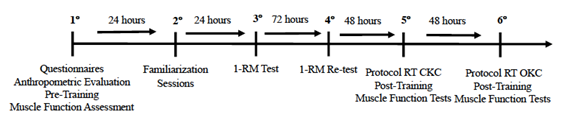
Figure 1 - Schematic representation of
the study
Experimental tasks
One-repetition maximum test (1rm)
Initially a warm up session, consisted of 5-10 repetitions with 40% of predicted 1rm, was realized. After a 1-minute rest, participants performed 3-5 repetitions with 60% of predicted 1rm. Two minutes after warm up, up to 5 attempts of the 1-rm protocol were applied with 5 minutes rest between attempts and 10 minutes between exercises (OKC protocol: leg extension, lying leg curl, ankle dorsiflexion; CKC protocol: back squat, sumo deadlift and seated calf raise). Re-test was performed 72 hours later. All 1rm measurements were reported in kilograms for subsequent data analysis [22,23].
Isokinetic dynamometer assessment
Isokinetic tests were realized with
a biodex system 4 dynamometer (Biodex
Medical Systems, Inc., Shirley, NY, USA). The flexion and extension movements
of the hips, knees and ankles were evaluated. After experimental instructions,
participants were familiarized with the procedure by performing five
repetitions in each velocity with submaximal contractions. The test consisted
of concentric isokinetic contractions with predetermined angular velocity. For
all joints, five repetitions were executed at 60°/s and 10 repetitions at
180°/s with 1 minute of rest between different velocities assessments.
Participants were verbally encouraged to develop maximal contraction during
test. All assessments were performed on both right and left sides, starting
with the dominant limb (defined as the limb used to kick a ball). The
positioning, stabilization, calibration and gravity correction procedures were
performed according to the manufacturer's recommendations.
Jump assessments
Participants were positioned on a
force plate (Biomec400, Emg System of Brazil, Ltda.,
SP) sampled at 100 hz and filtered with a 10 hz low pass to perform the vertical counter-movement jump (CMJ). Participants were instructed to jump with their hands
on the waist while avoiding bending the legs during flight. Moreover,
participants performed three CMJ on the force plate with two-minutes rest
intervals. The average power was calculated by Emglab
Software (emg system). The takeoff time, in which the
foot detached from the ground, and the time of impact were initially identified
through the vertical ground reaction force component. In this period, the
average power was calculated based on body weight, flight time and ground force
reaction.
Experimental tasks (isokinetic
protocol and counter-movement jump) were performed in separate blocks and
counterbalanced within the participants.
Dependent variables
The dependent variable used to
evaluate lower limb muscle function performance were the peak of torque and
time to peak torque at 60°/s and mean power at 180°/s in the isokinetic test
and the average power at jump test.
Statistical analysis
Data are presented as mean ± sd.
All statistical analyses were conducted using SPSS version 19.0 software (Spss Inc., Chicago, Il, USA). The normality and variance
homogeneity were assessed with Shapiro-Wilk test and the Levene
test, respectively. The data presented normal distribution. Thus, three-way anovas (moment [pre-sessions, OKC, CKC] x movement,
[flexion, extension] x limb [dominant, non-dominant]) were carried out as
repeated measures for peak of torque, time to peak torque and mean power
isokinetic variables in each joint (hip, knee and ankle). Furthermore, One-Way Anova (moment [pre-session, OKC, CKC]) was carried out as a
repeated measure for average power variable (jumps - force plate data). Post
hoc tests with Bonferroni adjustments were performed for main and interaction
effects. The significance level was set at p ≤ 0.05.
Results
A total of
10 inactive college men participated in this study, nine participants were
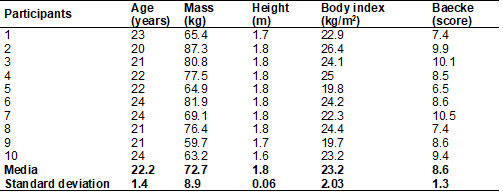
right-handed and one was left-handed. Table I presents the clinical and
anthropometric characteristics of the sample.
Table I - Clinical and anthropometric characteristics
of the sample
Isokinetic dynamometer data
Hip joint
Three-way anova
showed a moment effect (f2,18 = 6.05, p = 0.011) for the right limb. The mean
power was higher after OKC (182.63 w) compared to CKC (144.89 w) exercises for
hip extension and flexion movements (figure 2f).
Knee joint
Three-way Anova
revealed significant movement effect (f1.9 = 292.20, p ≤ 0.001) for the
right and left limbs. Participants had a higher peak of torque (figure 2a) in
the extension (right = 244.23n/m, left = 211.92n/m) compared to flexion
movement (right = 119.83n/m, left = 101.87n/m). However, the interaction effect
between movement and moment (f2,18 = 11.10, p = 0.002) showed that mean power
was greater in OKC (253.63 w) than CKC (225.81 w) in left knee extension
movement (figure 2c).
Ankle joint
Three-way anova
showed movement effect (f1.9 = 39.21, p ≤ 0.001) for the right lower
limb. The data showed a higher peak torque (figure 2g) in the plantar flexion
(74.35n/m) compared to the dorsiflexion movement (30.95n/m). However, for the
left ankle joint, it was revealed a moment effect (f2,18 = 6.47, p = 0.008),
with a greater time to peak torque in pre-session (292 ms)
compared to OKC (239.5 ms) for plantar flexion and
dorsiflexion movements (figure 2h).
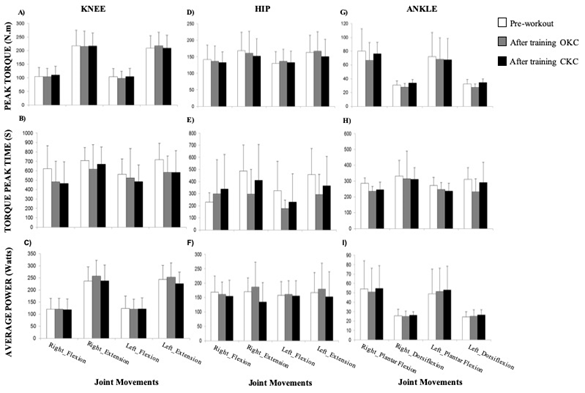
Figure 2 - Mean and standard deviation
of the following variables: peak of torque, time to peak torque and mean power
for knee (a-c), hip (d-f) and ankle (g-i) joints at
pre-training, OKC and CKC
Force plate data
The mean power (jumps) did not
present significant statistical differences (f2,18 = 2.98, p = 0.94) among the
interventions (pre-sessions, OKC and CKC) (figure 3).
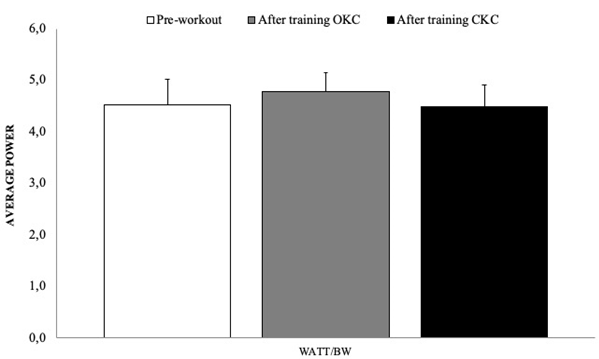
Figure 3 - Mean and standard deviation
of the average power variable evaluated in the force plate at the pre-training,
OKC and CKC moments
Discussion
The present study aimed at comparing the
acute effect of rt in OKC and CKC exercises on lower limbs (hip, knee, and
ankle joint) torque production and muscle power. The results of the present
study showed: 1) OKC exercises generate higher peak torque and power in all
joints compared to CKC, 2) for the knee and hip joints, exercises in OKC raised
the average power of the evaluated members compared to exercises in CKC, and 3)
for ankle joint, the time to peak torque after OKC exercise decreased compared
to baseline data. In relation to the hypothesis of the study, it was expected
that CKC exercises would generate greater torque and muscle power than OKC
exercises, which was not found by the results.
Assessments on the isokinetic
dynamometer were performed bilaterally on the lower limbs and no differences
were revealed between dominant and non-dominant lower limbs for the effect of
movement (flexion and extension). However, the bilateral comparison between
flexors and extensors may show some difference, being considered normal in
values of 10% between dominant and non-dominant lower limbs [24]. Moreover, the
results showed an increase for peak torque variable when comparing knee flexion
and extension movements and ankle plantar flexion and dorsiflexion. For the
knee joint, it was observed that the extension movement had higher peak torque
compared to the flexion movement. In agreement with previous studies that
demonstrate that knee extensor muscles are stronger than the flexors in the
entire range of motion, regardless of age, sex, angular speed and training
modality [25,26]. For the ankle joint, the results showed that plantar flexion
movement had a higher peak torque compared to dorsiflexion movement, which
agrees with Woodson et al. [27]. These authors observed that plantar
flexors have greater capacity for generating strength than ankle dorsiflexors.
In addition, exercises that work the ankle joint muscles favor the ones linked
to the plantar flexion movement over the dorsiflexion movement.
In rehabilitation, studies showed
that OKC exercises improve the strength of specific muscles, but when applied
isolated, they are not advantageous for musculoskeletal rehabilitation after
injuries, requiring a combination with CKC exercises. Tagesson
et al. [7] showed that in the isokinetic test after rehabilitation, OKC
exercise was more effective than CKC exercise in recovering quadriceps muscle
strength. In addition, Mikkelsen et al. [28] recommends that the
quadriceps needs training in OKC exercises to recover
muscle torque and that this type of exercise helps restore total muscle
function. However, CKC exercises distribute muscle work in the rehabilitation
process, avoiding overloading the injured joints, allow functional movement
patterns, provide isometric, concentric and eccentric contractions in several
planes, providing greater stability to the joints in addition to stimulating
proprioception and decrease shear forces [6,8].
In this sense, acute OKC exercises
are more effective for torque production and muscle power output in healthy
young adults without injuries, as this type of exercise recruits
muscles individually, prioritizing muscle groups of a single joint (e.g: knee, hip, and or ankle) and increasing functional
muscle strength. CKC exercises are more efficient for improving motor
coordination, proprioception and joint stability. The vertical jumps results
confirm the statements above, as they did not show an increase in the average
power after the CKC exercises in comparison with the isokinetic dynamometer,
which in its evaluation analyzes only OKC exercises.
As a limitation of the study, an
insufficient load was observed for some OKC exercise machines. Despite this
limitation, the participants used the maximum load on this equipment and had a
greater significant result compared to the CKC exercises, which had a higher
total volume. Another possible limitation was that the sequence of RT training
in CKC and OKC was not randomized between the participants, what could have
promoted different effects on motor learning. Given the above, it is evident
the need for future studies to better investigate the comparison between OKC
and CKC exercises training in the torque production and muscle power in young
and healthy individuals without muscle and joint problems.
Conclusion
Acute OKC exercises are more
efficient in producing torque and muscle power for all evaluated joints in
young adults. Thus, the acute OKC exercises are more appropriate for future
interventions with the proposal of improving strength in healthy young adults
without musculoskeletal injury.
Conflito
de interesses
Os
autores negam conflitos de interesses.
