Fisioter Bras.
2023;24:(5):564-79
ORIGINAL ARTICLE
Pilates method in low back pain: a randomized clinical
trial
Método
Pilates na dor lombar: um ensaio clínico randomizado
Idemar Rodrigues dos Santos Júnior, Rebecca Rickelle de Souza Mousinho, Nivaldo Antonio
Parizotto, Carina Carvalho Correia Coutinho
Universidade
Federal da Paraíba, João Pessoa, PB, Brasil
Received: March 21,
2022; Accepted: August 12, 2023.
Correspondence: Carina Carvalho Correia Coutinho, carina.caarvalho@gmail.com
How to cite
Santos Júnior IR, Mousinho RRS, Parizotto
NA, Coutinho CCC. Pilates method in low back pain: a randomized
clinical trial. Fisioter Bras. 2023;2495):564-79. doi: 10.33233/fb.v24i5.5430
Abstract
Objectives: To analyze the
effectiveness of the Pilates ground method in individuals with chronic
non-specific low back pain (LBP) in reducing pain, improve the functionality,
strength of the transverse abdomen muscle and quality of life. Methods:
Double-blind randomized controlled trial in the University clinic. Thirty
volunteers of both sexes were allocated randomly to two groups of 15
participants each: Pilates (PG) with Pilates exercises, and Control (CG). The
PG held 16 sessions of 60 minutes, held twice a week for eight weeks.
Participants were assessed pre-treatment and post-treatment for pain (Numerical
Pain Scale - NPS and McGill Pain Questionnaire -MPQ), functional disability (Oswestry), transverse abdomen muscle strength (TrA) by the biofeedback unit test pressure (BTP)
(Chattanooga Group, Australia) and quality of life by Medical Outcomes Study
36- Item Short-form Health Survey (SF-36). Results: There was a
statistically significant increase in TrA (p <
0.001) and a significant reduction in pain intensity plus qualification (p <
0.001) and functional disability (p < 0.001), as well as an increase in
quality of life (p < 0.001). A positive correlation was observed between
functional disability and pain assessed by Visual Anagolic
Scale (VAS) (rho = 0.773; p = 0.001), as well as a negative correlation between
disability and quality of life assessed by SF-36 (rho = -0.589; p = 0.021). Conclusion:
The present study suggests that Mat Pilates exercises may be a choice for the
treatment of patients with chronic non-specific low back pain.
Keywords: low back pain; exercise therapy;
quality of life; rehabilitation.
Resumo
Objetivos: Analisar a eficácia do método Mat Pilates em indivíduos com dor lombar crônica
inespecífica (DLCI) na redução da dor, e sua correlação na funcionalidade,
força do músculo transverso do abdômen e qualidade de vida. Métodos:
Ensaio Clínico controlado randomizado duplo-cego, realizado em clínica
universitária. Trinta voluntários de ambos os sexos foram alocados
aleatoriamente em dois grupos de 15 participantes: Grupo Pilates (GP) com exercícios
de Mat Pilates; e Grupo Controle (GC) sem
intervenção. O Grupo Pilates realizou 16 sessões de 60 minutos, duas vezes por
semana durante oito semanas. Os participantes foram avaliados pré-tratamento e
pós-tratamento para dor (Numerical Pain Scale - NPS e McGill Pain Questionnaire
-MPQ), incapacidade funcional (Oswestry), força
muscular transversa do abdome (TrA) pelo biofeedback unit test pressure (BTP) (Chattanooga Group, Austrália) e qualidade de vida (Medical Outcomes Study 36- Item Short-form Health Survey (SF-36).
Resultados: Houve aumento estatisticamente significativo na força do transverso
do abdomen (p < 0,001) e redução significativa na
intensidade e qualidade da dor (p < 0,001) e incapacidade funcional (p <
0,001), além de aumento na qualidade de vida (p < 0,001) no Grupo Pilates.
Observou-se correlação positiva entre incapacidade funcional e dor avaliada
pela Escala Visual Analógica (EVA) (rho = 0,773; p =
0,001), assim como correlação negativa entre incapacidade e qualidade de vida (rho = -0,589; p = 0,021). Conclusão: O presente
estudo sugere que os exercícios de Pilates podem ser uma escolha para o
tratamento de pacientes com dor lombar crônica inespecífica.
Palavras-chave: lombalgia; terapia por exercício;
qualidade de vida; reabilitação.
