Rev Bras Fisiol exerc 2021;20(3):315-24
doi: 10.33233/rbfex.v20i3.4244
ORIGINAL ARTICLE
Concurrent validity and intrarater
reliability of the Glittre ADL-Test in obstructive
sleep apnea
Validade
concorrente e reprodutibilidade intra-avaliador do
teste de AVD-Glittre na apneia obstrutiva do sono
José
Carlos Nogueira Nóbrega Júnior¹, Armèle Dornelas de
Andrade2, Adília Karoline Ferreira Souza3, Maria Inês
Remígio de Aguiar2, Rodrigo Pinto Pedrosa4, Maria do
Socorro Brasileiro-Santos5, Anna Myrna
Jaguaribe de Lima6
1Facottur, Olinda, PE, Brazil
2Universidade Federal de Pernambuco,
Recife, PE, Brazil
3Universidade Estadual da Paraíba,
Campina Grande, PB, Brazil
4Pronto Socorro Cardiológico de
Pernambuco (PROCAPE), Universidade de Pernambuco, Recife, PE, Brazil
5Universidade Federal da Paraíba, João
Pessoa, PB, Brazil
6Universidade Federal Rural de
Pernambuco, Recife, PE, Brazil
Received:
30 June 2020; Accepted: 27 January 2021.
Correspondence: Anna Myrna Jaguaribe de Lima,
Universidade Federal Rural de Pernambuco, Rua Dom Manuel de Medeiros, s/n, Dois
Irmãos, 52171-900 Recife PE
José Carlos Nogueira Nóbrega Júnior:
carlos_noobrega@hotmail.com
Armèle Dornelas de Andrade:
armeledornelas@hotmail.com
Adília Karoline Ferreira Souza: adiliakfsfisio@gmail.com
Maria Inês Remígio de Aguiar: miremigio@yahoo.com.br
Rodrigo Pinto Pedrosa: rppedrosa@terra.com.br
Maria do Socorro Brasileiro-Santos: sbrasileiro@yahoo.com
Anna Myrna Jaguaribe de Lima:
anna.myrna@ufrpe.br
Abstract
Objective: To evaluate the concurrent
validity and intrarater reliability of the Glittre-ADL test to determine exercise capacity in subjects
with obstructive sleep apnea (OSA). Methods: Twenty-two (22) subjects
with mild to severe OSA (50.7 ± 11.2 years, 32.0 ± 4.0 kg/m2)
performed the Glittre-ADL test and the
cardiopulmonary exercise testing (CPET). The tests were carried out in two
different days, twice a day, and the order was determined by randomization. Results:
The maximum HR (HRmax) in the Glittre-ADL test was
130.6 ± 13.3 bpm. Regarding the variables related to CPET, the volunteers had
values of maximal oxygen consumption (VO2max) of 25.4 ± 5.3
ml/kg/min, VO2 on the first threshold of 19.4 ± 3.9 ml/kg/min and
maximum HR of 161.3 ± 15.2 bpm. A moderate negative correlation was found
between the Glittre-ADL test performance time and VO2max
(r = -0.424; p = 0.049). Excellent agreement and consistency between
measurements was observed in analyzing the test-retest reliability of the total
performance time of the Glittre-ADL test (intraclass
correlation coefficient (ICC) = 0.865, 95% CI: 0.379-0.965 (p ≤ 0.0001). Conclusion:
According to the results of the present study, Glittre-ADL
test is reliable and valid for evaluating functional exercise capacity in
patients with moderate and severe OSA. Furthermore, it also could be considered
as a submaximal clinical exercise tolerance test for this population.
Keywords: obstructive sleep apnea; exercise
tolerance; exercise test.
Resumo
Objetivo: O objetivo deste trabalho foi testar a
hipótese que o teste de AVD-Glittre (TGlittre) tem validade concorrente e reprodutibilidade intra-avaliador em indivíduos com apneia obstrutiva do sono
(AOS). Métodos: Foram avaliados 22 indivíduos, de ambos os sexos, com
diagnóstico AOS. O TGlittre e o teste de esforço
cardiopulmonar (TECP) foram realizados em dois dias diferentes, duas vezes
cada, e a ordem era determinada por randomização. Resultados: A FC
máxima (FCmáx) obtida no TGlittre foi de 130,6 ± 13,3 bpm
e o tempo total para a realização do teste foi de 3,4 ± 0,5 min. Sobre as
varáveis analisadas no TECP, foram obtidos os seguintes valores: consumo máximo
de oxigênio (VO2máx) = 2,4 ± 5,3 ml/kg/min, VO2 no
primeiro limiar = 19,4 ± 3,9 ml/kg/min, FCmáx
= 161,3 ± 15,2 bpm e o tempo total de realização do
teste foi de 8,3 ± 1,6 min. Uma correlação negativa moderada foi verificada
entre o tempo de realização do TGlittre e VO2max
(r = -0,424; p = 0,049). Na análise da confiabilidade teste-reteste do
tempo total de realização do TGlittre, foi observada
uma excelente concordância e consistência entre as medidas (coeficiente de
correlação intraclasse (CCI) = 0,865; IC95%: 0,379-0,965 (p ≤ 0,0001). Conclusão:
O teste de TGlittre é válido e reprodutível na AOS.
