Rev Bras Fisiol Exerc 2021;20(1):93-100
doi: 10.33233/rbfex.v20i1.4090
REVIEW
Physical exercise during the COVID-19 pandemic for
individuals with a risk factor for cardiovascular disease: benefits and safety
Exercício
físico durante a pandemia da COVID-19 para indivíduos com fator de risco para
doença cardiovascular: benefícios e segurança
Wallace
Machado Magalhães de Souza1,2,3, Diogo Van Bavel
Bezerra1,4, Michel Silva Reis1,2,4
1Grupo de Pesquisa em Avaliação e
Reabilitação Cardiorrespiratória (GECARE), Universidade Federal do Rio de
Janeiro, Rio de Janeiro, RJ, Brasil
2Universidade Federal do Rio de Janeiro,
Rio de Janeiro, RJ, Brasil
3Centro de Cardiologia do Exercício,
Instituto Estadual de Cardiologia Aloysio de Castro (CCEx/IECAC),
Rio de Janeiro, RJ, Brasil
4Instituto do Coração Edson Saad,
Universidade Federal do Rio de Janeiro (ICES/UFRJ), Rio de Janeiro, RJ, Brasil
Received on: May 3, 2020; accepted on:
September 8, 2020.
Correspondence: Wallace Machado Magalhães de Souza, Grupo de Pesquisa em
Avaliação e Reabilitação Cardiorrespiratória, Universidade Federal do Rio de
Janeiro, Rua Prof. Rodolpho Paulo Rocco, 255, 21941-590 Rio de Janeiro RJ
Wallace Machado Magalhães de Souza: wallacemachado@ufrj.br
Diogo Van Bavel Bezerra:
diogobavel@gmail.com
Michel Silva Reis: msreis@hucff.ufrj.br
Abstract
Introduction: Physical
exercise is one of the main components of the cardiovascular rehabilitation
program (CR). However, due to the social isolation adopted by public
authorities because of the new coronavirus pandemic (COVID-19), the performance
of CR in an outpatient setting is impractical at this time. Objective:
To discuss about safe, efficient, and pleasant physical exercise strategies for
individuals with clinically stable risk factors for cardiovascular disease,
outside the traditional CR environment. Methods: Narrative literature
review with search of the sources made in Medline databases via PubMed and
Scientific Electronic Library Online (SciElo),
without date limit, with the key-words: physical exercise, coronavirus,
cardiovascular rehabilitation and risk factors for cardiovascular disease, in
Portuguese and English. Results: 25 articles and 1 book in electronic
format were included. Conclusion: The physical exercise program improves
functional capacity, muscle strength, oxygen perfusion, mental and social status and quality of life, minimizing the negative impact
of social isolation on health. Thus, the recommendations suggested in this
article are safe measures that bring benefits to individuals with risk factors
for CVD.
Keywords: cardiovascular rehabilitation;
functional capacity; coronavírus.
Resumo
Introdução: O exercício físico é um dos principais
pilares do programa de reabilitação cardiovascular (RC). Entretanto, devido ao
isolamento social adotado pelas autoridades públicas por causa da pandemia da
infecção provocada pelo novo coronavírus (COVID-19),
a realização de RC em ambiente ambulatorial é impraticável neste momento. Objetivo:
Discutir sobre estratégias seguras, eficientes e prazerosas de exercícios
físicos para indivíduos com fatores de risco para doença cardiovascular (DCV),
clinicamente estáveis, fora do ambiente tradicional de RC. Métodos:
Revisão de literatura narrativa com busca das fontes realizadas nas bases de
dados Medline via PubMed e Scientific
Electronic Library Online (SciElo),
sem limite de data, com as palavras-chave: exercício físico, coronavírus, reabilitação cardiovascular e fatores de risco
para doença cardiovascular, em português e inglês. Resultados: Foram
incluídos 25 artigos e 1 livro no formato eletrônico. Conclusão: O
programa de exercício físico provoca melhoras na capacidade funcional, força
muscular, perfusão de oxigênio, estado mental e social e a qualidade de vida,
minimizando o impacto negativo do isolamento social na saúde. Desta forma, as
recomendações sugeridas neste artigo são medidas seguras e que trazem
benefícios para indivíduos com fatores de risco para DCV.