Introduction
Low back pain, according to the
Global Burden of Disease (GBD), is considered the leading cause of disability
in the world [1]. In Brazil, it represents the second largest complaint of pain
in the population [2], and the prognosis is considered moderately favorable
when presenting 41% of patients with remission in 12 weeks, however, for the
others, after a period of six weeks, the clinical status improve and the
intensity vary from low to medium of disability, and pain are installed
persistently and present over a year (chronically) [2].
The European Guide to Clinical
Practice [3] recommends supervised exercises for the treatment of non-specific
LBP and several studies indicate that precise and specific exercises aimed to
activating and strengthening the transverse muscle of the abdomen and other
spinal stabilizers reduce the recurrence of spinal dysfunctions [4,5,6]
One of the exercises that has gained popularity among
individuals with low back pain is the Pilates method [7,8], which uses
contractions of the transverse abdomen and multiple muscles combined with
diaphragmatic breathing, as a basis for treating pain and promoting improvement
of functional capacity in people with chronic LBP [9,10,11]. Some studies have
observed the influence of the method in patients with chronic non-specific low
back pain [12]
Wells et al. [13], in a
systematic review, showed efficacy of the Pilates method in promoting the
reduction of pain and functional disability in short term when compared to
usual care and regular physical activities. Da Luz et al. [14] compared
the effects of Pilates apparatus and Mat Pilates in patients with chronic
non-specific LBP, categorized the exercises into levels and analyzed the
effects of the method along with variables such as pain, disability and kinesiophobia, concluding that both forms are effective in
the variables he studied in the short term.
In another systematic review it can
be concluded that there is evidence of low to moderate quality that Pilates
provides better results than minimal intervention, as well as there is no
conclusive evidence that Pilates is superior to other forms of exercise [15].
Among the randomized controlled studies that related the Pilates method and the
LBP, it was not possible to observe concise, significant and reliable results
due to the difference in the methodological criteria such as: heterogeneity of
the sample, brief or absence of description of the exercises performed, in
addition to differences is the number and frequency of the sessions due to the
lack of specific protocols for the clinical condition [16].
More, high-quality studies are
needed to evaluate Pilates for LBP. Therefore, this research aims to analyze
the effects of ground exercises proposed by the Pilates method compared to no
intervention in individuals with chronic non-specific LBP, analyzing pain,
functional disability, quality of life and activation and strength of the
transverse muscle of the abdomen, observing the clinical relevance of this
treatment, providing evidence to professionals and assisting in clinical
decision making.
Methods
Study design
This is a randomized, double blind
clinical trial. The study was approved by the Research Ethics Committee of the
Health Sciences Center of the Federal University of Paraíba
under protocol number 0666/15. CAAE: 51317315.2.0000.5188, in compliance with
resolution 466/12 of the National Health Council. The study was registered on
Clinical Trials under NCT02922322.
Participants
It was included in the study
participants of both sexes, between 18 and 60 years old, with a diagnosis of
chronic non-specific LBP lasting more than three months, without root symptoms
for more than 12 months, and NRS [17] greater than 3 (0/10). Contraindications
for physical exercise were assessed using the Physical Activity Readiness
Questionnaire - PAR-Q [18] (Appendix A), suggested as a minimum
pre-participation assessment standard. This instrument can identify by some
positive responses the participants who need prior medical evaluation and
clearance.
The exclusion criteria were:
presenting degenerative or inflammatory diseases of the spine, acute crisis of
pain in the shoulders, knees and spine, vertebral tumors, unconsolidated
fractures or with vicious consolidation in the spine, shoulder and upper limbs,
recent surgeries in the spine, shoulder and upper limbs, herniated disc,
spondylolysis or spondylolisthesis; any other rheumatological disease, patients
who are in labor disputes, who practice activities involving the Pilates method
frequently, who are undergoing other types of physical therapy or medication
treatment. Also excluded are those who do not understand the writing and
speaking of the Portuguese language clearly. All volunteers signed an Informed
Consent Form (ICF) and were informed of the research procedures in accordance
with the World Medical Association’s Declaration of Helsinki. Those who agreed
to take part provided written informed consent, in line with Resolution
466/2012.
Randomization and blinding
The randomization of the research
was carried out through a simple randomization scheme following the guidelines
of CONSORT - CONsolidated Standards of Reporting
Trials, controlled (1: 1), whose randomization list was generated through the
website www.random.org/lists/ constituted by the numbers from 1 to 30, these
are randomly assigned to each research participant, after randomization 15
individuals for each group. The research randomization process was carried out
by an independent researcher who was not involved with the recruitment process
of the participants or with the evaluations.
Participants were divided into two
groups: Pilates Group (PG) and Control Group (CG). One researcher (R1) was
responsible for evaluations and reevaluations; the second researcher (R2), for
the randomization process, the third (R3) for the application of the
intervention protocol, and the fourth researcher (R4) for the statistical
analyzes. All researchers were shielded as to the other processes developed by
the other researchers.
The participants were instructed to
report any complaints, whether related to the exercises or not. Moreover, they
were asked not to modify their life routine and not to participate in any other
treatment program.
Procedures
A total of thirty participants were
included in the study and randomized into two groups: the Pilates Group (PG)
and the Control Group (CG).
Pilates Group
The Pilates Group (PG) program
consisted of 16 sessions, held twice a week for a period of eight weeks, each
session lasting approximately 60 minutes. The exercise program was carried out
and supervised by a researcher trained about the Pilates method, who was not
involved in other stages of the research. Patients were instructed to report
any complaints related or not to exercise during the intervention.
The intervention was based on 20 of
the 34 original solo exercises proposed by the Pilates method, classified as
basic, intermediate and advanced. The exercises were organized in four cycles
where each cycle consisted of 5 exercises introduced according to the degree of
difficulty (basic, intermediate and advanced), however, the exercises could
progress or regress according to the physical fitness of each participant. Each
cycle lasted four sessions, totaling 4 cycles with 20 exercises. Each exercise
was performed 10 times, with two series of repetitions, respecting the limit of
each patient.
Cycle I (Exercises 1-5) - Basic level;
Cycle II (Exercises 6-10) - Intermediate level;
Cycle III (Exercises 11-15) - Intermediate level.
Cycle IV (Exercises 16-20) - Advanced level.
Control group
The participants allocated to
participate in the CG received instructions to remain with the usual care and
not to practice any type of physical activity or physical therapy until the end
of the research. After the conclusion of the study, the volunteers who made up
the CG were allocated within the extension project “Prevention and care in low
back pain”, consisting of prevention and physical therapy activities for
individuals with LBP.
Outcome measures
The evaluations were made by the
blind evaluator, in person, applied pre-treatment and after the end of the 16
treatment sessions. All the instruments adopted are validated for Brazilian
Portuguese. Initially, the PAR-Q [18] instrument was applied to verify the
volunteers' ability to carry out the proposed activities.
The primary outcomes of pain
intensity and quality were collected using the Visual Pain Scale [19] and
McGill Pain Questionnaire [20], functional disability using the Oswestry Index [21] and quality of life using the Short
Form-36 validated by Ciconelli [22].
The secondary outcomes were abdomen
transverse muscle strength. The activation of the transversus abdominis muscle
(TrA) was evaluated using the Pressure Biofeedback
Unit (PBU) / Stabilizer Pressure Biofeedback (Chattanooga Group-USA) [23] which
consists of a pressure transducer with three inflatable bags, a catheter and a
sphygmomanometer that varies from 0-200 mmHg graduated every 2 mmHg. Changes in
body position will imply pressure changes in the bag that will be recorded by
the sphygmomanometer.
The volunteers were instructed to
fast for two hours before the start of the assessments (including water), in
addition to having to empty their bladder immediately before the test, and not
to perform abdominal exercises on the day before and on the day of the
assessment. Before the test, the participants received basic educational
information about anatomy, biomechanics and the function of the TrA, in addition to specific guidelines about an ideal
contraction of the TrA. All evaluations were
performed with the patient in prone position, where the ideal contraction of
the TrA consists of the movement of the abdominal
wall (infra-umbilical region) towards the spine, in a slow and controlled
manner, without movements of the trunk or pelvis, or contractions other muscles
such as gluteus, quadriceps or spine extensors. During the test, the bag is
positioned under the TrA with the participant in
prone position. The ability to depress the abdominal wall against the lumbar spine
results in a pressure reduction of 4-10 mmHg, that is, from 70 mmHg to 66-60
mmHg (optimal contraction of the TrA), which is
recorded by the PBU sphygmomanometer [24].
The measurement was performed with
the patient in prone position on a rigid surface below the trunk and abdomen to
minimize foam deformation. The lower limbs are positioned with the feet off the
stretcher and the arms at the side of the body, with the head turned to the
right and the bag is positioned in the space immediately above the
anterosuperior iliac spines on the umbilical scar and before start contraction,
the pressure bag is inflated to a pressure of 70 mmHg with the valve closed.
Participants were instructed to
perform two inspirations and exhalations using mainly the abdominal region. The
bag pressure is then adjusted again to 70 mmHg. To assist in the execution of
the movement, the verbal command will be given: “With the lower abdomen inward
without moving the spine and pelvis and keep it”. These contractions must be
maintained for at least ten seconds, measured by the timer. Participants were
instructed to perform slow inhalation and exhalation, and contraction of the TrA was performed concurrently with exhalation.
Sample size
The sample size was calculated
considering a statistical power of 80%, standard deviation of two data points,
and 20% improvement in pain intensity [25], by G-POWER. As a result, 15
patients were required per group, with parameters of a 5% significance level
and 15% sample loss.
Statistical analysis
The data were analyzed using the
Statistical Package for Social Sciences v.2.0 (SPSS). Descriptive statistics
were performed obtaining of absolute and relative frequency values, and
measures of central tendency and variability. Initially, the Shapiro-Wilk
normality test was performed to observe the distribution of values in each of
the study variables, in order to choose the most suitable tests for each
analysis.
Comparisons between groups with
regard to the mean age, mass, height and body mass index were performed using
the unpaired t test. For the paired analyzes of the two assessments made in
each group, the paired t tests (normal distribution) or the paired Wilcoxon
(non-normal distribution) were used. Spearman's correlation test was also
performed among all variables studied. The level of significance used in this
study was 5% and the confidence interval was 95%.
Results
Thirty-five individuals with
chronic low back pain were assessed at baseline, and of these, 5 were excluded for
not achieving the inclusion criteria. In total, 30 individuals (24 women and 6
men) were chosen and randomly allocated to the Pilates Group (PG; n = 15) and
Control (CG; n = 15) groups. A total of 240 sessions were offered with 92.91%
of these being recorded, with 17 absences to the total number of participants
in the Pilates group (Figure 1)
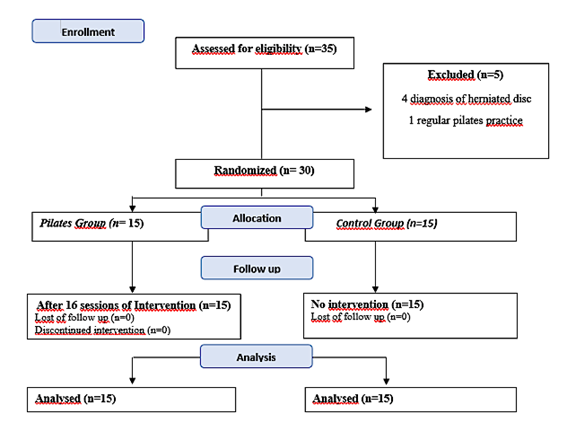
Figure 1 - Flowchart of the randomized
clinical trial
In the table I we can see how homogeneous is the
population in comparison between variables.
Table I -. Sociodemographic
characteristics of study participants
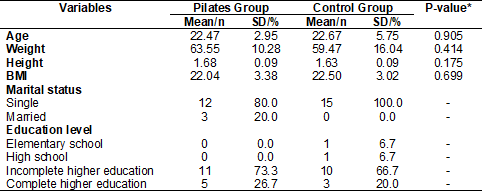
*Unpaired t-test
There was a significant reduction
in pain (p < 0.001) in the mean values obtained in the VAS in the PG, which
was not observed in the CG. In the same way, it was also observed in the PG a
significant decrease in pain measure by the MPQ, both in the total score (p
< 0.001) and in the sensory (p < 0.001) and affective (p < 0.001)
components. This same finding was not observed in the CG (Figure 2).
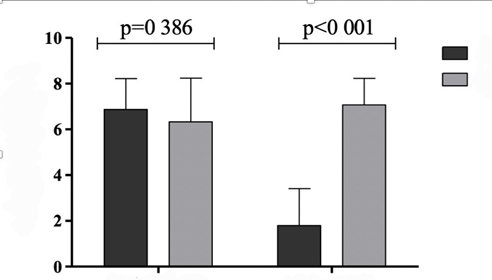
Figure 2 - Comparison graph between the
means of the Visual Analogue Scale (VAS) scores obtained in each group of the
study
There were improvements in quality
of life (SF-36) after the Pilates sessions (p = 0.001). The assessment of
disability, in the PG the scores obtained by the Oswestry
Index increased significantly after the intervention as shows the present study
(p < 0.001), in the Table II.
Table II - Comparison between the Oswestry Index scores obtained at two time points in both
groups

In the evaluation of the activation
of TrA, in the PG there was a significant decrease in
the pressure quantified in this test (p < 0.001), which was, on average,
66.53 mmHg (SD = 1.36) in the baseline and changed to 59.40 mmHg (SD = 4.10) on
the final of treatment. In the CG, the values were quite similar in the two
evaluations (Table III).
Table III - Comparison between the
quantified values in the assessment of the transversus abdominis muscle (TrA) at two research moments in both groups

*Unpaired t-test
A positive correlation was observed
between functional disability and pain assessed by VAS (rho = 0.773; p =
0.001), as well as a negative correlation between disability and quality of
life assessed by SF-36 (rho = -0.589; p = 0.021) (Table IV).
Table IV - Correlation coefficients
between pain, quality of life, functional disability (Oswestry),
and transversus abdominis muscle activation after treatment in the Pilates
group
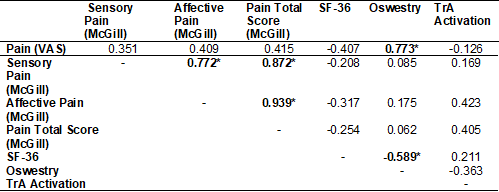
VAS = Visual Analogue Scale; McGill
= McGill Pain Questionnaire; SF-36 = Quality of life instrument; TrA = transverse abdominal muscle; *p < 0.05; Spearman
correlation test
Discussion
This study shows that in the
short-term Mat Pilates presents statistically significant results and
clinically relevant effects for the primary and secondary outcomes studied in
this clinical trial, when compared with no intervention.
The methodological approach used
became possible to verify the expressive results in relation to the real
effectiveness and impact of Mat Pilates along with factors such as quality of
life, pain, disability and activation of the TrA,
stabilizer of lumbar spine, in
individuals with non-specific low back pain, presenting low risk of bias, since
it was based on the guidelines of randomized clinical trials, following the CONSORT,
thus being able to help physiotherapists in their clinical practice decision
process.
In our research, the homogeneity of
the subjects was maintained, verified through the comparison of demographic
data. There was a predominant participation of women in the young-adult age
group, and this may be explained by the physiological characteristics of less
muscle and bone mass in the female sex. In this age group, there is a full
productive phase, greater occupational and domestic demand, which burden the lower
back, mainly due to important changes in lifestyle at home and in the work
environment, such as the constant use of computers, increasing sedentary
lifestyle, risk factor for the development of chronic low back pain [26].
The body mass index (BMI) in this
study is within normal parameters in both groups, in contrast to some published
studies that mentioned that overweight/obesity would be prevalent in
individuals with low back pain [27,28]. This overweight – low back pain
relationship was not observed in our research, however, some studies suggest
that this is a factor to be considered, as obesity promotes an increase in the
overload of articular structures of the lumbosacral spine, which may predispose
to degeneration [29].
The treatment for nonspecific low
back pain has the Pilates Method exercises (Mat Pilates) as a rehabilitation
tool, which is composed as a set of exercises focused on stabilization,
breathing and abdominal strength. In a recent systematic review, Byrnes, Wu and
Whillier [30] found that Pilates is an effective
rehabilitation tool in achieving the desired results, especially in reducing
pain and functional incapacity in the various pathologies studied. In addition,
this review indicates the need for more research to indicate the benefits of
certain Pilates exercises in rehabilitating specific conditions.
In our study Mat Pilates was
considered an important and effective treatment tool for patients with
nonspecific low back pain when compared to no intervention. This can be
explained by the fact that we promoted the adequate evolution of the exercises,
and for this, 20 of the 34 original exercises developed in the field and
described by Joseph Pilates in his book “Return to Life through Contrology” in
1945 [31], were selected and divided in 4 cycles according to the level of
difficulty, taking into account the biomechanics and muscle actions in all
phases of the exercises.
It is known that the exercises
proposed by Mat Pilates, when well executed and properly evolved, improve the
stability of the spine through the complex interaction of muscles, connective
tissue and joint structures [32]. It is possible to observe an increase in
muscle control around the spine, which is necessary to maintain functional
stability. We saw that the mean TrA strength after
the intervention with Mat Pilates increased to 10.6mmHg, a value in addition to
the variation established by Hodges and Richardson [24] by electromyography,
which would be between 4-10 mmHg, however, this increase is confirmed in the
study by Ceccato et al. [33] when using this
sphygmomanometer to assess the TrA strength in young
rowers, reaching values of 19 mmHg. According to this author, this finding can
be justified due to the action of other spinal stabilizer muscles, such as the
multifidus and oblique muscles, which, when activated, help to reduce
intra-abdominal pressure during the test.
It is known that the lack of muscle
strength, endurance or control can allow the emergence of inappropriate or
excessive segmental movements, in addition to repeated trauma to tissues within
or around the spine, causing activation of nociceptors and resulting in pain
[32].
These results were achieved after
performing 16 Mat Pilates sessions held twice a week for a period of eight
weeks, each session lasting approximately 60 minutes, corroborating the
systematic review by Yamato et al. [34], whose duration of all Pilates
sessions analyzed it was approximately one hour for all included studies, and
the mean number of sessions in the included studies was 15.3, ranging from six
to 30 sessions.
The difference of 5.07 points (p
< 0.001) in the VAS after the intervention with Mat Pilates compared to no
intervention was a clinically important result, in addition to the
statistically significant reduction in the results of the McGill Pain
questionnaire, in the domain of affective and sensory. Also the data obtained
through the Oswestry Index and the components of the
SF-36 questionnaire, in which it was observed that the domain “functional
capacity”, as opposed to disability and “pain”, obtained statistically
significant responses (Table IV), respectively, according to the SF-36,
indicating a direct association between the reduction of pain and disability
and the overall improvement in the quality of life of individuals with low back
pain intervened by Mat Pilates.
The correlations between the
variables analyzed confirmed the study hypothesis: positive correlations
between the domains of the SF-36 questionnaire and negative when compared to
data in which higher values meant worsening of the studied variables, such as
the strength of the TrA which increased while the
disability decreased. The same was observed between the SF-36 and the Owestry Index, indicating that the improvement in quality
of life implies an improvement in functional capacity of this patients.
The results of the present clinical
trial confirmed the data compiled by the systematic review by Kamioka et al. [34], which showed that the vast
majority of randomized clinical trials published so far obtained a positive
response from Pilates to LBP in a short period of time.
Our study suggests that Mat Pilates
is effective in reducing the levels of pain obtained by the VAS and the McGill
Questionnaire, as well as it is possible to observe the improvement in aspects
of quality of life in reducing the pain and functional disability of these
individuals. The strength of the transverse muscle of the abdomen had a
positive correlation with the improvement of all variables studied in this
research.
In a recent systematic review [35],
the authors concluded that there is no conclusive evidence that Pilates
is
superior to other forms of exercise due to the low to moderate quality
of
published studies, but there is evidence that Pilates is more effective
than an
intervention minimal or no intervention for pain and functional
disability. Our study used a good methodology, based on the Consort,
and as seen in
the data found, Mat Pilates can be considered effective for reducing
pain and
functional disability in patients with low back pain, despite having
been
applied in a small sample, therefore, we suggest carrying out studies
with the
methodological rigors adopted here with a larger number of participants.
Conclusion
The research results show that Mat
Pilates has positive responses in the quality of life, pain, disability and
activation and transverse muscle strength of individuals with unspecific
chronic low back pain compared to people who were not intervened by the method.
However, the study needs confirmation of these implications in the medium and
long term after the intervention, since other research claims positive results
only for short duration.
Funding
This research did not receive any
specific grant from funding agencies in the public, commercial, or
not-for-profit sectors.
Conflicts of interest
The authors declare no conflicts of
interest.
Authors' contribution
Conception and design
of the research: Coutinho CCC, Santos IR; Data
collection: Coutinho CCC, Santos IR; Data analysis and interpretation:
Coutinho CCC, Santos IR, Parizotto NA; Statistical
analysis: Coutinho CCC, Santos IR; Manuscript writing: Coutinho CCC,
Santos IR; Mousinho RRS, Parizotto
NA; Critical review of the manuscript for important intellectual content:
Coutinho CCC, Santos IR, Parizotto NA
References
- Institute for Health Metrics and Evaluation (IHME).
Findings from the Global Burden of Disease Study 2017. Seattle, WA: IHME, 2018.
- IBGE - Brazilian Institute of Geography and
Statistics. National Household Sample Survey. An overview of health in Brazil:
access to and use of services, health conditions and risk and protection
factors for health, 2008. IBGE: Rio de Janeiro; 2010.
