Rev Bras Fisiol Exerc;19(2):104-113
ORIGINAL
ARTICLE
Analysis of balance control in elderly practitioners of modalities of yoga,
gymnastics and stretching of the Exercise Orientation Service in Vitória/ES
Análise dos sistemas de
controle do equilíbrio em idosos praticantes das modalidades ioga, ginástica e
alongamento do Serviço de Orientação do Exercício de Vitória/ES
Jean Leite Cruz1,
Milena Razuk1, Victor Anthony Mendes Ferreira1, Leonardo Araujo Vieira1, Natalia Madalena Rinaldi1
1Laboratório de Análise Biomecânica do Movimento Humano, Centro de Educação Física e Esportes, Universidade Federal de Espírito Santo, Vitória, ES, Brazil
Received
on: December 19, 2019; accepted on: February 19, 2020.
Corresponding
author: Natalia Madalena Rinaldi,
Physical Education and Sports Center, Federal University of Espírito
Santo, 514 Fernando Ferrari Avenue, 29075-910 Vitória ES, Brazil
Jean Leite Cruz:
jeanleitevni@hotmail.com
Milena Razuk: milena.razuk@gmail.com
Victor Anthony Mendes
Ferreira: vitorf.ufes@gmail.com
Leonardo Araujo Vieira: lcaramuru@gmail.com
Natalia Madalena
Rinaldi: natalia.rinaldi@ufes.br
Abstract
Different
motor interventions have been widely investigated in balance control in
elderly. However, it is not yet clear which type of motor intervention promotes
improvements in balance control systems in the elderly. The aim of this study
was to compare different motor interventions of the balance control system in
elderly. Fifty-six elderly people participated in the study, distributed in
sedentary group (SED), gymnastic group (GG), yoga group (GI) and stretching
group (GA). Participants were evaluated using the Balance Evaluation System
Test (BESTest) tool, designed to evaluate six items
of balance control systems. The variables analyzed in the study were the scores
obtained in each of the BESTest items. The results
showed that GG and GI presented higher values in BESTest
compared to the SED group. Even more, for the item gait stability and stability
limits presented higher values compared to the other BESTest
items. The conclusion of the study is that elderly gymnastics and yoga
practitioners, modalities offered by the Exercise Orientation Service (SOE) can
promote benefits to the balance control system in elderly.
Keywords: BESTest; balance; elderly; motor
intervention.
Resumo
Diferentes intervenções
motoras têm sido amplamente investigadas no controle do equilíbrio em idosos.
Entretanto, ainda não está elucidado qual o tipo de intervenção motora que
promove melhoras nos sistemas de controle do equilíbrio em idosos. O objetivo
do estudo foi comparar diferentes intervenções motoras do sistema de controle
do equilíbrio em idosos. Participaram do estudo 56 idosos, distribuídos em
grupo sedentário (SED), grupo ginástica (GG), grupo ioga (GI) e grupo
alongamento (GA). Os participantes foram avaliados através da ferramenta Balance
Evaluation System Test (BESTest),
desenvolvida para avaliar seis itens do sistema de controle do equilíbrio. As
variáveis analisadas no estudo foram as pontuações obtidas em cada um dos itens
do BESTest. Os resultados mostraram que o GG e GI
apresentaram valores maiores no BESTest comparado ao
grupo SED. Ainda, para os itens estabilidade da marcha e limites de
estabilidade apresentaram valores maiores comparados aos demais itens do BESTest. A conclusão do estudo é que idosos praticantes de
ginástica e de ioga, modalidades oferecidas pelo Serviço de Orientação ao
Exercício (SOE) tem capacidade de promover benefícios ao sistema de controle do
equilíbrio em idosos.
Palavras-chave: BESTest;
equilíbrio; idosos; intervenção motora.
Introduction
The postural stability control and functional mobility are fundamental
for carrying out daily activities. During the aging process, changes in these
two aspects can be observed, which can have consequences for movement control,
for instance, history of falls [1]. Thus, changes in the sensory systems are
related to an erroneous perception about the body positioning in space [3].