Fontes
de financiamento
Não
houve fonte financiadora
Contribuições
dos autores
Concepção
e desenho da pesquisa:
Rinaldi NM, Reis CBF, Teixeira GL, Santos JM; Obtenção de dados:
Teixeira GL, Santos JM, Reis CBF; Análise e interpretação dos dados:
Rinaldi NM, Vieira LA; Análise estatística: Rinaldi NM; Redação do
manuscrito: Reis CBF, Vieira LA; Rinaldi NM; Revisão crítica do
manuscrito quanto ao conteúdo intelectual importante: Rinaldi NM
References
- Karandikar N, Vargas OOO. Kinetic chains:
a review of the concept and its clinical applications. PMR 2011; 8(3): 739–745. doi: 10.1016/j.pmrj.2011.02.021 [Crossref]
- Mayer F, Schlumberger A, Van Cingel R, Henrotin Y, Laube W, Schmidtbleicher D. Training and testing in open versus closed kinetic chain. Isokinet Exerc Sci. 2003;11(4):181–7. doi: 10.3233/ies-2003-0154 [Crossref]
- Vad V, Hong Hm, Zazzali M, Agi N, Basrai D. Exercise recommendations in athletes with early osteoarthritis of the knee. Sport Med. 2002;32(11):729–39. doi: 10.2165/00007256-200232110-00004 [Crossref]
- Bakhtiary AH, Fatemi E. Open versus closed kinetic chain exercises for patellar chondromalacia. Br J Sports Med. 2008;42(2):99–102. doi: 10.1136/bjsm.2007.038109 [Crossref]
- Jewiss D, Ostman C, Smart N. Open versus closed kinetic chain exercises following an anterior cruciate ligament reconstruction: a systematic review and meta-analysis. J Sports Med. 2017;4721548:1–10. doi: 10.1155/2017/4721548 [Crossref]
- Bunton EE, Pitney WA, Cappaert
TA, Kane AW. The role of limb torque, muscle action and proprioception during
closed kinetic chain rehabilitation of the lower extremity. J Athl Train. 1993 [Internet];28(1):10–20. [cited 2023 oct 8].
Available from: https://pubmed.ncbi.nlm.nih.gov/16558197/
- Tagesson S, Öberg B, Good L, Kvist J. A comprehensive rehabilitation program with quadriceps strengthening in closed versus open kinetic chain exercise in patients with anterior cruciate ligament deficiency: a randomized clinical trial evaluating dynamic tibial translation and muscle function. Am J Sports Med. 2008;36(2):298–307. doi: 10.1177/0363546507307867 [Crossref]
- Uçar M, Koca I, Eroglu M, Eroglu S, Sarp U, Arik Ho, Yetisgin A. Evaluation of open and closed kinetic chain exercises in rehabilitation following anterior cruciate ligament reconstruction. J Phys Ther Sci. 2014;26(12):1875–8. doi: 10.1589/jpts.26.1875 [Crossref]
- Perriman A, Leahy E, Semciw Ai. The effect of open-versus closed-kinetic-chain exercises on anterior tibial laxity, strength, and function following anterior cruciate ligament reconstruction: a systematic review and meta-analysis. J Orthop Sports Phys Ther. 2018;48(7):552–66. doi: 10.2519/jospt.2018.7656 [Crossref]
- Augustsson J, Esko A, Thomeé R, Svantesson U. Weight training of the thigh muscles using closed vs. open kinetic chain exercises: a comparison of performance enhancement. J Orthop. Sports Phys Ther. 1998;27(1):3–8. doi: 10.2519/jospt.1998.27.1.3 [Crossref]
- Blackburn JR, Morrissey Mc. Relationship between open and closed kinetic chain strength of the lower limb and jumping performance. J. Orthop. Sports Phys Ther. 1998; 27(6), 430–35. doi: 10.2519/jospt.1998.27.6.430 [Crossref]
- Stensdotter AK, Hodges PW, Mellor R, Sundelin G, Häger-Ross C. Quadriceps activation in closed and in open kinetic chain exercise. Med Sci Sports Exerc. 2003;35(12):2043–47. doi: 10.1249/01.mss.0000099107.03704.ae [Crossref]