Além disso, é um teste de intensidade submáxima, fácil aplicação e baixo custo,
que pode ser utilizado em larga escala.
Palavras-chave: apneia obstrutiva do sono; tolerância
ao exercício; teste de esforço.
Introduction
Obstructive
sleep apnea (OSA) is characterized by recurrent hypoxia/reoxygenation patterns
that cause oxidative stress and muscle injury [1,2,3]. These bioenergetic and
structural changes in skeletal muscles are responsible for generalized fatigue
and impaired functional exercise capacity in these individuals [3,4]. In
addition, OSA may cause respiratory muscle weakness, thus promoting activation
of cardiovascular reflexes. The muscle abnormalities that commonly occur in OSA
associated with intermittent blood gas disorders compromise the integrity of
the cardiorespiratory system, triggering the decline of exercise tolerance
[5,6,7,8].
Thus, assessing
functional exercise capacity provides important information for the diagnosis
and prognosis of cardiopulmonary function through the behavior of metabolic,
cardiac, and respiratory systems during the cardiopulmonary exercise testing
(CPET) [9]. Despite CEPT is the gold standard to assess exercise tolerance, the
cost is high, and it requires specialized and trained personnel. Furthermore,
CEPT is a maximum exercise test and could be not well-tolerated in elderly with
comorbidities [10]. On the other hand, field tests appear as a less strenuous
alternative. In addition to presenting good correlation with the activities of
daily life, they are low cost, simply executed and easily reproducible [11,12].
In this context,
the Glittre-ADL test has been able to reflect the
functional limitations in studies with healthy subjects [13] and those affected
by varied conditions such as COPD [14,15], cardiovascular diseases [16] and
obesity [17].
Regarding OSA,
there are still no reports in the literature on the use of the Glittre-ADL test to determine exercise tolerance in these
subjects. Therefore, the objective of this study was to test the hypothesis
that the Glittre-ADL test has concurrent validity and
reliability in subjects with OSA.
Methods
Sample
This is a
cross-sectional study and was approved by the Human Research Ethics Committee
of the Federal University of Pernambuco (UFPE) in accordance with the
resolution 466/12 CNS (No: 1068362). All volunteers included in the study were
informed about the research and signed an informed consent form, designed by
the principal investigator.
Volunteers were
recruited from the Cardiologic Emergency Hospital of Pernambuco (PROCAPE) based
on the evaluation of 428 individual (medical) records. All volunteers underwent
a polysomnography (ApneaLink™-Resmed)
for OSA diagnosis. Patients aged between 30 years and 65 years, with AHI
(=Apnea Hypopnea Index) ≥ 15 events/hour (moderate to severe OSA),
without a history of musculoskeletal, pulmonary or
cardiac diseases and with BMI ≤ 39.9 kg/m2 were included in
the study.
An independent
evaluator who did not participate in patient recruitment or in the testing
performed the randomization for the test order, using the randomized.com software.
Cardiopulmonary exercise test (CPET)
To evaluate the
functional exercise capacity, CPET was performed using a treadmill ramp
protocol (Centurium 300, Micromed, Brazil) and ErgoPCElite® software associated with an electrocardiogram
(Micromed Brazil) with twelve derivations. In this
protocol, the system suggests the velocity and inclination to be increased, so
that the patient reaches their maximum oxygen consumption (VO2max)
within 10 minutes. The respiratory variables during exercise were obtained
under standard conditions of temperature (18-22ºC), pressure and humidity
(50-70%), and collected using a face mask attached to a gas analyzer (Cortex - Metalyzer II - Germany). The patient was instructed not to
verbally communicate during the examination, informing their levels of fatigue
through manual gestures and requesting the end of the examination only at the moment of exhaustion. The test was considered maximal
when the respiratory exchange ratio (R) was ≥ 1.1 [18].
Glittre-ADL
Test
The patients
were instructed to walk 10 meters with a backpack (5.0 kg for men and 2.5 kg
for women). The circuit consisted of 5 laps starting with the patient sitting
on a chair, and upon receiving the command they would get up and walk fast up
the middle of the course and go up and down a two-step staircase (17 cm height
x 27 cm deep). Then they would continue (walking) until the end of the circuit,
where there was a shelf containing three objects (1 kg each) on the highest
shelf. They should move them one by one to the middle shelf (waist height), and
finally to the lowest shelf (floor height). Next, the objects were replaced on
the middle shelf and then on the highest shelf. The patient re-did the course,
sitting, getting up and repeating the circuit. