Rev Bras Fisiol Exerc 2020;19(2):95-103
ORIGINAL
ARTICLE
Multi-components
exercise associated with dual task: Effects on physical functional performance and
mobility of the older adults
Exercício multicomponente
associado a dupla tarefa: efeitos no desempenho físico funcional e mobilidade de
idosos
1Laboratório
de Análise Biomecânica do Movimento Humano, Centro de
Educação Físia e Esportes, Universidade Federal do
Espírito Santo, Vitória, ES, Brazil
Received
on: December 13, 2019; accepted on: March 16; 2020.
Corresponding author: Janine Carvalho Valentino
Camargos, Centro de Educação Física e Desportos, Av. Fernando Ferrari, 514 Goiabeiras
29075-910 Vitória, ES, Brazil
Janine Valentino: janinevalentino@hotmail.com
Milena Razuk: milena.razuk@gmail.com
Kathisuellen Reis Assis: khathisuellem@gmail.com
Alex
Tomé: alexloucutor@gmail.com
Natalia
Madalena Rinaldi: natalia.rinaldi@ufes.br
Abstract
Objective: The aim of this study was to verify the effect of dual task in a training
protocol in the components of physical Functional Performance and mobility of older
adults. Methods: Thirty older adults (twenty-three female and seven males;
66.48 ± 3.85 years) were distributed into three randomized groups: Multi-component
physical activity group (MC), Dual Task Group (DT) and Control Group (CG). Participants
were assessed before training and after 12 weeks of training with the following
tests: Mini Mental State Examination, for evaluation of cognitive functions, AAHPERD
test battery - American Alliance for Health, Physical Education, Recreation and
Dance, for evaluation of five physical Functional Performance components, Timed
Up and Go, for evaluation of functional mobility and The Baecke
Questionnaire to assess the level of physical activity. Both MC and DT groups performed
the same multi-components training protocol, however DT group performed simultaneously
with a second cognitive task. Results: The groups that performed the training
protocol improved some aspects of physical Functional Performance and mobility compared
to the CG (p < 0.01). No difference was found between the DT and MC groups. Conclusion:
Performing two simultaneous tasks in a training protocol does not seem to influence
the functional capacity and mobility.
Keywords: dual task training; multi-components training; physical functional performance.
Resumo
Objetivo: O objetivo deste estudo
foi verificar o efeito da dupla tarefa em um protocolo de treinamento nos componentes
de Desempenho físico Funcional e mobilidade de idosos. Métodos: Trinta idosos
(vinte e três mulheres e sete homens; 66,48 ± 3,85 anos) foram distribuídos em três
grupos randomizados: grupo de atividade física multicomponente (AM), grupo de tarefas
duplas (DT) e grupo controle (GC). Os participantes foram avaliados antes do treinamento
e após 12 semanas de treinamento com os seguintes testes: Mini Exame do Estado Mental,
para avaliação das funções cognitivas, bateria de teste AAHPERD - American Alliance
for Health, Physical Education,
Recreation and Dance, para
avaliação de cinco capacidades funcionais, Timed Up and Go, para avaliação da mobilidade
funcional e o questionário de Baecke para avaliar o nível
de atividade física. Os grupos AM e DT realizaram o mesmo protocolo de treinamento
de múltiplos componentes, no entanto, o grupo DT realizou simultaneamente com uma
segunda tarefa cognitiva. Resultados: Os grupos que realizaram o protocolo
de treinamento melhoraram alguns aspectos do desempenho físico funcional e da mobilidade
em comparação ao GC (p < 0,01). Não foi encontrada diferença entre os grupos
DT e AM. Conclusão: A realização de duas tarefas simultâneas em um protocolo
de treinamento não parece influenciar a capacidade funcional e a mobilidade.
Palavras-chave: treinamento com dupla
tarefa; treinamento multi-componentes; desempenho físico
funcional.