Palavras-chave: reabilitação cardiovascular;
capacidade funcional; coronavírus.
Introduction
Patients with
risk factors for cardiovascular disease (CVD) (i.e., obesity, systemic arterial
hypertension, diabetes mellitus, and dyslipidemia) are eligible for
cardiovascular rehabilitation (CR) programs. Outpatient CR involves several
components to improve the physical, mental, and social health of the
participants and must occur under the supervision of a multi-professional team composed
of doctors, physiotherapists, Physical Education teachers, nutritionists,
psychologists, social workers, and nurses. In this environment, educational
activities are carried out on health care in several aspects. Among the
activities developed in outpatient CR, physical exercise is one of the main
pillars due to its well-pronounced benefits in functional capacity, in the
control of risk factors, and the quality of life in this population [1].
However, the
social isolation measures certainly adopted by the World Health Organization
(WHO) and public authorities due to the pandemic of the new coronavirus
infection (COVID-19), caused by SARS-CoV-2, prevent the practice of physical
exercises in CR is carried out by security measures of this population. Data
presented by the Chinese Center for Disease Control and Prevention point to a
lethality rate of 2.3% by COVID-19 (1,023 deaths out of 44,672 confirmed
cases). Still, when patients had some risk factors for CVD, such as systemic
arterial hypertension or diabetes mellitus, this rate reached 10.5%, which
shows that this population is more vulnerable when infected by the virus [2].
This social seclusion can induce sedentary behaviors, favoring an increase in
body mass, an increase in systemic blood pressure, greater intolerance to
glucose, dyslipidemia, as well as psychosocial disorders such as depression and
anxiety [3]. The psychological impact of prolonged quarantine is associated
with feelings of anger, frustration, boredom, controversial information (i.e.,
fake news), and financial losses [4].
Therefore, due
to this challenging scenario that will last for a long period, the objective of
this article is to discuss the safety of prescription, efficiency and
enjoyment of physical exercises for requirements with risk factors for
clinically stable CVD (i.e., with optimized medication and no signs/symptoms of
uncontrolled blood pressure and/or blood glucose) for the traditional CR
environment.
Methods
A
narrative literature review was carried out with the search for sources made on
Medline via PubMed and Scientific Electronic Library Online (SciElo), with no date limit, with the key-words: physical
exercise, coronavirus, cardiovascular rehabilitation and risk factors for
cardiovascular disease, in Portuguese and English.
Benefits of physical exercise
If, on the one
hand, social isolation is crucial for patients with risk factors for CVD,
avoiding greater exposure to the virus, on the other hand, this withdrawal can
lead to a reduction in daily physical activities and physical exercise
practices [5]. Physical exercise is a way to improve the health of this
population, with significant effects on glucose metabolism, on skeletal muscle
function, on the respiratory, cardiac, and bone systems [6], on improving
mental health [7], on endothelial function, reduced levels of lipoproteins and
atherosclerotic lesions [8] and other organs (Figure 1).
Prolonged
periods of physical inactivity lead to changes in the sympathovagal
modulation and oxidative function of skeletal muscle, resulting in reduced
stroke volume and peripheral muscle dysfunction [9]. WHO data from 2016
indicate that 44% of the causes of death worldwide were cardiovascular
etiology. When physical inactivity is associated with some heart disease, the
risk of mortality increases significantly [10].
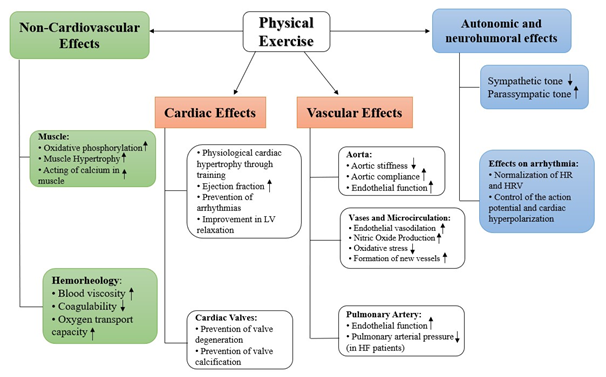
HR =
Heart rate; HRV = Heart rate variability; HF = Heart failure; LV = Left
ventricle. Niebauer J, 1996 [11]; Gielen
et al., 2010 [12].
Figure 1 - Effect of physical exercise
on the myocardium, blood vessels, and skeletal muscle
In patients with
risk factors for CVD, there is a significant improvement in functional
capacity, blood pressure, and quality of life with interventions through
aerobic and/or strength exercise, with no risk associated with disease
progression [13,14]. A study carried out with 5,641 patients with coronary
artery disease submitted to a CR program concluded that an increase of 1 MET
(metabolic equivalent) was able to reduce the risk of cardiovascular mortality
by 25% [15]. A recent meta-analysis pointed out that aerobic training combined
with strength training improved oxygen consumption at peak effort (VO2peak),
muscle strength, and quality of life in patients with heart failure, mainly due
to improved transport capacity and use of oxygen by peripheral musculature
[16].
Physical
exercise at home environment is considered an essential tool for the prevention
and treatment of diseases related to physical inactivity, especially in
situations where practice outside this environment is not possible [17]. In
this sense, even minimal amounts of physical exercise at home environment
(e.g., walking for 20 minutes) promote reductions in the risk of mortality from
CVD by improving systemic blood pressure and glycemic control [18].
Thus, physical
exercise promotes physiological adaptations that increase the perfusion and
oxygen supply to the cardiac and skeletal muscle, resulting in improvement of
peripheral muscle dysfunction, as a consequence, contributing to the reduction
of effort intolerance and risk of cardiovascular mortality in individuals with
factors risk factors for CVD [19].
Recommendations for physical exercise prescription
The current
Brazilian Cardiovascular Rehabilitation Guideline provides the following
recommendations for patients with clinically stable CVD risk factors for
physical exercise and will be presented in Chart 1 [1]:
Chart 1 - Recommendations for exercises
to improve functional capacity in cardiac patients
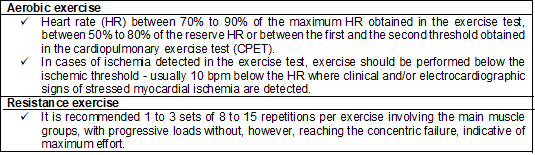
HR =
Heart rate. CPET = Cardiopulmonary exercise test. Carvalho et al., 2020 [1]
Although the
recommendations for exercise intensity are based on physiological parameters
(i.e., HR), the use of these indices can be difficult to monitor by the
patients themselves due to 1) lack of technological resources to monitor HR
(e.g., heart rate monitor); 2) lack of knowledge on how to measure HR using the
radial pulse and; 3) the influence of the fitness level on the HR response,
through sympathovagal modulation, in which the same
absolute HR value can represent a different physiological response, according
to the individual's fitness level.
As an
alternative that is easily accessible and understood by most people, especially
when performing physical exercises without direct supervision by a
multi-professional team, the intensity of the effort can be controlled by a
subjective effort perception scale. Among these scales, the most known and used
is the Borg Scale [20], which was originally developed on a scale of 6 to 20
and, alternatively, has a version adapted on a scale of 0 to 10 (Picture 2).

Borg,
1990 [20]
Figure 2 - Borg Scale (scale from 0 to
10)
The use of the
Borg Scale is a strategy widely used in exercise tests and the prescription of
physical exercise, both for cardiac patients and healthy individuals [21,22].
The safe training intensity should represent an effort up to 4 (on a scale from
0 to 10), corresponding to the intensity considered moderate. Thus, as a way of
controlling the intensity of effort, the Borg Scale is an important control
tool for self-monitoring during physical exercises [23].