Based on these data, it is important to develop motor interventions to improve
the control of dynamic static and balance in the elderly in order to reduce the
risk of falls in this population. Regarding the static balance control, Li et
al. [4] found improvement in the functional reach tests, Berg balance scale and
Timed Up & Go (TUG) in seniors after a period of 26 consecutive weeks of
Tai Chi training. However, Lelard et al. [5]
evaluated static balance control through the pressure center with eyes open and
closed, and speed gait over a 10-meter course. The authors compared a Tai Chi
program with a balance training program for three months at a twice a week frequency, and concluded that the intervention period was
insufficient to verify variations in gait speed or postural levels in the eyes
open and eyes closed condition on both interventions.
Zettergen
et al. [6] found an increase in gait speed and an increase in the Berg
scale score in the elderly after an 8-week yoga intervention. Still, Oken et al. [7] investigated the effect of yoga
training on balance control in the elderly. After the three-month period, these
authors found that the elderly were able to remain in unipodal
support for a longer time. A study by Zhuang et al. [8] verified the effect of
generalized training (balance and flexibility) on walking time (TUG) and
functional reach test. After the motor intervention period, the elderly reduced
walking time and increased the distance in the functional reach test.
Thus, the results showed beneficial effects of individualized and
generalized training, however, it is not yet fully elucidated which is the best
type of motor modality (generalized, stretching or yoga) for the control of
static and dynamic balance in the elderly. In addition, it would be interesting
that these interventions were easily accessible to the population, making it
possible to discriminate the benefits of physical activity. In this regard, the
SOE (Exercise Orientation Service) is a pioneering service considered a model by
the Brazilian Society of Sports Medicine in the area of Physical Activity and
Health developed in Vitória city/ES. In this program, physical activities are
developed in groups with the objective of improving the quality of life and
preventing chronic diseases. There are several modules throughout the city,
with trained teachers to serve the population. Gymnastics, yoga and stretching ara activities usually offered in SOE modules
Regarding the analysis of balance and the elderly, some studies used
BERG, TUG, POMA scales, among other existing tests, to evaluate balance [9-12].
Pimentel and Scheicher [9], for example, compared the
risk of falls among sedentary and active elderly people, verifying how the
practice of physical exercise can reflect on the subjects' performance on the
Berg scale. The authors found a worse performance in the inactive group, it
suggests that regular exercise can interfere with this performance and that
active subjects have less chance of falling.
Souza et al. [10] used the Berg scale to assess the balance of
elderly women after performing different exercise protocols. The participants
were divided into two groups: group A who performed resistance exercises, and
group B, who performed proprioceptive exercises. The authors found that both
groups showed improvement in balance after intervention, showing that the two
protocols generated a significant difference in balance, but when compared, no
difference was found between the groups. Thus, it was not possible to determine
whether there is a specific type of exercise to improve body balance.
Pavanate
et al. [11] verified the balance ratio of elderly women who practice
physical activity considering different ages using the Timed Up and Go (TUG).
The authors conclude that younger the age better the balance, which further
demonstrates the loss of the ability to maintain balance with aging. Carvalho,
Pinto and Mota [12] analyzed a relation between fear
of falling, balance and physical activity. The Balance assessment was performed
using the Performance-Oriented Mobility Assessment (POMA). The authors
concluded that the practice of physical activity is associated with better
balance performance and less fear of falling. From these theoretical
assumptions, it can be concluded that motor intervention promotes benefits for
the control of balance in the elderly, however, some questions regarding motor
interventions and the types of assessment adopted in these studies need to be
better clarified.
In the studies previously presented, the authors used some scales that
did not specifically assess the systems involved in balance control. Thus, Horak et al. [13] developed a clinical tool called BESTest (Balance Assessment System Test), whose main use
criteria are different systems involved in balance control, in order to
identify the underlying deficiencies that contribute to the prejudice of
balance. From this assessment, it is possible to identify which balance control
systems may be affected by the aging process, helping the health professional,
since it would be easier to know where to intervene. Thus, an investigation
into the benefits applied by different activities / changes, show the important
effects for those who can design and plan a quality intervention capable to
produce beneficial changes in the balance control in the elderly.
