Rev Bras Fisiol Exerc
2019;18(3):136-44
https://doi.org/10.33233/rbfe.v18i3.3239
ORIGINAL ARTICLE
How does blood flow restriction training have been applied
in Brazil?
Como
o treinamento com oclusão vascular tem sido utilizado no Brasil?
Cauê
Vazquez La Scala Teixeira*, Caio Bastos Messias*, Leonardo
Farah**, Ezequias Pereira Neto***, Alexandre Lopes Evangelista***, Danilo Sales
Bocalini****, Marzo Edir Da
Silva-Grigoletto***
*Universidade
Federal de São Paulo, Santos, SP, **Universidade Tecnológica Federal do Paraná
(UTFPR), Curitiba, PR, ***Universidade Federal de Sergipe, Aracaju, SE, ****Universidade
Federal do Espírito Santo, UFES, Vitória, ES
Received: September
24, 2019; Approved: September
30, 2019.
Corresponding author: Cauê
Vazquez La Scala Teixeira, Pça. Engº.
José Rebouças, S/N, Ponta da Praia 11030-000 Santos SP
Cauê
Vazquez La Scala Teixeira: contato@caueteixeira.com.br
Caio
Bastos Messias: caiosbm@hotmail.com
Leonardo
Farah: leonardo@cardiomed.com.br
Ezequias
Pereira Neto: neto.pereiraedf@gmail.com
Alexandre
Lopes Evangelista: contato@alexandrelevangelista.com.br
Danilo
Sales Bocalini: bocaliniht@hotmail.com
Marzo Edir da Silva-Grigoletto: medg@ufs.br
Abstract
Objective: The aim of the
present study was to analyze
how the blood
flow restriction (BFR) training
has been used by professionals
in Brazil, focusing on the user's
profile, control of training
variables and the rate of occurrence
of adverse effects. Methods: Eighty-six health professionals with experience in BFR training were interviewed through a digital questionnaire prepared by the authors
containing 17 questions about the characteristics
of using the method. Results: BFR training has been used
in Brazil for the past 5 years, mainly
by Physical Education professionals who attend healthy
adults, athletes and elderly people
with several objectives. Most of the professionals
seem to follow specific scientific recommendations for the BFR training
prescription, except for a small portion of
participants, especially regarding pressure control to BFR. Low-severity immediate adverse effects associated with the method
were observed at reasonable rates and no serious effects were reported.
Conclusion:
Since a small number of professionals
reported inattention to scientific recommendations
for controlling this variable, these adverse effects may be
associated with inadequate control of vascular occlusion pressure.
Keywords: hypoxia, physical training, rehabilitation, therapeutic occlusion, vascular occlusion devices.
Resumo
Objetivo: O objetivo
do presente estudo foi analisar como o treinamento de restrição de fluxo sanguíneo
(RFS) tem sido utilizado por profissionais no Brasil, com foco no perfil do usuário,
controle de variáveis de treinamento e taxa de ocorrência de efeitos adversos. Métodos: Oitenta e seis profissionais de
saúde com experiência em treinamento de RFS foram entrevistados por meio de um questionário
digital elaborado pelos autores, contendo 17 perguntas sobre as características
do uso do método. Resultados: O treinamento
em RFS tem sido utilizado no Brasil nos últimos 5 anos, principalmente por profissionais
de Educação Física que atendem principalmente adultos, atletas e idosos saudáveis,
com diversos objetivos. A maioria dos profissionais parece seguir recomendações
científicas específicas para a prescrição do treinamento de RFS, com exceção de
uma pequena parcela dos participantes, principalmente no que se refere ao controle
da pressão no RFS. Efeitos adversos imediatos de baixa gravidade associados ao método
foram observados a taxas razoáveis e nenhum efeito sério foi relatado. Conclusão: Como um pequeno número de profissionais
relatou desatenção às recomendações científicas para o controle dessa variável,
esses efeitos adversos podem estar associados ao controle inadequado da pressão
de oclusão vascular.
Palavras-chave:
hipóxia, treinamento físico, reabilitação, oclusão terapêutica, dispositivos de
oclusão vascular.
Introduction
The blood flow restriction (BFR) training is a technique created by the
Japanese researcher Yoshiaki
Sato in the late 1960s, which
consists of performing physical exercises under the condition of
restricted blood flow to the
mobilized segment (arms or legs)
and has the
primary aim of maximizing adaptations
related to strength and hypertrophy
under conditions where the application
of high intensities is not possible
or desirable [1]. It has become popular worldwide in the last decade. The main justification for this fact is
based on the large number
of scientific publications demonstrating the benefits of
this technique for heterogeneous populations, especially on muscle
strength and mass [2-4], besides relative safety [5-7].