Introduction
Aging is a natural process, which occurs changes characterized by physical
and cognitive modifications, as well declines in all body system leading to structural
and functional deterioration that may affect the level of physical activity, quality
of life and physical functional performance [1,2]. Older adults
population usually represents low levels in physical functional performance (PFP)
due to deterioration of important body systems as the musculoskeletal, cardiorespiratory
and nervous system [3,4]. PFP is defined as the efficiency of older people to accomplish
safely to physical demands of daily life whether in simple or complex tasks [5,6].
This PFP is composed of six components: strength, agility/ dynamic balance, flexibility,
coordination and aerobic endurance [6].
The PFP level can define the success or failure of the chosen activity to
perform, as well directly connected with the autonomy [7]. Yet, a highly analyzed
variable in combining with PFP and related to the autonomy of the older adults in
daily life activities is mobility, which is characterized by more specific stimulations
for agility and balance, from the combination of tasks. In the functional evaluation,
the mobility established as an essential point because of the relations with physical
functional performance [8].
Functional and structural losses are inevitable during the aging process,
however scientific studies show that there is a possibility of improving or maintaining
the functions of the body system through the practice of physical activity [9,10].
Physical activity is important to preserve the physical functional performance and
the independence of older adults [11]. Studies report that the regular practice
of physical activity produces benefits in cognitive and motor aspects, providing
control of body composition, maintenance and increase of muscle strength, improvement
of flexibility, and positive effects on the metabolism of older adults population,
taking place as an important instrument of health promotion [12,11].
According to the increase of population and necessity to offer better life
conditions, exercise protocols has been created in order to understand the different
effects of physical activity on physical Functional Performance or its components
and what they bring as benefits [10]. For example, Pauli et al. [13] reported increased
flexibility, shorter time for the coordination and agility test in a group of older
adults who practiced different types of moderate intensity physical activity compared
to a group of older adults who did not practice physical activity. Similar results
were found by Scarabottolo [7] in a group of older individuals
who combined of strength training with functional training for 12 weeks, with significant
improvements in agility and strength.
Some protocols used dual task exercises protocol (to perform two tasks simultaneously)
to evaluate their effect on some aspects of physical Functional Performance. According
to Hisayo Yokoyama [14], the training protocol associated with dual task (or-motor
cognitive) is more beneficial than a single-task training, with improvement in extents
of cognitive functions and muscle strength. The training protocol with dual task
components showed to be effective in increasing the mobility of the older adults
[15]. In addition, studies indicate that the training associating two tasks seems
to benefit older adults mobility, presenting an increase
in gait speed after the training [16,17]. Even though there are numerous studies
that investigated the effects of training protocols for older adults, however, is
not totally elucidated the effect of the dual task on the components of Physical
Functional Performance and mobility of older adults, converting in to an important gap. In addition, many studies have performed
the assessment of PFP by separating components and not evaluating all components
[7,14,15]. Therefore, the aim of the present study was to verify the effect of dual
task in a training protocol in all components of physical functional performance
and mobility of older adults people.
Methods
Participants
Thirty older adults participated in this study (twenty-three female and seven
males; 66.48 ± 3.85 years). The participants were distributed into three randomized
groups: 1) Multi-component physical activity group (MC), 2) Dual Task Group (DT)
and 3) Control Group (CG). As inclusion criteria, participants should show age between
60 and 80 years old. In addition, participants were able to walk without assistance.
As exclusion criteria were: presence of neurological or musculoskeletal disorder
that made it impossible to perform the training protocol and tests; attending to
a systematic physical activity program (more than twice a week) or in the three-month
period before to the start of the study; score < 24 points based on the Mini
Mental State Examination (MMSE) scale [18]. Moreover, two consecutive faults or
a total of three or more faults during the twelve weeks of training. The Institutional
Ethics Committee of Federal University of Espírito Santo,
Vitória, ES, Brazil approved the study protocol (71272817.0.0000.5542). In addition,
all procedures were performed with the adequate understanding and written consent
of all participants.
