Fisioter Bras.
2023;24(3):265-73
ORIGINAL ARTICLE
Self-reported rheumatic disease and presence of pain
in elderly in the countryside of Amazonas/Brazil
Doença
reumática autorreferida e presença de dor em idosos
no interior do Amazonas/Brasil
Yandra Alves Prestes1, Geuziane Souza da Silva1, Johrdy
Amilton da Costa Braga1, Maria Helena Ribeiro De Checchi3,
Elisa Brosina de Leon2, Hércules Lázaro
Morais Campos1
1Universidade Federal do Amazonas, Coari,
AM, Brazil
2Universidade Federal do Amazonas,
Manaus, AM, Brazil
Received: 2022 October 4th; Accepted: 2023 January
12th
Correspondência: Hércules Lázaro Morais Campos,
herculeslmc@hotmail.com
How to cite
Prestes YA, Silva GS, Braga JAC, MChecchi MHR, Leon EB, Campos HLM. Self-reported rheumatic
disease and presence of pain in elderly in the countryside of Amazonas/Brazil. Fisioter Bras. 2023;24(3):265-73. doi:
10.33233/fb.v24i3.5306
Abstract
Introduction: The presence
of self-reported rheumatic disease and pain in older adults from the countryside
of Amazonas state was identified and described. Methods: We visited 131
elderly residents of Amazonas, using the Functional Comorbidities Index to
track the presence of self-reported diseases, and, to assess pain, we used the
Numerical Scale and Sensitive Faces Scale for low education and cognitive
changes. Results: Most of the elderly in this study did not present the
presence of rheumatic diseases; however, a large part reports moderate to
severe pain, mainly in the lumbar spine, knees, and legs, and do not present
functional physical decline even with signs of rheumatic diseases.
Keywords: aged; rheumatic disease; pain, referred.
Introdução: Identificou-se e descreveu-se a
presença de doença reumática autorreferida e de dor
em idosos do interior do Amazonas. Métodos: Foram visitados 131 idosos
residentes do Amazonas. Utilizou-se o Índice de Comorbidades Funcional (ICF) para
rastrear a presença de doenças autorreferidas e para
avaliação de dor utilizou-se a Escala numérica e de faces que são sensíveis
para baixa escolaridade e alterações cognitivas. Resultados: A maioria
dos idosos deste estudo não apresentou presença de doenças reumáticas autorreferidas e são funcionais, porém, grande parte relata
dor de moderada à forte principalmente na coluna lombar, joelhos e pernas.
Palavras-chave:
idoso; doença reumática; dor referida.
Introduction
Population aging is becoming
increasingly evident in all countries of the world [1]. In 1950, the number of
people aged 60 years or more was 202 million; in 2020 it increased to 1.1
billion, and it is expected to reach 3.1 billion by 2100 [1]. In Brazil, this
global trend is observed even more markedly. In 2020, the number of Brazilians
aged 80 years or more reached 4.2 million and was expected to increase to 28.2
million in 2100 [2]. The different Brazilian states have specific
characteristics regarding the aspects related to population aging [3]. In
Amazonas, the elderly population in urban and rural areas represents 6.02% of
the total population [3]. In some cities in the state's interior, it is
possible to observe even higher numbers, such as in Coari,
which has more than 45% of elderly people [4].
The phenomenon of population aging
brings several consequences, among which is the increased frequency of
diseases, frailty, or disabilities [5]. According to the Brazilian Society of
Geriatrics and Gerontology (SBGG), advancing age is the leading risk factor for
chronic and degenerative diseases [5]. Rheumatic diseases are the most
prevalent among older Brazilian people; about 37.5% of people aged 60 years or
more are affected by this heterogeneous group of diseases [6]. They are
characterized by causing systemic alterations involving the connective tissue,
causing joint pain, and even causing deformities that lead to incapacity to
perform basic functional activities [7].