Thus, the
physical exercise program for patients with risk factors for CVD to perform at
home should consider the following points:
- Training frequency: Three to five times a week,
respecting the rest interval so that there are no harmful effects on the body
due to overtraining.
- Session duration: Initially, 20 minutes a day,
progressing gradually until reaching 60 minutes a day.
- Intensity: HR or Borg Scale, as previously discussed.
- Modality: Due to limited resources and space, it is
recommended that circuit exercises with their body weight and using home
equipment (i.e., chair, broom, bottles).
- Safety: It must be ensured that the place does not
have objects that can facilitate the fall or cause trauma during the execution
of physical exercises (i.e., carpets, furniture, toys). Also, whenever
possible, monitor the levels of blood pressure (hypertension) and capillary
blood glucose (diabetics) before and after exercise.
The training
sessions must consist of: 1) the warm-up phase, to
prepare the body for the increase in physiological demand; 2) training itself
and; 3) cool down, to help to return physiological parameters to rest indexes.
Physical
exercises should be stopped immediately if angina, severe dyspnoea,
syncope, and headache are present. However, in the presence of fever, the
practice of physical exercise is contraindicated, at least on that day.
Suggested physical exercises to be performed at home
There is a
challenge in prescribing physical exercises in the home environment due to the
limitation of equipment/resources for the execution of different types of
movements and the difficulty in controlling the variables and performing the
exercises. Besides, the physical exercise program should promote pleasant
experiences for the individual in a way that facilitates their adherence to a
daily training routine [24]. With that in mind, the American College of
Exercise Medicine (ACSM) and the Brazilian Society of Cardiology (SBC) prepare
documents that endorse the importance of staying active during this period and
suggestions for exercises that can be performed safely, pleasantly, and
efficiently indoors (Figure 3) [23,25]:
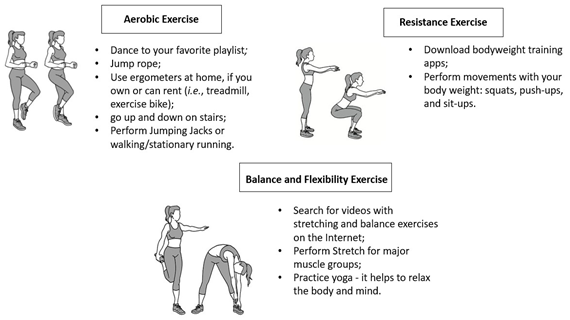
Reis
et al., 2020 [23]; American College of Sports Medicine, 2020 [25]
Figure 3 - Suggested physical exercises
to be performed at home
Bearing in mind
that social support is an essential factor for adhering to the physical
exercise program, establishing a positive relationship to encourage this
practice among family members is crucial for regular training and especially
maintenance in this training program [26]. In this way, exercises that involve
the spouse, children, and other family members can increase the positive
aspects of the training experience and promote greater adherence during the
period of pandemic and social isolation [24].
Conclusion
In this context,
it is extremely important for patients with risk factors for CVD to remain
physically active during the period of social isolation since sedentary
behavior causes damage in the clinical and functional framework. The physical
exercise program improves functional capacity, muscle strength, oxygen
perfusion, mental and social status, and quality of life. Following the
guidelines presented in this article can minimize the negative impact of social
isolation on health. Thus, the recommendations suggested in this article are
safety measures that bring benefits to individuals with risk factors for CVD.
Conflict of interest
The authors declare that they have no conflict of
interest.
Financing source
There were no sources of external funding for this
study.
Authors' contributions
Conception and design of the research:
Souza WMM, Bezerra DVB. Data collection: Souza
WMM, Bezerra DVB. Analysis and interpretation of
data: Souza WMM, Bezerra DVB. Writing of the
paper: Souza WMM, Bezerra DVB, Reis MS. Critical
review of the paper for important intellectual content: Reis MS.