In
this context, the objective of the study was compared with different
balance control engines in elderly people who practice physical
activity by the Exercise Orientation Service (gymnastics, yoga and
monitoring) with elderly
people who do not practice physical activity, making use of an easy to
use and
low cost tool called Balance Evaluation System Test (BESTest).
The hypothesis of the study is that the elderly who performed different motor
interventions (gymnastics, yoga and stretching) have a higher score on the BESTest compared to the sedentary groups.
Methods
Participants
The population of this study was composed of elderly participants in the
Exercise Orientation Service (SOE) and the Senior Citizenship Center located in
the Jardim da Penha neighborhood, which are part of the Unified Health Service
(SUS) and the Unique System of Social Assistance (SUAS) in the Vitória city/ES.
SOE is a program to promote physical activity in operation since 1990, which
different types of group exercises are offered, such as: gymnastics, yoga,
stretching, among others.
The sample consisted of 56 elderly people divided into four groups, with
1 group of inactive elderly people comprising 14 individuals (68.92 ± 6.53
years) recruited at the Elderly Living Center (Control Group) and 3 active
elderly groups participants of activities offered by SOE: Gymnastic Group (GG)
with 14 participants (67.36 ± 6.74 years), Yoga Group (GI) with 13 participants
(65.16 ± 5.14 years) and the Stretching Group (GA) with 15 participants (73 ±
5.12 years).
The study was approved by the ethics committee research of the Federal
University of Espírito Santo, CAAE
563154167.0000.5542. All study participants signed a Free and Informed Consent
Form (ICF) according to the rules established in Resolution No. 466/12 of the
National Health Council. As an inclusion criterion, all participants should be aged
60 to 80 years old and have independent gait without the use of auxiliary
devices, absence of cognitive, neurological and musculoskeletal diseases that
would prevent them from performing motor tasks. Also, for the groups of active
elderly people, only elderly people who had exercised for at least 3 months
with a weekly frequency of 2 workouts per week lasting approximately 60 minutes
per session were included, while in the group of inactive elderly people, only
elderly people who had not practiced physical activity for at least 3 months
were included.
Experimental
procedures
The Modified Baecke Questionnaire for the
elderly [14] was applied to assess the level of physical activity and the types
of exercises practiced by the elderly before participating in the study.
Moreover, the Mini-Mental State Examination [15] was applied to verify whether
the elderly's cognitive functions are preserved.
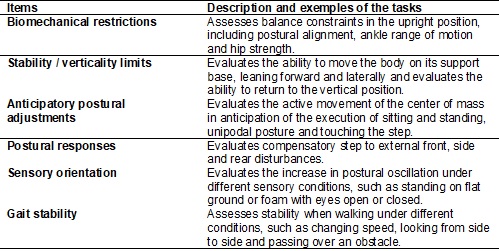
The Balance Evaluation Test (BESTest) [16] was used to assess balance control systems
[16], which consists of a clinical test that makes it possible to evaluate six
balance control systems (Table I). This test consists of 27 items, with a total
of 36 tasks divided into six sessions, referring to the balance control
systems. Each task is scored from 0 to 3 points, with 0 being the worst
possible performance and 3 the best possible, and the final score is calculated
separately for each session as a percentage [16].
Table
I - Description of the items of the Balance
Evaluation Test (BESTest)
Statistical
analysis
Statistical analyzes were performed using SPSS (Statistical Package for
the Social Sciences) software, version 21 (SPSS Inc., Chicago, United States).
To verify the normality and homogeneity of the data, the Shapiro Wilk test and
the Levene test were used, respectively. Four ANOVAs
were performed to compare anthropometric characteristics (height and body
mass), scores from Baecke and Mini-Mental assessments
between the sedentary group (SED) and the active group: gymnastics (GG), yoga
(GI) and stretching (GA). In addition, a two-way ANOVA (group [SED, GG, GI, GA]
x item BESTest [biomechanical restriction; stability
limits; anticipatory postural adjustments; postural responses; sensory
orientation; gait stability] was performed), to verify the possible effects of
exercise modalities on balance control. When necessary, post hoc tests with
Bonferroni adjustment were performed and for all analyzes a significance level
of p ? 0.05 was adopted.