- Cheon S, Lee JH, Jun HP, An Yw, Chang E. Acute effects of open kinetic chain exercise versus those of closed kinetic chain exercise on quadriceps muscle thickness in healthy adults. Int J Environ Res Public Health. 2020;17(13):1–11. doi: 10.3390/ijerph17134669 [Crossref]
- Rassier DE, Macintosh BR. Coexistence of potentiation and fatigue in skeletal muscle. Brazilian J Med Biol Res. 2000;33(5):499-508. doi: 10.1590/s0100-879x2000000500003 [Crossref]
- Tillin N, Bishop DJ. Factors modulating post-activation potentiation and its effects on performance. Sport Med. 2009;39(2):147–66. doi: 10.2165/00007256-200939020-00004 [Crossref]
- Bauer P, Sansone P, Mitter B, Makivic B, Seitz Lb, Tschan H. Acute effects of back squats on countermovement jump performance across multiple sets of a contrast training protocol in resistance-trained men. J Strength Cond Res. 2019; 33(4): 995–1000. doi: 10.1519/jsc.0000000000002422 [Crossref]
- Crewther BT, Kilduff LP, Cook CJ, Middleton MK, Bunce PJ, Yang Gz. The acute potentiating effects of back squats on athlete performance. J Strength Cond Res. 2011;25(12):3319–25. doi: 10.1519/jsc.0b013e318215f560 [Crossref]
- Byrne C, Eston R. The effect of exercise-induced muscle damage on isometric and dynamic knee extensor strength and vertical jump performance. J Sports Sci. 2002;20(5):417–25. doi: 10.1080/026404102317366672 [Crossref]
- Byrne C, Twist C, Eston R. Neuromuscular function after exercise-induced muscle damage. Sport Med. 2004;34(1):49–69. doi: 10.2165/00007256-200434010-00005 [Crossref]
- Skurvydas A, Brazaitis M, Kamandulis S. Muscle-damaging exercise affects isokinetic torque more at short muscle length. J Strength Cond Res. 2011;25(5): 1400–6. doi: 10.1519/jsc.0b013e3181d685a0 [Crossref]
- Sadeghisani M, Manshadi FD, Azimi H, Montazeri A. Validity and reliability of the persian version of baecke habitual physical activity questionnaire in healthy subjects. Asian J Sports Med. 2016;7(3):e31778. doi: 10.5812/asjsm.31778 [Crossref]
- Simão R, Farinatti PTV, Polito MD, Maior AS, Fleck SJ. Influence of exercise order on the number of repetitions performed and perceived exertion during resistance exercises. J Strength Cond Res. 2005;19(1):152–6. doi: 10.1519/1533-4287(2005)19<152:ioeoot>2.0.co;2 [Crossref]
- Haff G, Triplett NT
(2016). Essentials of strength training and conditioning. Fourth edition.
Champaign, Il: Human Kinetics; 2016.
- Kannus P. Isokinetic evaluation of muscular performance. Int J Sports Med. 1994;15:s11–s18. doi: 10.1055/s-2007-1021104 [Crossref]
- Yoon TS, Park DS, Kang SW, Chun SI, Shin JS. Isometric and isokinetic torque curves at the knee joint.. Yonsei Med J. 1991;32(1):33–43. doi: 10.3349/ymj.1991.32.1.33 [Crossref]
- Andrade MS, Lira CAB, Koffes FC, Mascarin NC, Benedito-Silva AA, Silva AC. Isokinetic hamstrings-to-quadriceps peak torque ratio: the influence of sport modality, gender, and angular velocity. J Sports Sci. 2012;30(6):547–53. doi: 10.1080/02640414.2011.644249 [Crossref]
- Woodson C, Bandy WD, Curis D, Baldwin D. Relationship of isokinetic peak torque with work and power for ankle plantar flexion and dorsiflexion. J Orthop Sports Phys Ther. 1995;22(3):113–5. doi: 10.2519/jospt.1995.22.3.113 [Crossref]
- Mikkelsen C, Werner S, Eriksson E. Closed kinetic chain alone compared to combined open and closed kinetic chain exercises for quadriceps strengthening after anterior cruciate ligament reconstruction with respect to return to sports: a prospective matched follow-up study. Knee Surgery Sport Traumatol Arthrosc. 2000;8(6):337–42. doi: 10.1007/s001670000143 [Crossref]
