Fisioter Bras.
2023;24(2):181-90
ORIGINAL ARTICLE
Subjective health assessment and functional
characterization of elderly people living in a city in the interior of Amazonas
state
Avaliação
subjetiva da saúde e caracterização da funcionalidade de idosos domiciliados
numa cidade do interior do Amazonas
Victor
Cezar Mendes de Melo1, Yandra Alves
Prestes1, Johrdy Amilton da Costa Braga2,
Higor Gregore Alencar
Oliveira1, Maria Helena Ribeiro de Checchi1, Elisa Brosina de Leon2, Hércules Lázaro Morais Campos1
1Instituto de Saúde e Biotecnologia,
Universidade Federal do Amazonas, Coari, AM, Brazil
2Faculdade de Educação Física e
Fisioterapia, Universidade Federal do Amazonas, Manaus, AM, Brazil
Received: October 6, 2022; Accepted: November 15,
2022.
Correspondence: Hércules Lázaro Morais Campos, herculeslmc@hotmail.com
How to cite
Melo VCM, Prestes YA,
Braga JAC, Oliveira HGA, Checchi MHR, Leon EB, Campos
HLM. Subjective health assessment and functional
characterization of elderly people living in a city in the interior of Amazonas
state. Fisioter Bras. 2023;24(2):181-90. doi: 10.33233/fb.v24i2.5307
Abstract
Objective: The subjective assessment of
health and functionality of the elderly domiciled in the interior of Amazonas
in the city of Coari was performed. Methods:
This is a cross-sectional observational and descriptive study with 81 elderly
assessed at home in the first half of 2019. The Who Disability Assessment
Schedule (WHODAS 2.0) was applied to assess functionality and the Subjective
Health Assessment Questionnaire for self-report of health. Results: Of the
81 elderly, the majority are women n = 62 (76.5%) from 70 to 79, who have not
completed 1 year of schooling n = 55 (67.9%) and have wage income equal to or
less than 1 minimum wage n = 72 (88.8%) minimum. It was found no or mild
difficulty for the domains evaluated in the WHODAS 2.0 and the self-reported
health was regular or poor n = 66 (81.5%) for most of the elderly. Conclusion:
The elderly from Coari assessed at home are mostly
independent and functional and report a poor self-perception of health compared
to others of the same age.
Keywords: elderly, health level,
psychosocial effects of illness, functionality; home care.
Resumo
Objetivo: Realizou-se a avaliação subjetiva da
saúde e da funcionalidade dos idosos domiciliados na cidade de Coari no
interior do Amazonas. Métodos: Trata-se de um estudo transversal e
descritivo com 81 idosos avaliados em domicílio no primeiro semestre de 2019. Aplicou-se
o Who Disability Assessment Schedule (WHODAS
2.0) para avaliar funcionalidade e o questionário de avaliação subjetiva da
saúde para o autorrelato da saúde. Resultados:
Dos 81 idosos, a maioria são mulheres n = 62 (76,5%) com faixa etária de 70 a
79, que não chegaram a completar 1 ano de escolaridade n = 55 (67,9%) e possuem
renda salarial igual ou inferior a 1 salário mínimo n = 72 (88,8%).
Encontrou-se nenhuma ou leve dificuldade para os domínios avaliados no WHODAS
2.0 e a saúde autorrelatada foi de regular ou ruim n
= 66 (81,5%) para a maioria dos idosos. Conclusão: Os idosos de Coari
avaliados em domicílio são em sua grande maioria independentes e funcionais
embora relatem autopercepção da saúde ruim comparada com outros da mesma idade.
Palavras-chave: idoso; nível de saúde; efeitos
psicossociais da doença; funcionalidade; assistência domiciliar.
Introduction
Aging is a natural and irreversible
phenomenon; it does not occur equally and simultaneously in humans. Aging is
part of life, and with the knowledge obtained so far, there are no ways to
change this process [1].
According to the WHO, between 2015
and 2050, the proportion of the world's elderly population over 60 will almost
double from 12% to 22% [2]. By 2050, the world's population aged 60 and over is
expected to total 2 billion, almost double today's elderly population [3].
The estimate of older people in
Brazil is about 28 million, a number that represents 13% of the country's
population, which tends to double in the following decades: a quarter of the
population will be over 60 years old by 2043, while the population of young
people up to 14 years old will be only 16.3% [4].
Self-rated health has been a widely
used variable in significant population-based health and well-being investigations,
showing that it is an excellent multidimensional indicator of health and a good
predictor of adverse events for the elderly population [5].
Self-assessing health depends on
how a person understands good health, not only considering the physical
problems that correlate with the aging process but also involving autonomy,
feelings of control, and day-to-day functionality [6].
Recent studies point out that this
assessment, in old age, is linked both to well-being [7,8] and to morbidity,
mortality, and functional decline indicators [9]. The elderly tend to evaluate their health status positively, and to
explain this, subjective comparison mechanisms are used social [10]. Possibly,
they adopt as a basis of comparison people in worse health and functioning
conditions than their own, leading to a sense of superiority [11]
Aging with quality of life depends
on several factors, such as health, family support, sufficient income,
opportunities for social and political participation, and good functionality
[12]. Functional capacity and performance reflect the health-related attributes
that enable people to be and do what they value or judge to be relevant [13].
Thus, functionality stands out as
one of the main components of healthy aging, pointed out by the elderly as one
of the essential aspects of life, as it is associated with independence and
autonomy. This does not mean, however, having good performance and good
competence in all domains during the entire course of life [12].
The functionality was characterized
along with the subjective evaluation of the health of the elderly population in
the city of Coari.
Methods
This is a cross-sectional and
descriptive study that presents the functional characteristics and the
subjective evaluation of the health of older people domiciled in the city of Coari in the interior of the Amazonas. This research was
approved by the Research Ethics Committee of the Federal University of Amazonas
(UFAM) under the registration number CAEE: 08021219.1.0000.5020; data collection
was carried out in the first and second semesters of 2019.
The students visited the homes of
older people in the city of Coari, in the state of
Amazonas, until the repetition of the researched data was noticed.
The elderly, their relatives, and caregivers were
informed about the study, and when they consented to participate, they signed
the Informed Consent Form (ICF).
In this study, the family member
and caregiver could answer and help the elderly. The inclusion criteria were
elderly individuals aged 60 years or older, with cognitive ability and autonomy
to actively participate in the evaluation battery. Although the Mini-Mental
State Examination cognitively assessed this group, we included all the elderly
regardless of the cut-off score for this test since the group was interested in
working with older people with moderate to severe cognitive deficits.
Older people with complete aphasia
and physical and cognitive inability to answer the battery of tests were
excluded.
For the characterization of the
elderly, a semi-structured questionnaire was applied, containing the following
information: age group, gender, level of education, housing situation,
medicines taken, place of birth, self-reported diseases, and monthly income.
To analyze functionality, the
Disability Assessment Schedule (WHODAS 2.0) was applied, an instrument that
measures the level of health and disability of the population and assists
clinical practice. This instrument evaluates the disability in six domains of
life: cognition, movement, self-care, interaction with others, activities of
life, and participation. For each item of WHODAS 2.0, the amount of difficulty
a subject has in the last month to perform their activities is evaluated [14].
To evaluate the subjective perception of health, a short questionnaire was used
to determine how each person considers their health based on the questions. In
general, how do you rate your health at the present moment? How do you rate
your health compared to other people your age? How do you rate your memory
compared to other people your age? How do you rate your health today compared
to a year ago? How do you rate your activity today compared to a year ago?
Based on the answer, the older person will choose one of five options, ranging
from much worse to much better [15].
From the collected data, a
spreadsheet database was built and analyzed using the SPSS (Statistical Package
for the Social Science) program, version 22.0, and Microsoft Excel 2007®
application.
Results
Most of the elderly in this study
are female and aged between 70 and 79; all the sociodemographic characteristics
are shown in table I.
Table I - Characterization of the
sample of elderly residing in the countryside of Amazonas (n = 81)
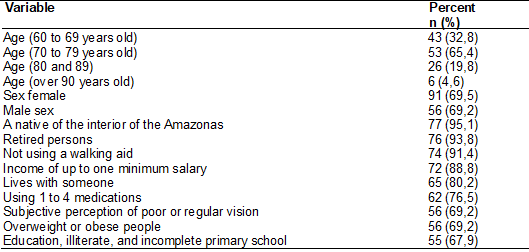
Source: Melo, 2021
About the WHODAS 2.0, it was
observed that most of the elderly had no mild or medium difficulty in the last
30 days for most of the domains. The other data are in Table II.
Table II - WHODAS 2.0 12-item version,
degree of difficulty in the last 30 days (n = 81)
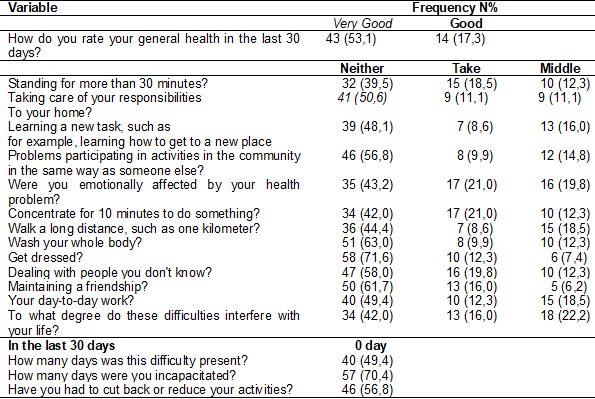
Source: Melo, 2021
More than half of the elderly
describe their health as regular or poor; the remaining information about
subjective health assessment is in table [III].
Table III - Results of Subjective Health
Assessment n = 81
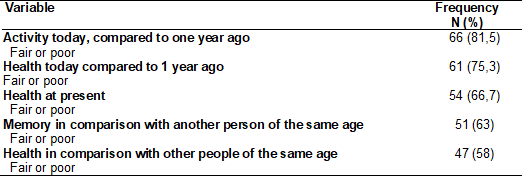
Fonte: Melo, 2021
Discussion
Most of the elderly in this study
were women aged 70 to 79 who did not complete one year of schooling and have a
wage income of 1 minimum wage or less. The high rate of women is due to their
higher survival rate, differences in exposure to occupational risks, higher
mortality rates from external causes among men, differences in lifestyles
regarding alcohol and tobacco consumption, and higher demand for health
services among them [16].
Regarding schooling, more than half
of the elderly assessed in their homes in the city of Coari
are illiterate or have only an incomplete primary school education, with the
majority not having completed one year of schooling. This low level of
education is because education is not seen as a priority in the region [17].
Many of the elderly in this study reported that during their childhood, they
lived in the city's rural area and that the socioeconomic cost, along with the
distance, was an obstacle to studying in the city. According to Torres &
Reis, the difficulty of transportation contributes to the prevalence of
illiterate or unlettered people [18].
The evaluation of functionality
through WHODAS 2.0 showed that most of these elderly
do not have difficulty performing their activities of daily living. There was a
high percentage of elderly who reported no problems with disability due to pain
or discomfort, which is reflected in their independence for the activities of
daily living. These data reflect the elderly's quality of life since it is
directly influenced by functionality related to independence and autonomy [12].
The elderly presented functional
independence for almost all the functions evaluated; however, they
self-reported terrible health compared to other people of the same age or
reached the previous year, which is controversial since the literature shows
that the more functional the elderly are, the greater their satisfaction with
life and their well-being [19,20]. According to Soares et al. [21], good
physical performance seems fundamental for functionality when facing daily
demands and for good perception of life. This reinforces the findings of Rocha et
al. [22], who stated that higher levels of self-perceived health are
associated with higher levels of independence in daily living.
People who are resilient in their
daily life practices in youth and adulthood are precisely those who will
generally have good health, few diseases, a good level of self-care, preserved
physical and mental functioning, adherence to physical activities, social
participation, and satisfaction with life, assuming that by middle age, such
resilience tends to increase, functioning as a driver of adaptations to a
prosperous old age [23,24].
One hypothesis to explain the
adverse self-reported health may be related to the level of education of the
elderly since it is related to cognitive decline [25]. The worsening of
self-reported memory, lower cognitive performance, the presence of depressive
symptoms, functional dependence, and the high prevalence of nonspecific
complaints and comorbidities are included in the aging process, in which low
education is one of the risk factors for these conditions found in the elderly
[26,27]. This reinforces the findings of Medeiros et al. [28]. According
to him, higher education is a limitation for studies with self-reported health,
as it can compromise the understanding of the investigated questions and the
quality of the answers.
Studies in developed countries have
shown that self-rated health is strongly influenced by the socioeconomic status
of the elderly and their families [29]. The self-assessment of health as
excellent or very good stands out among the elderly with better education and
income [30]. Another factor influencing this unfavorable result of
self-reported health is the low income since most elderly subjects in this
study did not earn more than one minimum wage.
Conclusion
The elderly living in Coari are mostly independent. In functional aspects, the
elderly in this study have little functional limitation; however, the
self-reported health does not match the degree of functionality that the data
show, which may be caused by low income and low education. Further studies
should be done to correlate the data found to know if cognition is not
interfering with self-reported health. It is necessary to evaluate a more
significant number of older people so that these data can be generalized to
this population.
Funding
source
No funding.
Conflict
of interest
The authors report no conflicts of interest.
Author’s
contribution
Data collection and
manuscript writing: Melo VCM, Oliveira HGA; manuscript
writing and correction: Prestes YA, Braga JAC; Study orientation:
Checchi MHR, Leon EBD; Concept and design of the study, critical review of
the article and study orientation: Campos HLM.
References
- Dantas
EHM, Santos CAS. Aspectos biopsicossociais do envelhecimento e a prevenção de
quedas na terceira idade. 1 ed. Unoesc; 2017.
- World
Health Organization. Envelhecimento e Saúde. 2020. Available from: http://www.who.int/news-room/fact-sheets/detail/ageing-and-health/
- Alves
JED. Laboratório de demografia e estudos populacionais. Envelhecimento
populacional continua e não há perigo de um geronticídio
[Internet]. [citado 2022 Mar 30]. Available from: https://www.ufjf.br/ladem/2020/06/21/envelhecimento-populacional-continua-e-nao-ha-perigo-de-um-geronticidio-artigo-de-jose-eustaquio-diniz-alves/
- Instituto
Brasileiro de Geografia e Estatística - IBGE. Projeção da População. 2018.
[Internet]. [citado 2022 Mar 22]. Available from:
https://agenciadenoticias.ibge.gov.br/agencia-saladeimprensa/2013-
agencia-denoticias/releases/21837-projecao-da-populacao-2018numero-dehabitantes-do-paisdeveparar-de-crescer-em-204/
- Whitley E, Popham F, Benzeval
M. Comparison of the Rowe–Kahn Model of successful aging with self-rated health
and life satisfaction: The West of Scotland Twenty-07 Prospective Cohort Study.
Gerontologist. 2016;56(6):1082-92.
https://doi.org/10.1093/geront/gnv054 [Crossref]
- Henchoz K, Cavalli S, Girardin. Health perception and health status in advanced old age: A paradox of association. J Aging Studies. 2008;22:282-90. https://doi.org/10.1016/j.jaging.2007.03.002 [Crossref]
- Borim FSA, Neri AL, Francisco PMSB, Barros MBA. Dimensões da autoavaliação de saúde em idosos. Rev Saúde Pública. 2014;48(5):714-22. https://doi.org/10.1590/S0034-8910.2014048005243 [Crossref]
- Confortin SC, Giehl MWC, Antes DL, Schneider IJC. Autopercepção positiva de saúde em idosos: estudo populacional no Sul do Brasil. Cad Saúde Pública. 2015;31(5):1049-60. https://doi.org/10.1590/0102-311X00132014 [Crossref]
- Shen C, Schooling CM, Chan WM, Zhou JX, Johnston JM, Lee SY, et al. Self-rated health and mortality in a prospective Chinese elderly cohort study in Hong Kong. Prevent Med. 2014;67:112-8. https://doi.org/10.1016/j.ypmed.2014.07.018 [Crossref]
- Cramm JM, Bornscheuer L, Selivanova A, Lee J. The health of India’s elderly population: A comparative assessment using subjective and objective health outcomes. J Popul Ageing. 2015;8:245-59. https://doi.org/10.1007/s12062-015-9122-2 [Crossref]
- Cheng S-T, Fung H, Chan A. Maintaining self-rated health through social comparison in old age. J Gerontol. 2007;62B(5):277-85. https://doi.org/10.1093/geronb/62.5.p277 [Crossref]
- Perracine MR, Fló CM. Funcionalidade
e envelhecimento. 2ª ed. Rio de Janeiro: Guanabara Koogan; 2019.
- Beard JR, Blom DE. Towards a comprehensive public heath response to population ageing. Lancet. 2015;385(9968):658-61. https://doi.org/10.1016/S0140-6736(14)61461-6 [Crossref]
- Moreira A, Alvarelhão J, Silva AG, Costa R, Queirós A. Tradução e validação para português do WHODAS 2.0 - 12 itens em pessoas com 55 ou mais anos. Rev Port Saúde Pública. 2015;33(2). https://doi.org/10.1016/j.rpsp.2015.06.003 [Crossref]
- Medeiros SM, Silva LSR, Carneiro JM, Ramos GCF, Barbosa ATF, Caldeira AP. Fatores associados à autopercepção negativa da saúde entre idosos não institucionalizados de Montes Claros, Brasil. Ciênc Saúde Coletiva 2016;21(11). https://doi.org/10.1590/1413-812320152111.18752015 [Crossref]
- Storti LB, Whebe SCCF, Kusumota L, Rodrigues RAP, Marques Sueli. Fragilidade de idosos internados na clínica médica da unidade de emergência de um hospital geral terciário. Texto Contexto Enferm. 2013;22(2):452-9. https://doi.org/10.1590/S0104-07072013000200022 [Crossref]
- Costa RS, Leão LF, Campos HLM. Envelhecer na zona rural do interior do estado do Amazonas, desempenho cognitivo, funcionalidade e percepção de saúde: um estudo transversal. Revista Kairós Gerontologia. 2020;23(1):83-103. https://doi.org/10.23925/2176-901X.2020v23i1p83-103 [Crossref]
- Torres GV, Reis LA, Fernandes MH. Características sociodemográficas e de saúde de idosos dependentes residentes em domicílio. Espaç Saúde. 2009;10(2):12-7. https://doi.org/10.1590/S0104-11692011000500022 [Crossref]
- Spocito G, D’elboux MJ, Neri AL, Guariento ME. A satisfação com a vida e a funcionalidade em idosos atendidos em um ambulatório de geriatria. Ciênc Saúde Coletiva. 2013;18;3475-3482. https://doi.org/10.1590/S1413-81232013001200004 [Crossref]
- Luoh MC, Herzog AR. Individual consequences of volunteer and paid work in old age: health and mortality. J Health Soc Behav. 2002;490-509. https://doi.org/10.2307/3090239 [Crossref]
- Soares VN, Fattori A, Neri AL, Fernandes PT. Influência do desempenho físico na mortalidade, funcionalidade e satisfação com a vida de idosos: dados do estudo FIBRA. Ciênc Saúde Coletiva. 2019;(24):4181-90. https://doi.org/10.1590/1413-812320182411.07592018 [Crossref]
- Rocha JP, Oliveira GG, Jorge LB, Rodrigues FR, Morsch P, Bós AJG. Relação entre funcionalidade e autopercepção de saúde entre idosos jovens e longevos brasileiros. Revista Saúde e Pesquisa. 2017;10(2):283-291. https://doi.org/10.177651/1983-1870.2017v10n2p283-291 [Crossref]
- Sato S, Demura S, Kobayashi H, Nagasawa Y. The relationship and its change with aging between ADL and daily life satisfaction characteristics in independent Japanese elderly living at home. J Physiol Anthropol. 2002;21(4):195-204. https://doi.org/10.2114/jpa.21.195 [Crossref]
- Garbaccio JL, Estêvão WG, Jacome BB, Batista LAT. Envelhecimento e qualidade de vida de idosos residentes na zona rural. Rev Bras Enferm. 2018;(71):776-84. https://doi.org/10.1590/0034-7167-2017-0149 [Crossref]
- Nascimento RASAD, Batista RTS, Rocha SV, Vasconcelos LRC. Prevalência e fatores associados ao declínio cognitivo em idosos com baixa condição econômica: estudo MONIDI. J Bras Psiquiatr. 2015;64(3):187-192. https://doi.org/10.1590/0047-2085000000077 [Crossref]
- Silveira EA, Vieira LL, Souza JD. Elevada prevalência de obesidade abdominal em idosos e associação com diabetes, hipertensão e doenças respiratórias. Ciênc Saúde Coletiva. 2018;(23):903-12. https://doi.org/10.1590/1413-81232018233.01612016 [Crossref]
- Santos RR, Bicalho MAC, Mota P, de Oliveira DR, de Moraes EN. Obesity in the elderly. Rev Med Minas Gerais.2013;(1):23. https://doi.org/10.5935/2238-3182.20130011 [Crossref]
- Medeiros
SM, Silva LSR, Cameiro JM, Ramos GCF, Barbosa ATF,
Caldeira AP. Fatores associados à autopercepção negativa da saúde entre idosos
não institucionalizados de Montes Claros, Brasil. Ciênc
Saúde Coletiva. 2016;21(11). https://doi.org/10.1590/1413-812320152111.18752015 [Crossref]
- Costa MFL, Firmo JOA, Uchôa E. A estrutura da auto-avaliação da saúde entre idosos: projeto Bambuí. Rev Saúde Pública. 2004;38:(6). https://doi.org/10.1590/S0034-89102004000600011 [Crossref]
- Borim FSA, Barros MBDA, Neri AL. Autoavaliação da saúde em idosos: pesquisa de base populacional no Município de Campinas, São Paulo, Brasil. Cad Saúde Pública. 2012;(28):769-80. https://doi.org/10.1590/S0102-311X2012000400016 [Crossref]