Studies have shown that
the isolated use of partial BFR can attenuate the
loss of strength
and muscle mass in immobilization situations [8]. If associated with aerobic exercise, such as walking and cycling, it can promote increased
muscle strength and hypertrophy and these increases
are more significant when associated with strength training using low external loads
[9]. Thus, the method has become
a training alternative for both
musculoskeletal rehabilitation
and performance. In addition,
while there is much speculation
about possible risks associated with BFR, several studies show that if the specific
recommendations for its application
are observed, the risks are low.
Following this worldwide trend of popularization
of BFR training, in Brazil the technique has
become better known and interest
in its use has grown in the last decade,
especially associated with physical training. Much of this
fact is due
to the greater
availability of information on the topic in Portuguese,
such as scientific articles [10,11], books [12,13], lectures
and classes.
However, although popularity is increasing and
the body of technical and
scientific information is large, little
is known about how BFR training is used in Brazil.
Thus, considering the need to
know the characteristics of its use to confront the
specific scientific evidence, the aim
of this study
was to analyze
how the BFR training has been used
by professionals in Brazil, focusing on the user's
profile, control of training
variables and the rate of occurrence
of adverse effects.
Methods
Participants
Ninety-five health professionals with experience in BFR training operating in different regions of Brazil
participated in the study, of these,
9 were excluded from the analysis
because they did not completely
answer the questionnaire. All participants were invited through digital means (e-mail and social medias) and the participation
in the study was voluntary, by digital signature of informed consent
term. The project complied with all ethical
criteria contained in the Declaration of Helsinki and was approved by
the Research Ethics Committee of Nove de Julho University (#1.861.919
of Dec 12, 2016).
Instruments and procedures
In order to accomplish the aim of the research and considering that we did not find previous studies with similar research model on BFR training, a digital questionnaire was elaborated through the Google Forms platform, containing 17 closed questions about to the professional's profile (3 questions) and the form to use the BFR training (14 questions). After disclosure of the link through invitations sent by digital means such as emails and social medias of health professionals from all over Brazil, the questionnaire was available for completion for a period of 15 days. After this period, the data were tabulated and the completed questionnaires were considered for analysis.
Statistical analysis
The results are presented considering the respective absolute and relative
(percentage) distributions for
each question applied. For analysis, we used Microsoft Excel and SPSS v.20software.
Results
Of the 86 volunteers who participated in the study (11 women,
75 men, 30.8 ± 7.6 years), 81
(94.2%) were academics or professionals of Physical Education,
2 (2.3%) of Physical Therapy and 3 (3.5%) from other health
areas. Regarding the use of the
method, the vast majority of
professionals (89.5%) reported
knowing or using it for less than 5 years and
the main purpose reported for use was musculoskeletal rehabilitation (57.0%), with balanced distribution for other purposes. Healthy adults comprise the public
most frequently assisted with BFR training (Table I).
Table I - Absolute (N) and relative (%)
distribution related to time and purpose
of use, as well as the profile of the public assisted
with BFR training
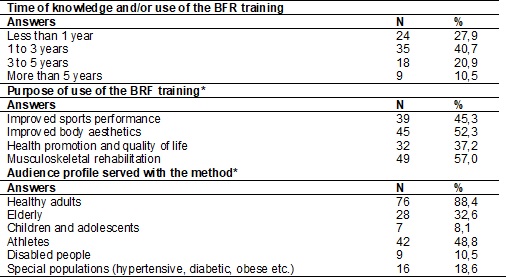
*questions in which more than one answer
was allowed, so the sum of
the relative distribution is greater than 100%
Regarding the control of
training variables, in most
cases, the method is applied preferentially
to resistance exercises, in a single exercise per
session, with low weekly frequency
(1 to 2 times), respecting a
maximum use time of 10 minutes
per session. Most professionals also reported using a low intensity protocol
from 2 to 4 sets performed until voluntary fatigue with short intervals between sets (less than 30 seconds).
When the method is
applied to more than one exercise,
most professionals reported adopting a time less than 3 minutes between exercises. To generate blood
flow restriction, specific inflatable cuffs and elastic
tourniquets were adopted. Regarding occlusion pressure for training, most reported the
use of a certain percentage of total occlusion pressure and systolic blood
pressure (Table II).