Results
Table II presents the values of average and standard deviation of
anthropometric characteristics, level of physical activity through the
Modification Questionnaire for Ages and MiniMental
for the active group: stretching (GA), gymnastics (GG), yoga (GI) and sedentary
(SED). One-way ANOVA for Baecke revealed significant
difference for group (F3.52= 3.857, p <0.014). Post hoc tests revealed that
GG (5.26 ± 3.3) had a higher score compared to SED (2.39 ± 0.85). Still,
one-way ANOVA for MiniMental revealed significant
difference for group (F3.52 = 4.421, p <0.008). Post hoc tests revealed that
GG (27.14 ± 2.79) and GI (27.38 ± 2.46) had a higher score compared to SED
(23.85 ± 3.65).
Table
II - Average and standard deviation of anthropometric
characteristics, level of physical activity by the Modified Baecke
Questionnaire for the Elderly and MiniMental for the
active group: GA, GG and GI and sedentary (SED)
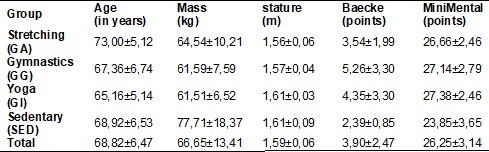
Figure 1 shows values of average and standard deviation for the items on
the BESTest scale for the active group: stretching
(GA), gymnastics (GG), yoga (GI) and sedentary (SED). Two-way ANOVA revealed a
significant difference for the group (F1.52 = 9.119; p < 0.001) and for the BESTtest item (F5.260 = (64.101, p < 0.001). Post hoc
tests for the group revealed that GG (16.53 ± 0.48 points) and GI (16.21 ± 0.49
points) showed higher values compared to SED (13.32 ± 0.48 points).
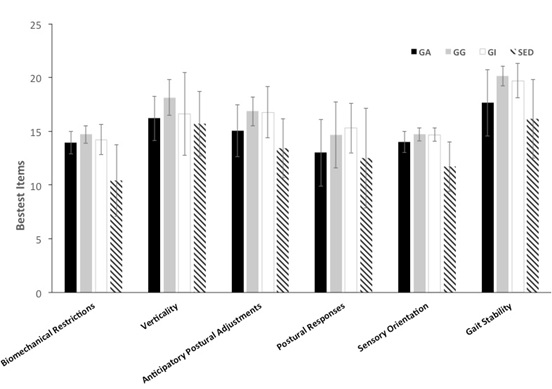
Figure
1 - Average and standard deviation of BESTest items: biomechanical restrictions, limits of
stability / verticality, anticipatory postural adjustments, postural responses,
sensory orientation, gait stability for the active group: GA, GG and GI and
sedentary (SED)
Discussion
The objective of the present study was to compare the different motor
interventions of the balance control system in elderly people who practice
physical activity by the Exercise Orientation Service (gymnastics, yoga and
stretching) with elderly people who do not practice systematic physical
activity, making use of a tool of easy application and low cost, called Balance
Evaluation System Test (BESTest).
The main findings of the present study were that the GG (16.53 ± 0.48)
and GI (16.21 ± 0.49) groups had a higher BESTest
score when compared to the sedentary group (SED) (13.32 ± 0.48). Still, the
elderly had a higher score in the items gait stability (18.37 ± 3), stability /
vertical limits (16.66 ± 2.83) and anticipatory postural adjustments (15.5 ±
2.64) compared to the items postural responses (13.82 ± 3.51), sensory
orientation (13.76 ± 1.78) and biomechanical restrictions (13.32 ± 2.53).
The modified Baecke Questionnaire for the
elderly revealed that the activity level of the GG group was higher compared to
the SED group, which was already expected. However, this was not observed in
the yoga and stretching modalities, suggesting that the intensity of both was
not capable of promoting significant levels of physical activity, remaining at
a level like the SED group. Finally, in the Mini-Mental State Exam, the elderly
in the GG and GI group had higher values than the GA and SED group. This means
that physical activity, promoted by these two modalities (gymnastics and yoga),
may be able to act on the practitioner's cognitive abilities, and can be a good
ally during the aging process.
The study by O'Hoski et al. [17] showed
a moderate relation to the rising of balance Evaluation System Test (BESTest) with physical activity in the elderly. Therefore, O'Hoski et al. [17] reinforce the results found in
the present study, because the active group practicing gymnastics and yoga
shows the best performance in BESTest when compared
to elderly people who do not practice systematic physical activity. Thus, the
result of the present study can be justified due to the fact that gymnastics
and yoga classes include exercises performed on different support bases
(bipedal and unipodal), multidirectional movements
(walking forward, backward and laterally), it can therefore contribute to the
improvement in the postural balance control system. In this context, Shanahan
et al. [18] showed that elderly practitioners of ballroom dance also performed
better in the Balance Assessment System Test (BESTest)
when compared to elderly non-dance practitioners. The authors justify that
dance, like any systematized physical activity program, contemplates several
factors that can bring benefits to the postural balance control system, such as
repetitive multidirectional movements [18].
In the present study, the active elderly participants in the motor
stretching intervention presented similar behavior at BESTest
when compared to the group that did not practice systematic physical activity. Chiacchiero et al. [19] evaluated the range of
motion for flexion, extension, abduction, adduction, internal and external
rotation of the hip; knee flexion and extension; and plantar flexion,
dorsiflexion, inversion and eversion of the ankle using a goniometer. Although
the authors report the study's limitation in evaluating the postural balance
system using only two functional tests (Timed Get Up and Go and Functional
Reach Test), no relation was found between ranges of motion of the joints
assessed with the balance test [19]. From these results, it is suggested that
motor intervention in which the main objective is only in gaining range of
motion does not promote benefits in the postural balance control system.
It is curious that all the elderly presented a worse perform in three of
the six items of the Balance Evaluation System Test (BESTtest),
with the following items: biomechanical restrictions, postural responses and
sensory guidance. Thus, it is possible to infer which are the categories with
the highest level of difficulty in the tasks evaluated, because it involves
conditions not experienced daily, especially for elderly people who have
advanced age and changes in sensory and motor systems. Makey
and Robinovitch [20] examined the relative importance
of strength (peak angular torque) and response speed (reaction time) in the
ability of individuals to use the ankle strategy to regain balance from a
determined angle of body inclination. When comparing young and elderly, the
results indicate that both strength and speed of response are lower for the
elderly. The authors suggested that the delay in response time was due to
differences in the perception of the stimulus and in the processing of the
motor commands. This can be explained due to neuronal factors such as the
reduction in the number of motor units, the decrease in the number of motor
neurons found in the spinal cord and the reduction in the capacity of the
central nervous system to send nerve impulses and activate the motor units
[21]. The decrease of strength and the increase of time to produce maximum
strength can lead to an inability to generate adequate torque in the joints
responsible for maintaining posture.
Regarding to the worst performance of the elderly in the item Sensory
Orientation of the Balance Evaluation System Test (BESTtest),
it may be due to changes in the sensory systems, mainly in the somatosensory,
visual and vestibular systems resulting from the aging process that can provide
reduced and inappropriate sensory information for the postural control system.
Several studies [22-25] have investigated the contribution of the visual system
to postural control through manipulations of this system and the verification
of the postural response triggered by this manipulation [25]. It is simple to
manipulate the visual system, since the simple act of closing your eyes is
enough to observe changes in postural control. According to a literature review
conducted by Maki and McIlroy [26], elderly people have reduced visual acuity,
contrast sensitivity, depth perception and adaptation in dark environments. In
addition, there is a decrease in the ability to detect changes in the direction
of the optical flow. As a consequence of these changes, the elderly have difficulty perceiving changes in the environment, such
as changes in the characteristics of the floor, unevenness and obstacles [27],
which can have consequences for the control of balance, such as a history of
falls. Thus, the Balance Evaluation System Test (BESTest),
by offering a complete assessment, encompassing different systems, makes it
more reliable to track and identify the system that is most affected and that
wants more attention for future interventions aimed at improving postural
balance. Thus, this tool shows great potential as an ally in assessments of the
balance control system in the elderly.
If possible, future researches should carry out a pre- and post-training
investigation of the modalities offered by SOE, in order to be clearly
evidenced possible changes caused by each of the practices and, also, observe
the necessary practice time so that the practitioners can benefit from such
changes.
An important service limiting that must be considered is the fact that
the training control is not carried out regarding the progression (overload)
and training intensity for example. In this way, a training that offers this
control can provide more accurate data about the changes and adaptations
promoted to the participants.
Conclusion
Regarding to the evaluated modalities, we can conclude that the
gymnastics and yoga modalities, offered by the Exercise Orientation Service of Vitória
City/ES, held twice a week with an approximate duration of 60 minutes per session,
has the capacity to promote positive gains in balance systems in the elderly
practitioners population, reducing the risk of falls and, consequently, helping
to improve the quality of life.
References
- Rubenstein
LZ. Falls in older people: epidemiology, risk factors and strategies for
prevention. Age Ageing 2006;3591):37-41. https://doi.org/ 10.1093/ageing/afl084
- Melzer
I, Benjuya J, Kaplanski J.
Postural stability in the elderly: a comparison between fallers and
non-fallers. Age Ageing 2004;33(6):602-7. https://doi.org/10.1093/ageing/afh218
- Pasma JH, Engelhart
D, Schouten AC, Van der Kooij H, Maier AB, Meskers CGM. Impaired standing balance: the clinical need
for closing the loop. Neuroscience 2015;267:157-65.
https://doi.org/10.1016/j.neuroscience.2014.02.030
- Li
F, Harmer P, Fisher KJ, McAuley E, Chaumeton N, Eckstrom E, Wilson NL. Tai Chi and fall reductions in older
adults: a randomized controlled trial. J Gerontol A
Biol Sci Med Sci 2005;60:187-94.
https://doi.org/10.1093/gerona/60.2.187
- Lelard T, Doutrellot
PL, David P, Ahmaidi S. Effects of a 12-week Tai Chi Chuan program versus a balance training program on postural
control and walking ability in older people. Arch Phys Med Rehabil
2010;91(1):9-14. https://doi.org/10.1016/j.apmr.2009.09.014
- Zettergren KK, Lubeski JM, Viverito JM. Effects
of a yoga program on postural control, mobility, and gait speed in
community-living older adults: a pilot study. J Geriatric Phys Ther 2011;34:88-94.
https://doi.org/10.1519/JPT.0b013e31820aab53
- Oken BS, Zajdel
D, Kishiyama S, Flegal K, Dehen C, Haas M et al. Randomized, controlled, six-month
trial of yoga in healthy seniors: effects on cognition and quality of life. Altern Ther Health Med 2006;12:40-7.
- Zhuang
J, Huang L, Wu Y, Zhang Y. The effectiveness of a combined exercise
intervention on physical fitness factors related to falls in community-dwelling
older adults. Clinical Intervention Aging 2014;9:131-40.
https://doi.org/10.2147/CIA.S56682
- Pimentel RM, Scheicher ME. Comparação do risco de queda em idosos
sedentários e ativos por meio da escala de equilíbrio de Berg. Fisioter Pesqui 2009;16(1):6-10.
https://doi.org/10.1590/S1809-29502009000100002
- Souza
CM et al. Equilíbrio
de idosas após aplicação de diferentes protocolos de exercícios. Semina: Ciências Biológicas e da Saúde
2019 ;39(2):153-60. http://doi.org/10.5433/1679-0367.2018v39n2p153
- Pavanate AA, Hauser E, Goncalves AK, Mazo GZ
et al. Avaliação do equilíbrio corporal em idosas praticantes de atividade
física segundo a idade. Rev Bras
Ciênc Esporte 2018;40(4):404-9.
https://doi.org/10.1016/j.rbce.2018.03.023
- Carvalho J, Pinto J,
Mota J. Actividade física, equilíbrio e medo de cair.
Um estudo em idosos institucionalizados. Rev Port Ciênc Desp
2007;7(2):225-31.
- Horak FB, Wrisley DM, Frank J. The Balance Evaluation
Systems Test (BESTest) to differentiate balance deficits. Phys Ther 2009;89:484-98.
https://doi.org/10.2522/ptj.20080071
- Voorrips LE, Ravelli AC, Dongelmans PC, Deurenberg P, Van Staveren WA. A physical activity
questionnaire for the elderly. Med Sci Sports Exerc 1997;29:117-21.
- Brucki SMD, Nitrini
R, Caramelli P, Bertolucci PHF, Okamoto IH.
Suggestions for utilization of the mini-mental state examination in Brazil. Arqui Neuro-Psiquiatr 2003;61(3-B):777-81.
https://doi.org/10.1590/S0004-282X2003000500014
- Maia AC,
Rodrigues-de-Paula F, Magalhães LC, Teixeira RLL. Cross-cultural
adaptation and analysis of the psychometric properties of the Balance
Evaluation Systems Test and MiniBESTest in the
elderly and individuals with Parkinson’s disease: application of the Rasch
model. Braz J Phys Ther
2013;17(3):195-217. https://doi.org/10.1590/S1413-35552012005000085
- O’Hoski S, Sibley KM, Brooks
D, Beauchamp MK. Construct validity of the BESTest,
mini-BESTest and briefBESTest
in adults aged 50 years and older. Gait & Posture 2015;42:301-5.
https://doi.org/10.1016/j.gaitpost.2015.06.006
- Shanahan
J, Coman L, Ryan F, Saunders J, O´Sullivan K, Ni Bhriain O, Clifford AM. To dance or not to dance? A
comparison of balance, physical fitness and quality of life in older Irish set
dancers and age-matched controls. Public Health 2016;56-62.
https://doi.org/10.1016/j.puhe.2016.07.015
- Chiacchiero M, Dresely
B, Silva U, Delosreyes R, Vorik B. The relationship
between range of movement, flexibility, and balance in the elderly. Topics in
Geriatric Rehabilitation 2010;26(2):147-54.
- Mackey
DC, Robinovitch SN. Mechanisms underlying age-related
differences in ability to recover balance with the ankle strategy. Gait and
Posture 2006;23:59-68.
https://doi.org/10.1016/j.gaitpost.2004.11.009
- Häkkinen K, Pastinen
UM, Karsikas R, Linnamo V.
Neuromuscular performance in voluntary bilateral and unilateral contraction and
during electrical stimulation in men at different ages. Eur
J Appl Physiol 1995;70:518-27. https://doi.org/10.1007/bf00634381
- Engelhart
DE, Pasma JH, Schouten AC. et al. Impaired
standing balance in elderly: a new engineering method helps to unravel causes
and effects. J Am Med Dir Assoc 2014;15:221-27.
https://doi.org/10.1016/j.jamda.2013.09.009
- Hay
L, Bard C, Fleury M. Availability of visual and proprioceptive afferent
messages and postural control in elderly adults. Exp Brain Res 1996;108:129-39.
- Prieto
TE, Myklebust JB, Hoffman RG et al. Measures of
postural steadiness: Differences between healthy young and elderly adults. IEEE
Trans Biomed Eng 1996;43:956-66,
1996. https://doi.org/10.1109/10.532130
- Teasdale
N, Stelmach GE, Breunig A. Postural sway
characteristics of the elderly under normal and altered visual and support
surface conditions. J
Gerontol 1991;46:238-44.
https://doi.org/10.1093/geronj/46.6.B238
- Maki
BE, McIlroy WE. Postural control in the older adult.
Clin Geriatr Med 1996;12(4):635-58.
- Lord
SR, Clark RD, Webster IW. Postural stability and associated physiological
factors in a population of aged persons. J Gerontol
1991;46(2):69-76. https://doi.org/10.1093/geronj/46.3.m69