References
- Carvalho
T, Milani M, Ferraz AS, Silveira AD, Herdy AH, Hossri CAC et al. Diretriz Brasileira de Reabilitação
Cardiovascular – 2020. Arq Bras
Cardiol 2020;114(5):849-93. doi: 10.36660/abc.20200407 [Crossref]
- Guo T, Fan Y, Chen M, Wu X, Zhang L, He T et al. Cardiovascular implications of fatal outcomes of patients with coronavirus disease 2019 (COVID-19). JAMA Cardiol 2020;5(7):811-18. doi: 10.1001/jamacardio.2020.1017 [Crossref]
- Ferreira MJ, Irigoyen MC, Consolim-Colombo F, Saraiva JFK, Angelis K. Physically Active Lifestyle as an Approach to Confronting COVID-19. Arq Bras Cardiol 2020;114(4):601-2. doi: 10.36660/abc.20200235 [Crossref]
- Jiménez-Pavón D, Carbonell-Baeza A, Lavie CJ. Physical exercise as therapy to fight against the mental and physical consequences of COVID-19 quarantine: Special focus in older people. Prog Cardiovasc Dis 2020. doi: 10.1016/j.pcad.2020.03.009 [Crossref]
- Brooks SK, Webster RK, Smith LE, Woodland L, Wessely S, Greenberg N et al. The psychological impact of quarantine and how to reduce it: rapid review of the evidence. Lancet 2020;395(2):912-20. doi: 10.1016/S0140-6736(20)30460-8 [Crossref]
- Fiuza-Luces C, Garatachea N, Berger NA, Lucia A. Exercise is the real polypill. Physiology (Bethesda) 2013;28(5):330-58. doi: 10.1152/physiol.00019.2013 [Crossref]
- Mikkelsen K, Stojanovska L, Polenakovic M, Bosevski M, Apostolopoulos V. Exercise and mental health. Maturitas 2017;106(9):48-56. doi: 10.1016/j.maturitas.2017.09.003 [Crossref]
- Santos LF, Vicente GA, Correa LMA. Reabilitação cardiovascular com ênfase no exercício físico para pacientes com doença arterial coronariana: visão crítica do cenário atual. Revista da Sociedade de Cardiologia do Estado de São Paulo 2019;29(3):303-13. doi: 10.29381/0103-8559/20192903306-13 [Crossref]
- Perhonen
MA, Franco F, Lane LD, Buckey JC, Blomqvist
CG, Zerwekh JE et al. Cardiac atrophy
after bed rest and spaceflight. J Appl Physiol (1985)
2001;91(2):645-53. https://doi:10.1152/jappl.2001.91.2.645 [Crossref]
- Benjamin EJ, Muntner P, Alonso A, Bittencourt MS, Callaway CW, Carson AP, et al. Heart disease and stroke statistics-2019 update: a report from the American Heart Association. Circulation 2019;139(10):e56-e528. doi: 10.1161/CIR.0000000000000659 [Crossref]
- Niebauer J, Cooke JP. Cardiovascular effects of exercise: role of endothelial shear stress. J Am Coll Cardiol 1996;28(7):1652-60. doi: 10.1016/S0735-1097(96)00393-2 [Crossref]
- Gielen S, Schuler G, Adams V. Cardiovascular effects of exercise training: molecular mechanisms. Circulation 2010;122(12):1221-38. doi: 10.1161/CIRCULATIONAHA.110.939959 [Crossref]
- Bocchi EA. Exercise training in Chagas' cardiomyopathy: trials are welcome for this neglected heart disease. European Journal of Heart Failure 2010;12(8):782-4. doi: 10.1093/eurjhf/hfq124 [Crossref]
- Laoutaris ID, Adamopoulos S, Manginas A, Panagiotakos DB, Kallistratos MS, Doulaptsis C et al. Benefits of combined aerobic/resistance/inspiratory training in patients with chronic heart failure. A complete exercise model? A prospective randomised study. Int J Cardiol 2013;167(5):1967-72. doi: 10.1016/j.ijcard.2012.05.019 [Crossref]