Table II - Absolute (N) and relative (%)
distribution related to control of
variables in BFR training
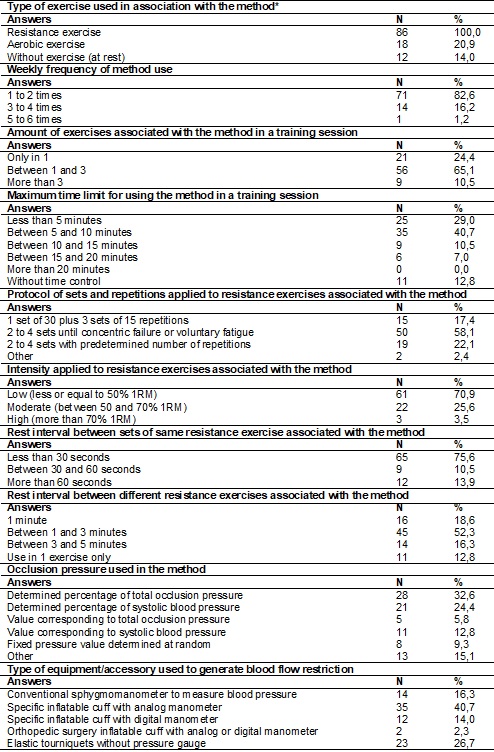
*questions in which more than one answer
was allowed, so the sum of
the relative distribution is greater than 100%
Regarding the observation of adverse effects resulting from the method, most
professionals reported never having observed
problems, but paresthesia and red pigmentation in the limb under
BFR were reported by 1/3 of the
volunteers, while severe acute pain
by 1/4 of the professionals (Table III).
Table III - Absolute (N) and relative (%)
distribution related to observation of adverse effects observed in BFR training
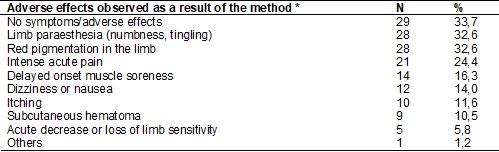
*questions in which more than one answer
was allowed, so the sum of
the relative distribution is greater than 100%
Discussion
Considering the increasing popularity of BFR training in Brazil and the
lack of information
on how the
method has been used by
professionals working in this country, this paper sought to
understand how this type of
training has been used by professionals
in Brazil, focusing on user's profile, control of training variables and the
rate of adverse effects occurrence. The main finding of the
present study was that most
of the interviewed
professionals seem to adopt practices
consistent with the current recommendations
for prescribing, supervising
and controlling the variables involved
in BFR training, revealing attention
to scientific evidence. Additionally, the occurrence of high severity adverse effects has not
been reported.
The vast majority of professionals
who participated in this research and
reported the use of the method
were from the Physical Education
area, which was to be
expected since many studies involving
BFR training observed significant
increases in strength and muscle mass
[2,3]. These are results that achieve the
aims of majority
of the public
seeking the services of the
Physical Education professional
for aesthetic purposes, health promotion or improvement of physical performance, confirmed in the purposes reported by the volunteers.
However, what attracted attention was the
small participation of professionals from physical therapy
and other health areas, which
indicates a probable underutilization of the method in these
areas, since the current scientific
literature has supported the use of this technique
for therapeutic purposes [14,15].
Importantly, despite the small participation
of physiotherapists and health professionals
from other areas in this research,
musculoskeletal rehabilitation
was the most
reported purpose given the use of
BFR training, highlighting the
significant performance of Physical Education professionals in this area, following trend pointed by
Thompson [16].
Although international scientific literature has been exploring the BFR training for over a decade,
especially after the first publication
by Kaatsu Training creator Yoshiaki Sato [1], most professionals interviewed have known the
method for less than 5 years. However,
this data is justified by the
recent availability of information on BFR training in Portuguese.
Regarding the public to
which the technique has been
applied, a higher utilization rate was observed in healthy adults and athletes,
publics for whom the scientific literature presents great availability of information to support its safe use [9,17,18].
In special populations, such as the elderly,
children, adolescents, people with disabilities
and people with certain diseases,
the rates of BFR training application were lower revealing caution among the
professionals, because, although emerging, there is still a small amount of
scientific publications involving this population [4,19,20].