Research on this subject still
needs to be conducted in the Amazonian population. Thus, knowing that rheumatic
diseases are the second most prevalent self-reported disease in the Brazilian
elderly and that the complaint of pain in this public may be related to at
least one significant health problem that can impact the functionality and
purpose of life of these people [8,9], we sought to identify and describe the
presence of self-reported rheumatic diseases and the presence of pain in the
elderly assessed in their homes in the countryside of the state of Amazonas.
Methods
This cross-sectional and
descriptive study presents pain characteristics and self-reported rheumatic
diseases in older people evaluated at home in Coari,
in the state of Amazonas. The sample size was random and straightforward until
the number of 131 older people was reached. This study is part of a more
extensive study evaluating the elderly at home in Coari,
Amazonas.
The inclusion criterion was 60
years old or older and physical and cognitive ability to answer the
evaluations. The exclusion criterion was the elderly who were unable (mentally)
to answer the questions and participate in the assessments.
Data collection was carried out in
the first and second semesters of 2019 after the approval of the Research
Ethics Committee of the Universidade Federal de
Amazonas (UFAM) under the registration of CAAE number: 08021319.0000.5020.
First, the elderly, their families, or caregivers were informed about the
study, and when they consented to participate, they signed the Informed Consent
Form (ICF). Then, to characterize the elderly, a semi-structured questionnaire
was applied to contain the following information: age group, gender, level of
education, housing situation, medications taken, place of birth, self-reported
diseases, and monthly income.
To evaluate pain, two scales were
used that are sensitive to the screening of pain in older people with low
education. The Numerical Pain Scale was applied, which allows quantifying the
intensity of pain using numbers from 0 to 10, 0 (zero) represents no pain, and
10 (ten) represents maximum pain [10], and then the Faces Scale, where the
elderly indicate the intensity of their pain according to the expression that
the mimic means in each drawn face, the expression of happiness corresponds to
the classification "no pain" and the manifestation of maximum sadness
corresponds to the classification "maximum pain " [11].
The Functional Comorbidity Index
(FCI) was applied to check the presence of self-reported rheumatic diseases,
which consists of a list of 18 comorbidities, with no difference in weights
among them. The ICF score is obtained by the sum of all comorbidities present
and ranges from 0 to 18 [12].
A descriptive statistical analysis
was performed from the collected data. A spreadsheet database was built and
analyzed using SPSS (Statistical Package for the Social Science), version 22.0,
and Microsoft Excel 2007®.
Results
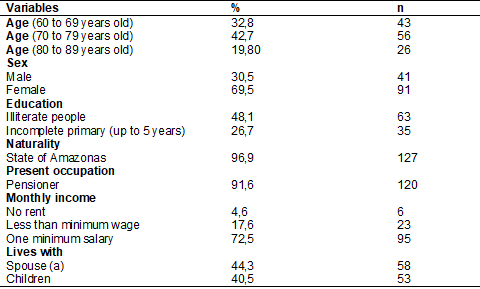
One hundred and thirty-one elders
of both sexes were evaluated in their homes in the countryside of the Amazonas.
The sociodemographic characteristics of these elderly are described in table I.
Table I - Sociodemographic data of the
elderly living in the interior of Amazonas (n = 131)
Sources: autores
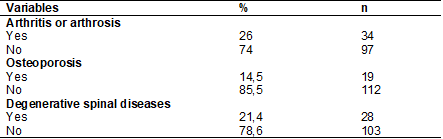
The self-reported rheumatic
diseases concern the group of osteoarthritis and degenerative diseases of the
spine. These findings are described in table II.
Table II - Self-reported rheumatic
diseases by the elderly in the Interior of Amazonas (n = 131)
Source: autores
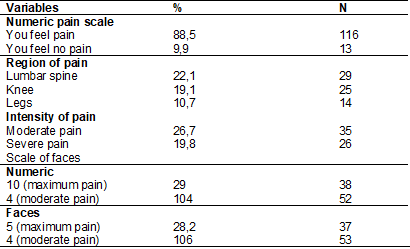
Regarding the presence of pain, the
main findings are described in table III.