- Airaksinen O, Brox JI, Cedraschi C, Hildebrandt
J, Klaber-Moffett J, Kovacs F, et al. Working Group
on Guidelines for Chronic Low Back Pain. Chapter 4. European guidelines for the
management of chronic nonspecific low back pain. Eur Spine J. 2006;15(Suppl2):S192-300. doi: 10.1007/s00586-006-1072-1 [Crossref]
- Comerford MJ, Motram SL. Movement and stability dysfunction – contemporary developments. Man Ther 2001;6:15-26. doi: 10.1054/math.2000.0388 [Crossref]
- O'Sullivan PB, Phyty GD, Twoney LT, Alison GT. Evaluation of specific stabilizing exercise in the treatment of chronic low back pain with radiologic diagnosis of spondylolysis or spondylolisthesis. Spine. 1997;22(24):2959-67. doi: 10.1097/00007632-199712150-00020 [Crossref]
- Hides J, Richardson C, Jull G. A multifidus muscle recovery is not automatic after resolution of acute, first episode low back pain. Spine. 1996;21:2763-2769. doi: 10.1097/00007632-199612010-00011 [Crossref]
- Fonseca JL, Magini M, De Freitas TH. Laboratory gait analysis in patients with low back pain before and after a Pilates intervention. J Sport Rehabil. 2009;18:269-82. doi: 10.1123/jsr.18.2.269 [Crossref]
- Rydeard R, Leger A, Smith D. Pilates-based therapeutic exercise: effect on subjects with nonspecific chronic low back pain and functional disability: a randomized controlled trial. J Orthop Sports Phys Ther. 2006;36:472-84. doi: 10.2519/jospt.2006.2144 [Crossref]
- Gladwell V, Head S, Haggar M, Beneke R. Does a program of Pilates improve chronic non-specific low back pain? J Sport Rehabil. 2006;15:338-50. doi: 10.1123/jsr.15.4.338 [Crossref]
- Curnow D, Cobbin D, Wyndham J, Boris STC. Altered motor control, posture and the Pilates method of exercise prescription. J Bodyw Mov Ther. 2009;13:104-11. doi: 10.1016/j.jbmt.2008.06.013 [Crossref]
- Quinn K, Barry S, Barry L. Do patients with chronic low back pain benefit from attending Pilates classes after completing conventional physiotherapy treatment? Physiother Ireland. 2011;32:5-12. doi: 10.3233/PPR-2011-32102 [Crossref]
- Rajpal N, Arora M, Chauhan V. The study on efficacy of
Pilates and McKenzie exercises in postural low back pain -- a rehabilitative
protocol. POTJ. 2008;1:33-56.
- Wells C, Kolt GS, Marshall P, Hill B, Bialocerkowski A. The effectiveness of Pilates exercise in people with chronic low back pain: a systematic review. PLoS One. 2014;9:e100402. doi: 10.1371/journal.pone.0100402 [Crossref]
- Luz MA, Costa LOP, Fuhro FF, Manzoni ACT, Oliveira NTB, Cabralet CMN. Effectiveness of mat Pilates or equipment-based Pilates exercises in patients with chronic nonspecific low back pain: a randomized controlled trial. Phys Ther. 2014;94:623-631. doi: 10.2522/ptj.20130277 [Crossref]
- Yamato T, Maher C, Saragiotto B, Hancock M, Ostelo R, Cabral C, Costa LC, Costa L. Pilates for low back pain: complete republication of a cochrane review. Spine. 2016;41:1013-1021. doi: 10.1097/BRS.0000000000001398 [Crossref]
- Miyamoto GC, Costa LOP, Galvanin T, Cabral CMN. Efficacy of the addition of modified Pilates exercises to a minimal intervention in patients with chronic low back pain: a randomized controlled trial. Phys Ther. 2013;93:310-20. doi: 10.2522/ptj.20120190 [Crossref]
- Costa LO, Maher CG, Latimer J, Ferreira PH, Ferreira ML, Pozzi GC, Freitas LM. Clinimetric testing of three self-report outcome measures for low back pain patients in Brazil: which one is the best? Spine. 2008;33(22):2459-2463. doi: 10.1097/BRS.0b013e3181849dbe [Crossref]
- Luz LGO, Farinatti PTV. Questionário de Prontidão para Atividade Física (PAR-Q). Rev Bras Fisiol Exerc. 2009;4(1):43. doi: 10.33233/rbfe.v4i1.3585 [Crossref]
- Williams VS, Morlock RJ, Feltner D. Psychometric evaluation of a visual analog scale for the assessment of anxiety. Health Qual Life Outcomes 2010;8:57. doi: 10.1186/1477-7525-8-57 [Crossref]
- Varoli FK, Pedrazzi V. Adapted version of the McGill Pain Questionnaire to Brazilian Portuguese. Braz Dent J. 2006;17(4):328-35. doi: 10.1590/S0103-64402006000400012 [Crossref]
- Fairbank JCT, Pynsent PB. The Oswestry Disability Index. Spine. 2000;25(22):2940-2953. doi: 10.1097/00007632-200011150-00017 [Crossref]
- Ciconelli RM. Tradução para o português e
validação do Questionário Genérico de Qualidade de Vida "Medical outcomes study 36 - item short-form health survey
(SF-36)". [Dissertação]. São Paulo: Universidade Federal de São Paulo
(Escola Paulista de Medicina); 1997.