About training
variables, resistance exercises were the most used,
corroborating the literature that shows the effects of
this type of exercise associated
with BFR on strength and hypertrophy
may be more expressive than aerobic exercises and BFR without exercise [9]. Most professionals use up to 3 resistance exercises associated with BFR per training session, in
accordance with Pope et al. [17].
Although the literature does not present a limit
amount of exercises that can be associated
with blood flow restriction in a training session, Nakajima et al.
[21] recommend a maximum time
limit for using the technique in a single session, which would be 15 and
20 minutes per sessions involving
upper and lower limbs, respectively.
In this sense, with the exception
of 12% of respondents who do not control the
use time, the others do not exceed 15 minutes, revealing attention to the recommendations
in the literature.
Regarding the external loads
used in resistance exercises associated with BFR, although ~70% of the professionals
reported using low external loads
(<50% 1RM), ~1/3 of the sample
reported the use of high intensities (>50% 1RM),
a fact that caught our attention,
as some studies show that use
of high external loads in the method
does not provide additional benefits [10,22]. Corroborating the idea, studies have
shown that one of the
main advantages of strength training associated with BFR over traditional training models is that it does not need to
use heavy loads and may be a viable
alternative for conditions in
which high loads are not possible and/or desirable [2,9].
The most commonly used sets and repetitions protocols include performing 2 to 4 sets per exercise, performing repetitions to concentric failure
(~58%) or with a predetermined number of repetitions (~22%). Although some researches use similar
protocols [23,24], the literature reports as the most common performing 1 set of 30 repetitions, followed by 3 sets of 15 repetitions [25]. In the present study, a minority reported the use of this
protocol, a fact that also draws
our attention because it is considered
a standard protocol, as it has
been widely investigated [26].
Most participants (~86%) reported adopting short rest intervals between sets (≥ 60
seconds), in accordance with specific scientific
recommendations [9]. However,
when the method is applied
to more than one exercise in the training session, 71% of respondents said to apply
rest intervals of less than
3 minutes between exercises,
a shorter time than suggested by Pope et al. [17] to allow reperfusion,
which is 5 minutes without BFR. Almost all participants (~99%) reported applying the method with
weekly frequency less than or
equal to 4 times, also in accordance with what has
been recommended [9].
To generate BFR, about 73% of professionals use some type of inflatable
cuff with objective pressure control (manometer), however, the use of elastic tourniquets
with no objective pressure control was expressive (~27%). Although previous studies have shown
the use of elastics tourniquets may be a practical
and cost-effective [27] and safe [28] alternative, the number of
publications is limited [29]. Moreover, when using elastic
tourniquets, pressure control becomes subjective [28] and it depends on the
user's sensitivity which increases the risk of
intervention failure, as noted by Loenneke
et al. [30].
Regarding occlusion pressure, although many professionals
use values related to total occlusion pressure or systolic
blood pressure, which meets the
scientific safety recommendations [9,17,25], the use
of total or randomly determined-occlusion pressure values have been reported
(~6 and ~9%, respectively),
which may substantially increase the risk of
adverse effects.
About the occurrence of adverse effects resulting from the method, according
to the best
of our knowledge,
this is the
first study that analyzed the
observation rate among professionals working in Brazil. One third
of the sample reported never having observed any adverse effects; in contrast the observation
of paresthesia and red pigmentation
in the limb was also reported
by approximately 1/3 of respondents.
In the present study, although the occurrence
rates were higher than those reported
by Nakajima et al.
[31], in research conducted
in Japan, reported effects are immediate and appear to
be alleviated or disappear after
the end of
the training session. However, these effects may decrease
training adherence and this hypothesis needs to be
further investigated. It is important to
highlight that, even observing that most of
the professionals follow scientific recommendations for the prescription of BFR training, part of the interviewees
does not seem to pay attention
to these details, especially regarding the pressure
control during the training session. This may partly
explain the adverse effect rates observed in the present study.
The main limitation of this
study is related to the
limited number of professionals interviewed considering the geographic and population dimensions of Brazil.
Thus, it is necessary to enlarge
the sample to confirm the results
found here.
Conclusion
BFR training has been used in Brazil
for the past 5 years, mainly by
Physical Education professionals who mainly attend healthy
adults, athletes and elderly people
with several objectives. Regarding the manipulation of training variables, most of the
reports seem to follow specific scientific recommendations for the BFR training prescription, except for a small portion that did
not seem to pay attention
to these recommendations, especially regarding pressure control to BFR, which may increase
the risk of adverse effects.