Table III - Assessment of pain degree
with the face and numeric scales (n = 131)
Sources: autores
Discussion
The sample of this study is
composed mainly of older women aged 70 to 79. Of these, most are illiterate,
presenting a low level of education. They are from the interior of the state of
Amazonas, are retired, and have incomes of up to less than one minimum wage per
month. These characteristics are similar to the sociodemographic profile
described by Costa et al. [13] in their study of elderly residents of
rural areas in Coari/AM.
Regarding education, it was
observed that working in the field or fishing is the primary source of income,
and education was seen as a privilege, being possible only for those with
higher financial status [13]. According to Silva et al. [14], low
schooling and the prevalence of agricultural activities are frequent among the
elderly living in rural areas. It is worth mentioning that for those living in
areas far from the city, the high cost and difficulties of access through river
transport to schools are considered major obstacles to continuing their studies
[13,14]. Torres et al. [15] state that the problem of displacement is a
contributing factor to the prevalence of illiterate or unlettered people, which
may be directly linked to low income.
As for the participation of older
women in this study, Storti et al. [16]
justified that their presence in the study, when compared to men, is mainly due
to differences in lifestyles, either in the consumption of alcohol and tobacco
or because most of them are more likely to request health services [16].
Regarding the findings by the ICF,
the elderly in this study reported not having any rheumatic diseases:
osteoarthritis or osteoarthrosis, osteoporosis, or degenerative diseases of the
spine. In Holick et al. [17], the opposite of
this study was found; the author states that in the elderly, rheumatic diseases
have a higher incidence, with osteoarthritis, osteoporosis, and spinal diseases
being the most common.
When we evaluated the results by
the numerical pain scale and the faces scale, the elderly reported pain,
referring to it with greater intensity in the regions of the lumbar spine,
knees, and legs. For Dellaroza et al. [18],
pain can be understood as a multifactorial phenomenon due to an injury,
emotional, sociocultural, or environmental aspects. In his other study about
chronic pain in the elderly, Dellaroza et al.
[19] states that the most prevalent sites for pain in the elderly were 21.7% in
the back and 21.7% in the lower limbs.
On the Numerical and Face Scale,
the pain was considered moderate to severe, and some studies [19,20,21] point out
that pain in the elderly is frequent in women and can be associated with their
lifestyles. For Cunha et al. [22], the leading cause of pain in the
elderly is osteoarticular diseases. With that, returning to the ICF, it was
observed that most of the elderly presented difficulties relating their pain to
the diseases mentioned, making it clear that the lack of information influenced
the interpretation of this questionnaire.
The presence of pain can cause
limitations in activities of daily living (ADL) in the elderly; for Ferretti et
al. [23], pain interferes with the acuity that each individual has in his
life, and due to this act, it is necessary to take appropriate actions that can
provide well-being and pain control, aiming at reducing pain complaints to
improve functional capacity.
When assessing pain in the elderly,
we impact their quality of life, for most of the time, pain drives to
situations that generate discomfort and limitations [24]. In the studies by
Gold et al. [25], one can see that pain causes an impact on daily
activities with a high prevalence of functional disability, greater frailty,
and high levels of comorbidities.
The low level of education and the
little knowledge of the elderly in this study about the pathologies may have
directly influenced how the elderly made the self-report; in this sense, the
self-report may not express the reality.
There is a need for further studies
on the subject, and more research on these older people since the impact of
rheumatic diseases on the health of the elderly population is well known and
described in the literature.