Procedures
All data collection and training protocols were made at the Fitness Station
Gym in the city of Serra / ES. Participants were evaluated before the beginning
of training (pre training) and after 12 weeks of training (post training). The following
evaluation tools were used: 1) Anamnesis to characterize the profile of participants
with information such as age, weight, height and current and past pathological history.
2) Mini Mental State Examination (MMSE), for evaluation of cognitive functions related
to temporal / spatial orientation, memory, language, attention and calculation;
The MMSE score ranges from 0 to 30 points [18]. 3) AAHPERD test battery - American
Alliance for Health, Physical Education, Recreation and Dance, for evaluation of
five Physical Functional Performance components: Agility/ dynamic balance - time
to complete two circuits involving the task stand up of a chair, walk around cones
and return to the chair; Coordination - time to complete a task requiring a manipulation
of twelve soda cans in a precise; Strength endurance- Number of elbow flexion repetitions
associated with resistance in 30 s; Flexibility- sit-and-reach test; Aerobic endurance-
Time to complete an 880-yard walk [19]. 4) Timed Up and Go (TUG), for evaluation
of functional mobility. The participants sat in a firm chair and were instructed
to stand up from without using the arm rests and walk 3 m at their normal pace turn
180º around a cone and return to the chair to sit down [20]. In order to increase
the level of difficulty of the test it was performed associated with a second motor
task (holding a tray with two cups) and associated with a second cognitive task
(Countdown), named TUG motor and TUG cognitive, respectively. 5) The Baecke Questionnaire to assess the level of physical activity
in three specific domains: household activities, sporting activities, and other
physically active leisure. Scores are obtained through specific questions and the
relationship between type, frequency and intensity of activity. The level of physical
activity is proportional to the score [21].
Training
protocols
Both groups performed the same training protocol that included different
Physical Functional Performance components such as flexibility, agility, balance,
strength, aerobic endurance and coordination. All exercises were performed in three
sets of 10 to 12 repetitions. Each session lasted 50 minutes and was supervised
by a qualified professional. The first and second week of exercises corresponded
to the adaptive phase, which aimed at providing reeducation of functional tasks
such as walking, sit and stand up. The sessions were divided into three parts: warm-up
(5 minutes), with walk at their self-selected velocity; exercise training (35 minutes)
and static stretching (10 minutes). The DT group performed the training protocol
simultaneously with a second cognitive task. Cognitive exercises were based on MMSE,
involving temporal and spatial orientation (approximate time, day of the week, month
etc.), memory (short-term memory, which lasts for approximately 30 seconds), attention
and calculation (perform mathematical calculations) evocation (recent memory with
lasting minutes, weeks or months), language (reading, repetition and naming objects),
repetition (auditory discrimination). The dependent variables calculated were: Agility/
dynamic balance(s), coordination(s), strength endurance (number of repetitions),
aerobic endurance(s), flexibility (cm) and TUG, TUG motor and TUG cognitive(s).
Statistical
analysis
After data normality and homogeneity of variance assumptions were tested
and fulfilled, one MANOVA-one way with repeated measures were employed (Group [Control
group, Multi-component and Dual]) for the all variables of Physical Functional Performance
and mobility. All dependent variables were calculated using Delta calculation (D = post Training – pre Training) to verify possible effects of the physical
training protocol between the groups, with group factor (MC, DT, CG) for analysis
of the following AAHPERD test variables: dynamic agility/balance, coordination,
strength endurance, flexibility and aerobic endurance, and TUG: Functional Mobility
(task execution time). Appropriate follow-up univariate analyses were performed,
when applicable, with the overall significance level set at .05. All analyses were
performed using SPSS (SPSS for Windows 10.0). One-way analysis of variances (ANOVAs)
were computed to compare age, anthropometric (height and body mass) and clinical
characteristics (MMSE, and Baecke scores) between groups.