Low-severity immediate adverse effects associated with the method were
observed at reasonable rates and no serious effects were reported. However, these effects may be
associated with inadequate control of vascular occlusion pressure, since a small number of
professionals reported inattention to scientific recommendations for controlling this variable.
References
- Sato
Y. The history and future of Kaatsu training. Int J Kaatsu Training Res 2006;1(1):1-5.
https://doi.org/10.3806/ijktr.1.1
- Slysz J, Stultz
J, Burr JF. The efficacy of blood flow
restricted exercise: A systematic review & meta-analysis.
J Sci Med Sport 2016;19(8):669-75.
https://doi.org/10.1016/j.jsams.2015.09.005
- Lixandrão ME, Ugrinowitsch C, Berton R, Vechin FC, Conceição MS, Damas F et al. Magnitude of muscle strength
and mass adaptations between high-load resistance training versus low-load resistance training associated with blood-flow restriction: a systematic review and meta-analysis. Sports Med 2018;48(2):361-78.
https://doi.org/10.1007/s40279-017-0795-y
- Centner C, Wiegel
P, Gollhofer A, König D. Effects of blood
flow restriction training on muscular strength and hypertrophy in older individuals: A systematic review and meta-analysis. Sports Med 2019;49(1):95-108.
https://doi.org/10.1007/s40279-018-0994-1
- Nakajima
T, Kurano M, Iida H, Takano
H, Oonuma H, Morita T et al. Use and
safety of KAATSU training: results of a national
survey. Int J KAATSU Training
Res 2006;2: 5-14. https://doi.org/10.3806/ijktr.2.5
- Loenneke JP, Wilson JM, Wilson GJ,
Pujol TJ, Bemben MG. Potential safety issues with blood
flow restriction training. Scand J Med Sci
Sports 2011;21:510-8. https://doi.org/10.1111/j.1600-0838.2010.01290.x
- Neto
GR, Novaes JS, Dias I, Brown A, Vianna J, Cirilo-Sousa MS. Effects
of resistance training with blood flow
restriction on haemodynamics: a systematic review.
Clin Physiol Funct Imaging 2017;37(6):567-74. https://doi.org/10.1111/cpf.12368
- Takarada Y, Takazawa
H, Ishii N. Applications of vascular occlusion diminish disuse atrophy of knee
extensor muscles. Med Sci Sports Exerc 2000;32(12):2035-9.
https://doi.org/10.1097/00005768-200012000-00011
- Kubota A, Sakuraba
K, Sawaki K, Sumide T, Tamura Y. Prevention of disuse muscular weakness by restriction
of blood flow. Med Sci
Sports Exerc 2008;40(3):529-34. https://doi.org/10.1249/MSS.0b013e31815ddac6
- Scott
BR, Loenneke JP, Slattery KM,
Dascombe BJ. Exercise with blood flow
restriction: an updated evidence-based approach for
enhanced muscular development.
Sports Med 2015;45:313-25. https://doi.org/10.1007/s40279-014-0288-1
- Chulvi-Medrano IC, Hernández
SB, Pérez MR, La Scala Teixeira CV. O edema muscular induzido pelo treinamento com
oclusão vascular parcial é dependente da intensidade? Um estudo piloto. Rev Bras Prescr
Fisiol Ex 2015;9(53):309-14.
- Corrêa
DA, Rizatto GF, Marchetti PH, Lopes CR. Breve revisão
dos efeitos do treinamento de força com restrição vascular nas adaptações musculares
de força e hipertrofia. Rev CPAQV 2016;8(2):1-9.
- La
Scala Teixeira CV. Treinamento de força com oclusão vascular. São Paulo: Lura, 2018.
- Nascimento
DC. Exercício físico com oclusão vascular:
métodos para a prescrição segura na prática
clínica. São Paulo: Blucher; 2018.
- Hughes
L, Paton B, Rosenblatt B, Gissane C, Patterson SD. Blood flow restriction training in clinical musculoskeletal rehabilitation: a systematic review
and meta-analysis. Br J Sports Med 2017;51(13):1003-11.
https://doi.org/10.1136/bjsports-2016-097071
- Barber-Westin S, Noyes FR. Blood flow-restricted training for lower
extremity muscle weakness due to
knee pathology: A systematic review. Sports Health 2019;11(1):69-83. https://doi.org/10.1177/1941738118811337
- Thompson
WR. Worldwide survey of fitness trends for 2019. ACSM's Health Fit J 2018;22(6):10-7. https://doi.org/10.1249/FIT.0000000000000438
- Pope
ZK, Willardson JM, Schoenfeld
BJ. Exercise and blood flow restriction.