Conclusion
The elderly in this study present
pain, some rheumatologic complaints, and changes in the functions of the lower
limbs; however, they have difficulty in self-reporting rheumatic diseases; it
is believed that this happens due to the enormous difficulty in diagnosing
these diseases in the interior of the state of Amazonas, besides the low
education and understanding when asked about the presence of these
comorbidities. It is necessary, based on the complaint that these
elderly have to perform the clinical and functional diagnosis for rheumatic
diseases, to foster decision-making and prevention in health for this
population.
Conflict of interest
There is no conflict of interest
Funding source
There were no external funding
sources for this study
Authors’ contributions
Research conception and
design: Campos HLM; Data collection: Silva GS, Braga
JAC, Prestes YA; Data analysis and interpretation:
Campos HLM, Braga JAC, Prestes YA; Manuscript
writing: Braga JAC, Prestes YA, Silva GS; Critical
review of the manuscript for important intellectual content: Braga JAC,
Checchi MHR, Leon EB
References
- Alves JED. Envelhecimento populacional no Brasil e no mundo. Novas projeções da ONU. Rev LongeViver. 2019
- Instituto Brasileiro de Geografia e
Estatística [Internet]. Projeção da
População [Internet]. [cited 2020 Jan 13]. Available
from: https://agenciadenoticias.ibge.gov.br/agencia-sala-de-imprensa/2013-agencia-de-noticias/releases/21837-projecao-da-populacao-2018-numero-de-habitantes-do-pais-deve-parar-de-crescer-em-204
- Costa EAC, Shor T.
Envelhecimento populacional e sua produção
histórica no Brasil, Amazonas, Tefé, Alvarães e
Uarini-Am. Anais do VII CBG [Internet]. 2014. [cited 2020 Jan 15]. Available from:http://www.cbg2014.agb.org.br/resources/anais/1/1404152885_ARQUIVO_ENVELHECIMENTOPOPULACIONALESUAPRODUCAOHISTORICANOBRASIL_ArtigoCompleto.pdf
- Instituto Brasileiro de Geografia e Estatística [Internet]. Censo de 2010 [Internet]. [cited 2020 Jan 15]. Available from: http://cidades.ibge.gov.br/painel/populacao.php?lang=&codmun=130120&search=|coari
- Sociedade Brasileira de Geriatria e Gerontologia [Internet]. Envelhecimento e longevidade. 2020. [cited 2020 Jan 20]. Available from: https://sbgg.org.br/envelhecimento-e-longevidade/
- Lima-Costa MF, Barreto SM, Giatti L.
Health status, physical functioning, health services utilization, and
expenditures on medicines among Brazilian elderly: a descriptive study
using data from the National Household Survey. Cad Saúde Publica. 2003;19(3):735-43.
- Ramos HVL, Pillon J, Kosugi EM, Fujita R, Pontes P. Avaliação laríngea em pacientes reumatológicos. Rev Bras Otorrinolaringol. 2005;71(4):499-503. doi: 10.1590/S0034-72992005000400017 [Crossref]
- Bettiol CHO, Dellaroza MSG, Lebrão ML, Duarte YA, Santos HG. Fatores preditores de dor em idosos do Município de São Paulo, Brasil: Estudo SABE 2006 e 2010. Cad Saúde Pública. 2017;33(9):e00098416. doi: 10.1590/0102-311X00098416 [Crossref]
- Picavet HS, Hazes JM. Prevalence of self-reported musculoskeletal diseases is high. Ann Rheum Dis. 2003; 62:644-50. doi: 10.1136/ard.62.7.644 [Crossref]
- Andrade FA, Pereira LV, Sousa FAEF. Mensuração da dor no idoso: uma revisão. Rev Latino-Am Enferm. 2006;14(2);271-6. doi: 10.1590/S0104-11692006000200018 [Crossref]
- Ciena AP, Gatto R, Pacini VC, Picanço VV, Magno IMN, Loth EA. A influência da intensidade da dor sobre as respostas nas escalas unidimensionais de mensuração da dor em uma população de idosos e de adultos jovens. Semina: Ciências Biológicas e da Saúde [Internet]. 2008[citado 2022 Out 12];29(2);201-12. doi: 10.5433/1679-0367.2008v29n2p201 [Crossref]
- Groll DL, To T, Bombardier C, Wright JG. The development of a comorbidity index with physical function as the outcome. J Clin Epidemiol. 2005;58(6);595-602. doi: 10.1016/j.jclinepi.2004.10.018 [Crossref]
- Costa RS, Leão LF, Campos HLM. Envelhecer na zona rural do interior do estado do Amazonas, desempenho cognitivo, funcionalidade e percepção de saúde: um estudo transversal. Revista Kairós – Gerontologia. 2020;23(1):83-103. doi: 10.23925/2176-901X.2020v23i1p83-103 [Crossref]
- Silva EF, Paniz VMV, Laste GL, Torres ILST. Prevalência de morbidades e sintomas em idosos: um estudo comparativo entre zonas rural e urbana. Ciênc Saúde Coletiva. 2013;18(4). doi: 10.1590/S1413-81232013000400016 [Crossref]
- Torres GV, Reis LA, Fernandes MH.