- Martin BJ, Arena R, Haykowsky M, Hauer T, Austford LD, Knudtson M et al. Cardiovascular fitness and mortality after contemporary cardiac rehabilitation. Mayo Clin Proc 2013;88(5):455-63. doi: 10.1016/j.mayocp.2013.02.013 [Crossref]
- Gomes-Neto M, Durães AR, Conceição LSR, Roever L, Silva CM, Alves IGN et al. Effect of combined aerobic and resistance training on peak oxygen consumption, muscle strength and health-related quality of life in patients with heart failure with reduced left ventricular ejection fraction: a systematic review and meta-analysis. Int J Cardiol 2019;293(6):165-75. doi: 10.1016/j.ijcard.2019.02.050 [Crossref]
- Schwendinger F, Pocecco E. Counteracting physical inactivity during the COVID-19 pandemic: Evidence-based recommendations for home-based exercise. Int J Environ Res Public Health 2020;17(6):2-6. https://doi:10.3390/ijerph17113909 [Crossref]
- Castro RRT, Neto JGS, Castro RRT. Exercise training: a
hero that can fight two pandemics at once. International Journal of
Cardiovascular Sciences 2020;33(3):284-7. doi: 10.36660/ijcs.20200083 [Crossref]
- Drexler H, Riede U, Münzel T, König H, Funke E, Just H. Alterations of skeletal muscle in chronic heart failure. Circulation 1992;85(5):1751-9. doi: 10.1161/01.CIR.85.5.1751 [Crossref]
- Borg G. Psychophysical scaling with applications in physical work and the perception of exertion. Scand J Work Environ Health 1990;16 Suppl 1:55-8. https://doi:10.5271/sjweh.1815 [Crossref]
- Kaercher PLK, Glänzel MH, Rocha GG, Schmidt LM, Nepomuceno P, Stroschöen L et al. Escala de percepção subjetiva de esforço de Borg como ferramenta de monitorização da intensidade de esforço físico. Revista Brasileira de Prescrição e Fisiologia do Exercício 2018;12:1180-5.
- Meneghelo RS, Morhy SS, Zucchi P. Time of exercise as indicator of quality control in ergometry services. Arq Bras Cardiol 2014;102(2):151-5. doi: 10.5935/abc.20140005 [Crossref]
- Reis
MS, Oliveira GMM, Guio BM, Bezerra DVB, Pinto EP, Nasser I et al. Como cuidar
do seu coração na pandemia da COVID-19: Recomendações para a prática
de exercícios físicos e respiratórios. Rio
de Janeiro. Universidade Federal do Rio de Janeiro (UFRJ),
Departamento de Fisioterapia, Programa de
Pós-Graduação em Educação
Física e Cardiologia,
Grupo de Pesquisa em Avaliação e
Reabilitação Cardiorrespiratória (GECARE); 2020. p.1-21. [Cited 2021 dez 10]. Available from: http://poscardio.ufrj.br/images/documentos/EBook_COVID19_respirat%C3%B3ria.pdf
- Oliveira
Neto L, Elsangedy HM, Tavares VDO, Teixeira CVLS, Behm DG, Da Silva-Grigoletto ME. #TrainingInHome
- Home-based training during COVID-19 (SARS-COV2) pandemic: physical exercise
and behavior-based approach. Rev Bras Fisiol Exerc 2020;19(2):S9-S15. doi: 10.33233/rbfe.v19i2.4006 [Crossref]
- American College of Sports Medicine. Staying active
during the coronavirus pandemic exercise is medicine, 2020. [cited 2020 abr
15]. Available from: https://www.exerciseismedicine.org/assets/page_documents/EIM_Rx%20for%20Health_%20Staying%20Active%20During%20Coronavirus%20Pandemic.pdf
- Pridgeon L, Grogan S. Understanding exercise adherence and dropout: an interpretative phenomenological analysis of men and women’s accounts of gym attendance and non-attendance. Qualitative Research in Sport, Exercise and Health 2012;4(8):382-99. doi: 10.1080/2159676X.2012.712984 [Crossref]