Fisioter Bras.
2023;24:(5):555-63
ORIGINAL ARTICLE
Physical therapy and Pilates in the functionality and
quality of life of people with multiple sclerosis
Fisioterapia
e Pilates na funcionalidade e qualidade de vida de pessoas com esclerose
múltipla
Edson
Toshiro Nakau¹, Irana de Souza Castro1,
Juliana Aparecida Rhein Talles1, Alice
Estevo Dias1, Rita Helena Duarte Dias Labronici2
1Centro Universitário Saúde ABC, Santo
André, SP, Brasil
2Universidade de São Paulo; Associação
Brasileira de Esclerose Múltipla (ABEM), São Paulo, SP, Brasil
Received: April 13, 2023; Accepted: September 9, 2023
Correspondence: Alice Estevo, alice.estevo@abem.org.br
How to cite
Nakau ET, Castro IS, Talles
JAR, Dias AE, Labronici RHDD. Physical therapy and Pilates in the functionality
and quality of life of people with multiple sclerosis. Fisioter Bras.
2023;24(5):555-63. doi: 10.33233/fb.v24i5.5421
Abstract
Background: Multiple
Sclerosis is a chronic progressive disease that affects the Central Nervous
System, causing destruction of myelin, and like many autoimmune diseases, it
should be caused by a combination of environmental and genetic factors. Objective:
To evaluate the influence of conventional physical therapy and the Pilates
method in patients with Relapsing Remitting MS (RRMS) on their daily activities
and quality of life. Methods: We retrospectively analyzed 25 medical
records of patients submitted to Pilates (group A with 12 patients) and physical
therapy (group B with 13 patients) with only one technique for each group from
2018 to 2019. Some scales were used: the Berg Balance
Scale, Modified Fatigue Impact Scale (MFIS), MRC Medical Research Council Scale
(MRC), and Quality of Life in Multiple Sclerosis Scale (MSQOL-54). Results:
With the significance level adopted for p < 0.05, by the Wilcoxon test, we
obtained MFIS: conventional p = 0.030 and Pilates p = 0.005, BERG: conventional
p = 0.015 and Pilates p = 0, 004, MSQOL-54 (Physical): Conventional p = 0.263
and Pilates p = 0.009 and MSQOL-54 (Mental): Conventional p = 0.807 and Pilates
p = 0.028. Conclusion: The Pilates method proved to be more efficient,
both in terms of functionality regarding fatigue and balance, as well as in
quality of life, showing physical and mental improvement.
Keywords: multiple sclerosis;
physiotherapy; Pilates; quality of life; rehabilitation.
Resumo
Introdução: A Esclerose Múltipla (EM) é uma doença
autoimune crônica que afeta o Sistema Nervoso Central, causando destruição da
mielina e, como muitas doenças autoimunes, acredita-se que seja causada por uma
combinação de fatores ambientais e genéticos. Objetivo: Avaliar a
influência da fisioterapia convencional e do método Pilates em pacientes com
Esclerose Múltipla Remitente Recorrente (EMRR) nas atividades diárias e na
qualidade de vida. Métodos: Foram analisamos retrospectivamente 25
prontuários de pacientes com EMRR submetidos a Pilates (grupo A com 12
pacientes) e fisioterapia convencional (grupo B, com 13 pacientes), sendo que
cada grupo utilizou apenas uma técnica, no período de 2018 a 2019. Foram
comparados os dados obtidos por meio da Escala de Equilíbrio de Berg, Escala
Modificada do Impacto da Fadiga (MFIS), Medical Research
Council Scale (MRC) e
Escala de Qualidade de Vida na Esclerose Múltipla (MSQOL-54). Resultados:
Com o nível de significância adotado para p < 0,05, pelo teste de Wicoxon, obteve-se MFIS: convencional p = 0,030 e Pilates p
= 0,005; BERG: convencional p = 0,015 e Pilates p = 0,004; MSQOL (Físico):
convencional p = 0,263 e Pilates 0,009; MSQOL (Mental): convencional p = 0,807
e Pilates p = 0,028. Conclusão: O método Pilates se mostrou mais
eficiente, tanto na funcionalidade referente à fadiga e equilíbrio, quanto na
qualidade de vida, apresentando melhora física e mental.
Palavras-chave: esclerose múltipla; fisioterapia;
Pilates; qualidade de vida; reabilitação.
Introduction
Multiple sclerosis is a chronic,
autoimmune disease that affects the central nervous system, causing destruction
of myelin, a fundamental protein in the transmission of nerve impulse. The main
areas of the Central Nervous System affected by MS are the periventricular
areas of the brain, optical formations, cerebellum, brainstem and spinal cord
[1].
In Brazil, around 40 thousand
people are affected by MS [3], and in the world according to the International
Federation of Multiple Sclerosis, there are about 2.8 million people with the
disease [2]. It is the most common among demyelinating disorders, and although
it can manifest itself in both sexes and at any time in life, it is more
prevalent between the ages of 20 and 40, and women are twice most affected as
men [3].
The clinical manifestations are
varied and determined by the location of the lesions, and include paresis,
spasticity, gait disorders, intentional tremor, visual disturbances, fatigue,
bladder and intestinal disorders, sensory disorders, sensory and/or drunken
ataxia, nystagmus and cognitive disorders [4].
The benefits of regular physical
exercise for healthy people and the prevention and treatment of various
diseases has been proven by numerous studies [5].
Currently observe the use of
aerobic exercise, muscle strengthening or flexibility in the search for a
better quality of life for all people [6].
In the case of MS, the
implementation of physical exercise programs has only recently started to be
considered. In the last two decades, several researches have provided
encouraging evidence so that these people can engage in body practices, safely
and achieving improvements in physical fitness and in some symptoms attributed
to the disease [7].
Studies indicate that interventions
such as physical therapy and therapeutic physical exercises can improve many of
the deficiencies observed in MS. However, the effectiveness of these
interventions is not always proven in functional aspects. An overview of the
rehabilitation strategies developed for autoimmune diseases, identified as the
main components in the rehabilitation of MS the increase of the physical
capacity, muscular strength, aerobic resistance and functional abilities [4].
Since MS accommodates a wide range of symptoms, the rehabilitation of these
patients requires a multidisciplinary approach, with more satisfactory results
being observed in the techniques that demonstrate the use of sensory strategies
[5].
Physical exercise is an important
non-pharmacological tool in the rehabilitation of MS. Contrary to previous
belief, exercise is well tolerated and induces beneficial effects in patients
with MS. Studies examining resistance training are, in general, of low
methodological quality, which makes it difficult to draw solid conclusions
about the effects of this training modality. However, resistance formation with
moderate intensity appears to be well tolerated and has beneficial effects in
patients with moderate disabilities [6].
Some scales are used to quantify the evolution of the
patients, just like MFIS (modified fatigue impact scale) for fatigue, Berg
balance scale for balance, MSQOL-54 (multiple sclerosis quality of life – 54)
for quality of life, MRC (medical research council) for strength evaluation.
Objective
To compare the benefits of
conventional physical therapy and Pilates method in fatigue, strength, balance
and quality of life in patients with multiple sclerosis.
Methods
Type of study
We retrospectively analyzed 25
medical records of MS patients undergoing rehabilitation program between 2018
and 2019, using the MFIS, MRC, BERG and MSQOL-54 scales. It was approved by the
Ethics Committee in Research by the number 3.635.962 from ABC Federal
University, in 2019.
Evaluation methods
The MFIS, BERG, MRC and MSQOL-54
were chosen because they were valid instruments for multiple sclerosis and
fatigue, balance and strength are common symptoms.
The Modified Fatigue Impact Scale
(MFIS) is one of the most used scales to assess fatigue, it consists of 21
questions divided into: physical (9), cognitive (10), psychosocial (2),
allowing scores of 0 to 4 for each item. The result is given by the sum of the
scores of the three domains, and varies from 0 to 84. A score under 38 means no
fatigue and above this value until the higher the score, a strong fatigue [7].
The Medical Research Council (MRC)
aims to assess muscle strength, analyzing movements of the main muscle groups,
and the absence or presence of muscle contraction, ranging from 0 = no
contraction to 5 = normal muscle strength [8].
The Berg Balance Scale evaluates a
quantitative description of the functional balance skill in 14 items common to
daily life. In this case the higher the score means a better result. Each item
has an ordinal scale that varies from 0 to 4 points, with a score of 56 being
the maximum achieved. A score below 44 points is described as a predictor of
falls in MS [9].
The MSQOL-54 is the first specific
instrument applied to MS. This scale is a modification of the SF-36, with the
addition of 18 specific questions. There are 52 items grouped into 12 subscales
and two distinct questions that deal with changes in health status and the
patient's assessment of satisfaction with sexual function [10].
Protocol
The sample were divided into two
groups: Group A with Pilates intervention and Group B with conventional
physical therapy.
Protocol Group A: muscle
strengthening of the lower limbs, upper limbs and trunk, balance training,
central stabilization and posture) with the participation of 12 patients.
Protocol Group B: muscle
strengthening of lower limbs, upper limbs and trunk, global stretching, static
and dynamic balance training) with the participation of the other 13 patients.
The evaluations of Pilates and
physical therapy training were performed before the beginning of the treatment
and 4 months later, after 16 sessions, once a week, for 1 hour.
Some other information were collected, such as age, gender, time of diagnosis, EDSS
degree (from 0 to 6.5), medication used and rehabilitation time, contained in
the medical records of these patients with an informed consent form signed by
the participant, authorizing the collect of data from medical records.
Inclusion criteria
As inclusion criteria, all the
medical records of patients who started physical therapy in 2018 were analyzed.
Participants signed the Informed Consent Form.
Exclusion criteria
Patients who did not undergo
physical therapy at the institution or the ones who suffered outbreaks during
the rehabilitation process.
Statistical analysis
Qualitative variables were
presented by absolute frequency and relative frequency. Quantitative variables
were presented by measures of position and measures of variability using the
normality test of the Shapiro-Wilk test data.
The McNemar
test was used to compare the evolution of muscle strength of upper and lower
limbs before and after sessions in both physical therapy and Pilates groups.
The Wilcoxon test was used to correlate muscle fatigue (MFIS), balance (Berg
Balance Scale) and quality of life (physical and mental aspects with MSQOL-54)
before and after therapy performed by physical therapy and Pilates groups. The
EDSS classification and muscle strength of the upper and lower limbs were also
associated with the Chi-square test. In all analyzes, the level of significance
adopted was p ≤ 0.05. The statistical program used was Stata version
11.0.
Results
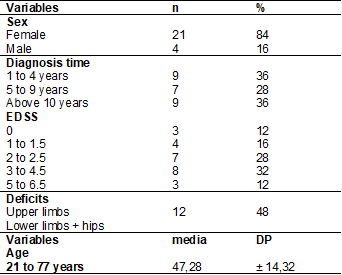
The participants in this study were
aged between 21 and 77 years. There were 25 participants, 21 were female (84%)
and 4 were male (16%). The degree of EDSS ranged from 0 to 6.5. As shown in
Table 1, the muscle group that suffered the most involvement was the lower
limbs and the hip, affecting 96% of the participants, while the upper limbs are
affected in 48% of the participants.
Table I - Characterization of the
sample
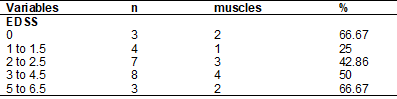
When we compare EDSS and the
impairment in muscle strength, we observe that the higher degree of EDSS takes
a greater tendency to affect muscle strength, as shown in Table 2. The degree
zero, showed a high index, due to one of the participants presenting associated
hemiparesis, causing a decrease in muscle strength.
Table II - Comparison between degree of
EDSS and impairment in muscle strength
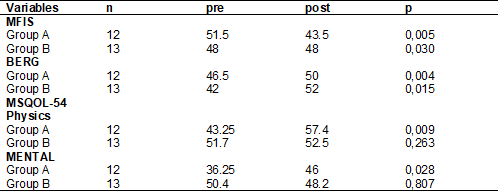
From the data presented in Table
III, we found that the two methods proved to be efficient in improving
patient’s fatigue, in this case, the Pilates method showed better results
compared to the conventional method. In the balance assessment, we verified
that both methods showed improvement, again the methods showed improvement,
with the Pilates method having better efficiency. The quality of life analysis
was subdivided into two parts, Physical Health and Mental Health, in both,
conventional physical therapy did not show significant improvement and the
opposite occurred with Pilates method.
Table III - Comparison of the rating
scales with the results of the medians of pre and post Pilates and physical
therapy sessions (Wilcoxon Text)
Discussion
In this study, we found a
significant improvement in balance and a reduction in fatigue through the
practice of exercises, with conventional physical therapy and the Pilates
method.
This study is relevant for clinical
practice because elucidate different types of therapies to the improvement of
multiple sclerosis patients and there is no other study that compare the
benefits between Pilates and physical therapy. Regular therapeutic exercise is
particularly important, to improving muscle strength; it is designed to improve
endurance, muscle tone, postural stability, and flexibility. Any program must
be adapted to the needs and symptoms of an individual patient [11].
Especially when we think about
patients with RRMS, each patient, depending on their EDSS degree, has a degree
of physical and emotional involvement, for this reason the Pilates method is
very well accepted, bringing body awareness, increasing the level of
concentration and spatial perception, improving balance, controlling muscle
strength and consequently improving functionality and quality of life, as we
can see in the results of this study.
Highlighting the benefits obtained
by methods like Pilates in neurological dysfunctions are attributed to the
ability that this practice has to work the balance between the mind and the
body in a global and non-segmented way. Benefits that can positively influence
the recovery and maintenance of brain capacity with the consequent activation
of neuronal cells necessary for carrying out the most diverse functional
activities [12].
However, physical therapy is also
important for improvement of physical conditions of patients with MS, especially
in balance issues, comparing pre and post intervention studies [13].
We provide them with better
conditioning, pain relief, through stretching, which can contribute to
improving great spasticity and muscle stiffness, greater independence and improvement
in the performance of their activities of daily living and prevention of future
injuries [14].
Conclusion
With the data obtained in this
sample analyzed, we understand that physical activity is an important ally to
improve the quality of life of patients with RRMS, the two methods studied
showed good results.
More studies are still needed to
prove the effectiveness of physical activities in people with MS, as well as to
evaluate other techniques and other methods.
Conflitos
de interesse
Não
há conflito de interesses
Fontes
de financiamento
Não
houve financiamento
Contribuição
dos autores
Concepção
e desenho da pesquisa:
Telles JAR, Dias AE; Coleta de dados: Nakau
ET, Castro IS; Análise e interpretação dos dados: Telles JAR, Nakau ET, Castro IS, Labronici
RHD; Análise estatística: Labronici RHD; Redação
do manuscrito: Telles JAR, Nakau ET, Castro IS; Revisão
crítica do manuscrito quanto ao conteúdo intelectual importante: Telles
JAR, Dias AE, Labronici RHD
References
- Dobson R, Giovannoni G.
Multiple Sclerosis - an review. Eur J Neurol.
2019;26(1):27-40. doi: 10.1111/ene.13819 [Crossref]
- The atlas of multiple sclerosis. 3rd ed. [cited 2023
mar 8]. Available from:
https://www.msif.org/wp-content/uploads/2020/10/Atlas-3rd-Edition-Epidemiology-report-EN-updated-30-9-20.pdf
- Harbo HF, Gold R, Tintoré M. Sex and gender issues in multiple sclerosis. Ther Adv Neurol Disord. 2013;6(4):237-48. doi: 10.1177/1756285613488434 [Crossref]
- Oh J, Vidal-Jordana A, Montalban X. Multiple Sclerosis: clinical aspects. Curr Opin Neurol. 2018;31(6):752-9. doi: 10.1097/WCO.0000000000000622 [Crossref]
- Reynolds ER, Ashbaugh AD, Hockenberry BJ, McGrew CA. Multiple sclerosis and exercise: a literature review. Curr Sports Med Rep. 2018;17(1):31-5. doi: 10.1249/JSR.0000000000000446 [Crossref]
- Kim Y, Lai B, Mehta T, Thirumalai M, Padalabalanarayanan S, Rimmer JH, Motl RW. Exercice trining guidelines for Multiple Sclerosis, Stroke and Parkinson Disease: rapid review and synthesis. Am J Phys Med Rehabil. 2019;98(7):613-21. doi: 10.1097/PHM.000000000000117 [Crossref]
- Halabchi F, Alizadeh Z, Sahrajan MA, Abolhasani M. Exercise prescription for patients with multiple sclerosis: potential benefits and practical recommendations. BMC Neurol. 2017;17(1):185. doi: 10.1186/s12883-017-0960-9 [Crossref]
- Camargo, L.; Preira, C. Dispneia em DPOC: além da escala modified medical research council. J. Bras. Pneumol. 2010;36(5). doi: doi: 10.1590/S1806-37132010000500008 [Crossref]
- Flachenecker P. Autoimmune diseases and rehabilitation. Autoimmun Rev. 2012;11(3):219-25. doi: 10.1016/j.autrev.2011.05.016 [Crossref]
- Lindroth JL,
Sullivan JL, Silkwood-Sherer D. Does hippotherapy effect use of sensory
information for balance in people with multiple sclerosis. Physiother
Theory Pract. 2015;31(8):575-81. doi: 10.3109/09593985.2015.1067266 [Crossref]
- Dalgas U, Stenager E, Ingemann-Hansen T.
Multiple sclerosis and physical exercise: recommendations for the application
of resistance-, endurance- and combined training. Mult
Scler. 2008;14(1):35-53. doi: 10.1177/1352458507079445 [Crossref]
- Pavan K, Schmidt K, Marangoni B, Mendes MF, Tilbery CP, Lianza S. Multiple sclerosis: cross-cultural adaptation and validation of the modified fatigue impact scale. Arq Neuropsiquiatr. 2007;65(3A):669-73. doi: 10.1590/s0004-282x2007000400024 [Crossref]
- Miyamoto ST, Lombardi Junior I, Berg KO, Ramos LR, Natour J. Brazilian version of the Berg balance scale. Braz J Med Biol Res. 2004;37(9):1411-21. doi: 10.1590/s0100-879x2004000900017 [Crossref]
- Kalron A, Rosenblum U, Frid L, Achiron A. Pilates exercise training vs. physical therapy for improving walking and balance in people with multiple sclerosis: A randomized controlled trial. Clinical Rehabilitation. 2916;31(3):319-28. doi: 10.1177/0269215516637202 [Crossref]