Results
Sample
characteristics
The
groups were similar in age (GC= 66.1 years |MC= 67 years |DT= 65.8 years), cognition
and level of physical (Table I). The volunteers obtained total frequency in the
physical exercise programs.

Physical
functional performance variables
MANOVA showed a significant effect of group (Wilks' Lambda = 0.232, F10.46=
4.955, p < 0.01). ANOVA showed a significant effect of agility/ dynamic balance
(F2.27 = 4.373, p = 0.023), coordination (F2.27 = 10.572, p < 0.001), flexibility
(F2.27 = 9.936, p = 0.001) and aerobic endurance (F2.27 = 3.9, p = 0.03), but no
effect of strength endurance (F2.27 = 2.787, p = 0.079). Post hoc tests showed that
the MC and DT groups presented higher flexibility (3.0 cm/3.7 cm respectively)
and less time in coordination test (-9.9 s/-1.3 s respectively) compared to CG
(0.10 s / 0.4 s respectively). Furthermore, post hoc tests showed that the DT group
presented less time for the agility/ dynamic balance test than CG (-2.79 s/-2.1s
respectively), and MC showed less time for the aerobic endurance test than CG (-1.376
s /-6.2 s respectively) (Figure 1).
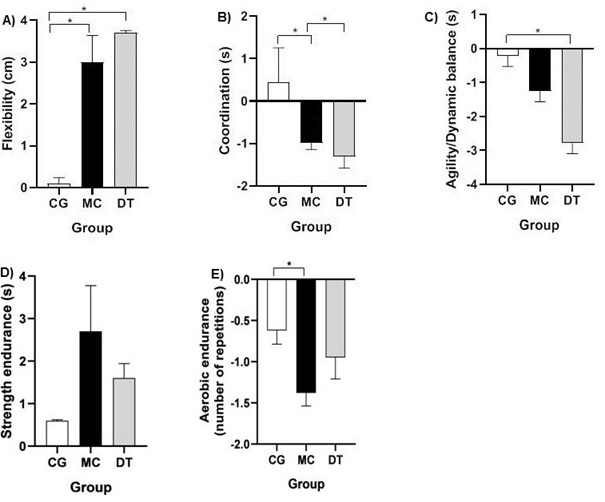
*(p≤0,05)
Figure
1 - Mean and standard deviation of the control (CG),
Multicomponent (MC) and Dual task (DT) groups in the following Physical Functional
Performance variables: flexibility (A), coordination (B), agility/ dynamic balance
(C), strength endurance (D), and aerobic endurance (E)
Functional
mobility variables
ANOVA showed a significant effect of mobility for the group (Wilks' Lambda=
0,519, F6,50= 3.234, p= 0.009). Post hoc tests revealed that MC and DT groups showed
lower time to perform the test TUG (-7600/-7900) compared to the CG (-2600) (p=0.033/
p=0.023 respectively). Thus, post hoc tests showed that the DT group had lower time
in the TUG M (-6000) test than compared to the CG (0.1000) (p=0.025) (Figure 2).
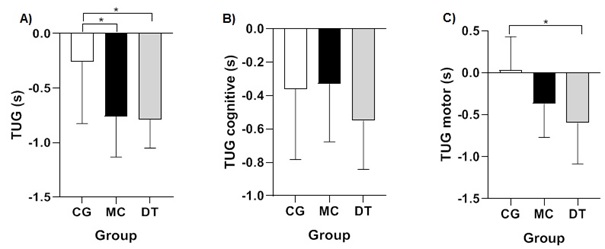
*p ≤ 0,05
Figure
2 - Mean and standard deviation of the control (CG),
Multicomponent (MC) and Dual task (DT) groups in the mobility variable, TUG (A),
TUG cognitive (B) and TUG motor (C)
Discussion
The aim of the present study was to verify the effect of dual task in a training
protocol in all components of Physical Functional Performance and mobility of older
adults. Overall, the dual task had no effect on the variables of Physical Functional
Performance, because both groups showed performed better in some aspects of CF and
mobility. This could be explained by the fact that physical activity generally promotes
positive impacts in functional aspects, such as increased aerobic capacity, preservation
of muscle mass, improved functionality and autonomy in activities [3,7,12].
In addition, performing two simultaneous tasks increases the demand for central
nervous system processing when compared to a single task, and the more attention
given to performing a task, the higher the level of interference in the secondary
task [22,23]. This interference can be improved by training, increasing performance
during the dual task [22]. Therefore, the addition of the dual task in the training
protocol may not have influenced the variables of the Physical Functional Performance
due to the low level of difficulty and complexity of the secondary task, not being
challenged enough to generate impact on the CF variables.
In relation to CF, both groups (MC and DT) presented differences for the
variables of flexibility and coordination, corroborating with the results found
by Pauli et al. [13], where the coordination and flexibility effects of older
adults people who practiced different types of physical activity at moderate intensity
were evaluated, using the AAHPERD scale as an analysis tool. In the present study,
the only variable that did not present an effect was muscle strength, which can
be explained by the fact that the activities were not directed to the systematic
training of muscle strengthening. Carvalho et al. [24] compared the muscular
strength of the older adults before and after 24 weeks of two types of training
(Multi-components and resistance). No differences were found for muscle strength
in the multicomponent physical activity group. The study concludes that multi-component
training does not appear to influence muscle strength; however, resistance training
in the multi-component exercise protocol improves muscle strength in the older adults.
In addition, the present study the Multi-component physical activity group
presented better performance in aerobic endurance, which can be explained by the
fact that they are only dedicating themselves to single task. In addition, exercise
protocols of the present study favor the impact of this variable, due to the number
of aerobic exercise time in the training protocol. The magnitude of aerobic endurance
improvement is determined by the intensity and frequency of exercise [25].
In relation to mobility, Menezes et al. [26] found an improved mobility
by decreasing the time to perform the TUG test of the older adults after four months
of intervention with multi-component protocol; Lorca and Lepe
[27] also found that the older adults perform the fastest TUG test after a year
of muscle strength training, flexibility and balance. Also, studies report that
dual-task training leads to better performance in the mobility of the older adults,
as shorter time to perform the TUG test [14,15] and increased gait speed [16,17].
In the present study, similar results were found, because both training protocols
improved performance during the TUG test, with shorter test time after training.
This result was precipitated, since the practice of physical activity being maintained
or improving the mobility of the older adults [28]. In the mobility test associated
with a second motor task, the DT group presented shorter test time and better performance
than the CG. Hisayo Yokoyama [14] evaluated the effect of dual-task training on
executive functions and concluded that cognitive-motor dual-task training was more
beneficial than single-task training in improving broader domains of cognitive functions
in older people. The improvement of executive function may be a possible explanation
for the better performance of the DT group in the dual task mobility test when compared
to the CG.
The second task proposed in the protocol of this study may not have been
complex enough to generate an effect on Physical Functional Performance. The aging
process causes deterioration in the central nervous system, however, these changes
are limited to more complex processes, such as executive function, which refers
to the ability to plan strategies [29] so maybe the difference between the protocols
was not found because the second task was not complex enough. A possible limitation
of the study was the low complexity of the second task in the training protocol,
and the training time. Thus, for future studies we suggest a greater complexity
of the second task and an increase in total training time.
Conclusion
Both training protocols improve the Physical Functional Performance of the
older adults, regardless of the dual task in training
References
- Macena WG, Hermano LO, Costa
TC. Alterações fisiológicas decorrentes do envelhecimento. Rev
Mosaicum 2018;27:223-36.
- Nascimento CM, Ingles M, Salvador-Pascual A, Cominetti
MR, Gomez CMC, Viña J. Sarcopenia, frailty and their
prevention by exercise. Free Radic Biol Med 2018;132:42-9. https://doi.org/
10.1016/j.freeradbiomed.2018.08.035
- Tomás
MT, Galán-Mercant A, Carnero
EA, Fernandes B. Functional capacity and levels of physical activity in aging: A
3-year follow-up. Front Med 2017;9(4):244. https://doi.org/10.3389/fmed.2017.00244
- Carmona
JJ, Michan S. Biology of healthy aging and longevity.
Rev Invest Clin 2016;68(1):7-16.
- Berlezi EM, Farias AM, Dallazen F, Oliveira KR, Pillatt AP,
Fortes CK. Analysis of the functional capacity of elderly residents of communities
with a rapid population aging rate. Rev Bras Geriatr Gerontol 2016;19(4):643-52. https://doi.org/10.1590/1809-98232016019.150156
- Clark
BA. Tests for fitness in older adults: AAHPERD Fitness Task Force. Joperd 1989;60(3):66-71. https://doi.org/10.1080/07303084.1989.10603976
- Scarabottolo CC, Garcia JJR, Gobbo LA,
Alves MJ, Ferreira AD, Zanuto EAC et al. Influence of physical exercise on the functional capacity in institutionalized
elderly. Rev Bras Med Esporte 2017;23(3):200-3. https://doi.org/10.1590/1517-869220172303150175
- Lin
SI, Lee HC, Chang KC, Yang YC, Tsauo JY. Functional
mobility and its contributing factors for older adults in different cities in Taiwan.
J Formos Med Assoc 2017;116(2):72-9. https://doi.org/10.1016/j.jfma.2016.01.011
- Ferreira CB, Teixeira PDS,
Alves dos Santos G, et al. Effects of a 12-week exercise
training program on physical function in institutionalized frail elderly. J Aging
Res 2018;2018:1-9. https://doi.org/10.1155/2018/7218102
- Pereira AMG, Paulo TRS,
Santos SFS. Efeito do exercício físico na capacidade funcional e atividade da vida
diária em idosos: revisão sistemática. ACTA Brasileira do Movimento Humano 2015;5(2):79-95.
- Nelson ME , Rejeski WJ, Blair SN, Duncan PW,
Juiz JO, Rei AC, et al. Physical activity and public
health in older adults: recommendation from the American College of Sports Medicine
and the American Heart Association. Med Sci Sports Exerc
2007;39(8):1435-45. https://doi.org/10.1249/mss.0b013e3180616aa2
- Granacher U, Hortobágyi
T. Exercise to improve mobility in healthy aging. Sports Med 2015;45:1625-26. https://doi.org/10.1007/s40279-015-0405-9
- Pauli J, Souza LS, Zago AS, Gobbi S. Influência de 12
anos de prática de atividade física regular em programa supervisionado para idosos.
Rev Bras Cineantropom Desempenho Hum 2009;11(3):255-60. https://doi.org/10.5007/1980-0037.2009v11n3p255
- Yokoyama H, Okazaki
K, Imai D, Yamashina Y, Takeda
R, Naghavi N et al. The
effect of cognitive-motor dual-task training on cognitive function and plasma amyloid
beta peptide 42/40 ratio in healthy Older adults persons: a randomized controlled
trial. BMC
Geriatr 2015;15(60):2-10. https://doi.org/10.1186/s12877-015-0058-4
- Brustio PR ,
Rabaglietti E, Formica S , Liubicich
ME. Dual-task training in older adults: The effect of additional
motor tasks on mobility performance. Arch Gerontol Geriatr 2018;75:119-24. https://doi.org/10.1016/j.archger.2017.12.003
- Gregory
MA, Gill DP, Zou G, Liu-Ambrose T, Shigematsu R, Fitzgerald
C, et al. Group-based exercise combined with dual-task training improves gait but
not vascular health in active older adults without dementia. Arch Gerontol Geriatr 2016;63:18-27. https://doi.org/10.1016/j.archger.2015.11.008
- Silsupadol P ,
Shumway-Cook A , Lugade V , Van DP , Chou LS , Mayr U.
Effects of single-task versus dual-task training on balance performance in older
adults: a double-blind, randomized controlled trial. Arch Phys Med Rehabil 2009;90(3):381-7. https://doi.org/10.1016/j.apmr.2008.09.559
- Melo
DM, Barbosa AJG. O
uso do Mini-Exame do Estado Mental em pesquisas com idosos
no Brasil: uma revisão sistemática. Ciênc Saúde Coletiva
2015;20(12):3865-76. https://doi.org/10.1590/1413-812320152012.06032015
- Benedetti TRB, Mazo GZ, Goncalves, LHT. Bateria de testes da AAHPERD: adaptação
para os institucionalizados. Rev Bras Cineantropom Desempenho Hum 2014;16(1):1-14.
https://doi.org/10.5007/1980-0037.2014v16n1p1
- Podsiadlo D, Richardson S. The timed
“Up & Go”: a test of basic functional mobility for frail older adults’ persons.
J Am Geriatr Soc 1991;39(2):142-8. https://doi.org/10.1111/j.1532-5415.1991.tb01616.x
- Voorrips
LE , Ravelli AC , Dongelmans PC , Deurenberg P , Van SWA. A physical activity questionnaire for the elderly. Med Sci Sports Exerc 1991;23(8):974-9.
- Matthews
A, Garry MI, Martin F, Summers J. Neural correlates of performance trade-offs and
dual-task interference in bimanual coordination: an ERP investigation. Neurosci Lett 2006;400(1):172-6. https://doi.org/10.1016/j.neulet.2006.02.043
- Ghai S, Ghai I,
Effenberg AO. Effects of dual tasks and dual-task training
on postural stability: a systematic review and meta-analysis. Clin Interv
Aging 2017;12:557-577. https://doi.org/10.2147/CIA.S125201
- Carvalho J, Marques E , Soares JM , Mota J . Isokinetic
strength benefits after 24 weeks of multicomponent exercise training and combined
exercise training in older adults. Aging Clin Exp Res 2010;229(1):63-9. https://doi.org/10.1007/BF03324817
- Varela
S, Ayan C , Cancela JM , Martin V . Effects of two different intensities
of aerobic exercise on elderly people with mild cognitive impairment: a randomized
pilot study. Clin Rehabil 2012;26(5):442-50.
https://doi.org/10.1177/0269215511425835
- Menezes AV, Aguiar AS, Alves
EF, Quadros LB, Bezerra PP. Efetividade de uma intervenção fisioterapêutica cognitivo-motora
em idosos institucionalizados com comprometimento cognitivo leve e demência leve.
Ciênc Saúde Colet 2016;21(11):3467-2016.
https://doi.org/10.1590/1413-812320152111.17892015
- Lorca NM, Lepe LM, Diaz NVP, Araya OE. Efectos de un programa de ejercicios para evaluar las capacidades funcionales y el balance de un grupo de adultos
mayores independientes sedentarios que viven en la comunidad.
Salud Uninorte. 2011;27(2):185-97.
- Wang
RY, Wang YL, Cheng FY, Chao YH, Chen CL, Yang YR. Effects of combined exercise on
gait variability in community-dwelling older adults. Effects of combined exercise
on gait variability in community-dwelling older adults. Age Dordr
2015;37(3):40. https://doi.org/10.1007/s11357-015-9780-2
- Poranen CT, Von BMB, Rantakokko M, Portegijs E, Eronen J, Kauppinen M, et al. Executive
function and life-space mobility in old age. Aging Clin Exp Res 2018;30(2):145-151.
https://doi.org/ 10.1007/s40520-017-0762-3