J Strength Cond Res 2013;27:2914-26. https://doi.org/10.1519/JSC.0b013e3182874721
- Scott
BR, Loenneke JP, Slattery KM,
Dascombe BJ. Blood flow restricted exercise for athletes: A review of available evidence.
J Sci Med Sport 2016;19(5):360-7.
https://doi.org/10.1016/j.jsams.2015.04.014
- Domingos
E, Polito MD. Blood pressure response between resistance exercise with and without
blood flow restriction: A systematic review and meta-analysis. Life Sci 2018;209:122-31. https://doi.org/10.1016/j.lfs.2018.08.006
- Cardoso
RK, Araujo AM, Freitas MP, Rombaldi
AJ. Efeito do treinamento com restrição parcial do fluxo sanguíneo em adultos mais
velhos e idosos: Uma revisão sistemática. Rev Bras Cineantropom Desempenho Hum 2018;20(2):219-28.
https://doi.org/10.5007/1980-0037.2018v20n2p219
- Nakajima
T, Morita T, Sato Y. Key considerations when conducting Kaatsu training. Int J Kaatsu Training Res 2011;7:1-6. https://doi.org/10.3806/ijktr.7.1
- Laurentino
G, Ugrinowitsch C, Aihara AY,
Fernandes AR, Parcell AC, Ricard
M et al. Effects of strength training and vascular occlusion. Int J Sports Med 2008;29(8):664–7. https://doi.org/10.1055/s-2007-989405
- Laurentino
GC, Ugrinowitsch C, Roschel
H, Aoki MS, Soares AG, Neves M Jr et al. Strength training with blood flow restriction
diminishes myostatin gene expression.
Med Sci Sports Exerc 2012;44(3):406-12. https://doi.org/10.1249/MSS.0b013e318233b4bc
- Meister CB, Kutianski FAT, Carstens LC, Andrade
SLF, Rodacki ALF, Souza RM. Effects
of two programs
of metabolic resistance training on strength and hypertrophy.
Fisioter Mov 2016;29(1):147-155.
https://doi.org/10.1590/0103-5150.029.001.AO16
- Patterson
SD, Hughes L, Warmington S, Burr
J, Scott BR, Owens J, et al. Blood flow restriction exercise position stand: considerations
of methodology, application, and safety. Front Physiol 2019;10:533. https://doi.org/10.3389/fphys.2019.00533
- Conceição
MS, Ugrinowitsch C. Exercise
with blood flow restriction: an effective alternative
for the non-pharmaceutical treatment for muscle wasting. J Cachexia Sarcopenia Muscle 2019;10(2):257-62. https://doi.org/10.1002/jcsm.12397
- Lowery RP, Joy JM, Loenneke JP, Souza EO, Machado
M, Dudeck JE, Wilson JM. Practical
blood flow restriction training increases muscle hypertrophy during a periodized resistance training programme. Clin Physiol Funct
Imaging 2014;34(4):317-21. https://doi.org/10.1111/cpf.12099
- Wilson
JM, Lowery RP, Joy JM, Loenneke JP, Naimo MA. Practical blood flow restriction training increases acute determinants of hypertrophy without increasing indices of muscle damage.
J Strength Cond Res 2013;27(11):3068-75.
https://doi.org/10.1519/JSC.0b013e31828a1ffa
- Mattocks KT, Jessee MB, Mouser JG, Dankel SJ, Buckner SL, Bell ZW et
al. The application of blood flow restriction:
lessons from the laboratory. Curr Sports Med Rep 2018;17(4):129-34.
https://doi.org/10.1249/JSR.0000000000000473
- Loenneke JP, Kearney ML, Thrower AD, Collins S,
Pujol TJ. The acute response
of practical occlusion in the knee extensors. J StrengthCond Res 2010;24(10):2831-4. https://doi.org/10.1519/JSC.0b013e3181f0ac3a
- Nakajima T, Kurano M, Iida H, Takano H, Oonuma H, Morita T, et al. Kaatsu Training Group. Use and safety of kaatsu training: Results of a national survey. Int J Kaatsu Training Res 2006;2:5-13. https://doi.org/10.3806/ijktr.2.5