- Richardson CH, Hides P. Therapeutic exercise for
lumbopelvic stabilization. A motor control approach for the treatment and
prevention of low back pain. 2ª ed. Churchill Livingstone; 2004.
- Hodges PW, Richardson CA. Inefficient muscular stabilization of the lumbar spine associated with low back pain: a motor control evaluation of transversus abdominis. Spine. 1996;21(22):2640-50. doi: 10.1097/00007632-199611150-00014 [Crossref]
- Meucci RD, Fassa AG, Faria NM. Prevalence of chronic low back pain: systematic review. Rev Saude Publica. 2015;49:1. doi: 10.1590/S0034-8910.2015049005874 [Crossref]
- Shiri R, Karppinen J, Leino-Arjas P, Solovieva S, Viikari-Juntura E. The association between obesity and low back pain: a meta-analysis. American Journal of Epidemiology. 2009;171(2):135–54. doi: 10.1093/aje/kwp356 [Crossref]
- Heuch I, Hagen K, Heuch I, Nygaard Ø, Zwart JA. The Impact of Body Mass Index on the Prevalence of Low Back Pain. Spine. 2010;35(7):764–8. doi: 10.1097/BRS.0b013e3181ba1531 [Crossref]
- Fine N, Lively S, Séguin CA. Intervertebral disc degeneration and osteoarthritis: a common molecular disease spectrum. Nat Rev Rheumatol 19, 136–152 (2023). doi: 10.1038/s41584-022-00888-z [Crossref]
- Byrnes K, Wu PJ, Whillier S.
Is Pilates an effective rehabilitation tool? A systematic review. J Bodyw Mov Ther [Internet].
2018;22(1):192–202. Available from:
https://www.ncbi.nlm.nih.gov/pubmed/29332746
- Pilates JH, Miller WJ. Return to life
through contrology. Ravenio Books; 1945.
- Alves MC, Souza Neto RJ, Barbosa RI, Marcolino AM, Kuriki HU. Effects of a Pilates protocol in individuals with non-specific low back pain compared with healthy individuals: Clinical and electromyographic analysis. Clinical Biomechanics. 2020;72:172–8. doi: 10.1016/j.clinbiomech.2019.12.009 [Crossref]
- Ceccato J, Varriale M, Donadio MVF, Kiefer
T, Vaz MA. Avaliação
Funcional do Transverso do Abdômen em Remadores. Rev Bras Biomec. 2011;12:9-13.
- Yamato
TP, Maher CG, Saragiotto
BT, Hancock MJ, Ostelo RWJG, Cabral CMN, et al. Pilates
for low back pain. Sao Paulo Medical Journal. 2016;134(4):366–7. doi: 10.1590/1516-3180.20161344T1 [Crossref]
- Kamioka H, Tsutani K,
Katsumata Y, Yoshizaki T, Okuizumi H, Okada S, et al. Effectiveness
of Pilates exercise: A quality evaluation and summary of systematic reviews
based on randomized controlled trials. Complementary Therapies in Medicine
[Internet]. 2016 Apr;25:1–19. Available from:
https://www.sciencedirect.com/science/article/pii/S096522991530039X
- Grooten WJA, Boström C, Dedering Å, et al. Summarizing the effects of different exercise types in chronic low back pain - a systematic review of systematic reviews. BMC Musculoskelet Disord. 2022;23(1):801. doi: 10.1186/s12891-022-05722-x [Crossref]