Características sociodemográficas e de saúde de
idosos dependentes residentes em domicilio. Espaç Saúde [Internet]. 2009 [cited 2022 Out 12];10(2);12-17. Available from: https://pesquisa.bvsalud.org/portal/resource/pt/lil-528441
- Storti LB, Whebe SCCF, Kusumota L, Rodrigues RAP, Marques SI. Fragilidade de idosos internados na clínica médica da unidade de emergência de um hospital geral terciário. Texto Contexto Enferm. 2013;22(2):452-9. doi: 10.1590/S0104-07072013000200022 [Crossref]
- Holick MF. Vitamin D deficiency. N Engl J Med. 2007;357(3):266-81.
- Dellaroza MSG, Furuya RK, Cabrera MAS, Matsuo T, Trelha C, Yamada KN. Caracterização da dor crônica e métodos analgésicos utilizados por idosos da comunidade. Rev Assoc Med Bras. 2008;54(1):36-41. doi: 10.1590/S0104-42302008000100018 [Crossref]
- Dellaroza MSG, Pimenta CAM, Matsuo T. Prevalência e caracterização da dor crônica em idosos não institucionalizados. Cad Saúde Pública. 2007;23(5). doi: 10.1590/S0102-311X2007000500017 [Crossref]
- Helme RD, Gibson SJ, Croft PR, Linton SJ, Le Resche L, von Korff M. Pain in the older people. In: Crombie IK, Croft PR, Linton SJ, Le Resche L, von Korff M, eds. Epidemiology of pain. Seattle: IASP Press; 1999. p. 103-12.
- Andersson HI, Ejlertsson G, Leden I, Rosenberg C. Chronic pain in a geographically defined general population: studies of differences in age, gender, social class, and pain localization. Clin J Pain. 1993;9:174-82. doi: 10.1097/00002508-199309000-00004 [Crossref]
- Cunha LL, Mayrink WC. Influência da dor crônica na qualidade de vida em idosos. Rev Dor. 2011;12(2):120-4. doi: 10.1590/S1806-00132011000200008 [Crossref]
- Ferretti F, Castanha AC, Padoan ER, Lutinski J, Silva MR. Quality of life in the elderly with and without chronic pain. BrJP. 2018;1(2):111-5. doi: 10.5935/2595-0118.20180022 [Crossref]
- Freitas RS, Fernandes MH, Coqueiro RS, Reis WJ, Rocha S, Brito A. Capacidade funcional e fatores associados em idosos: estudo populacional. Acta Paul Enferm. 2012;25(6):933-9. doi: 10.1590/S0103-21002012000600017 [Crossref]
- Gold DT, Roberto KA. Correlates and consequences of chronic pain in older adults. Geriatr Nurs 2000;21(5):270-3. doi: 10.1067/mgn.2000.110838 [Crossref]
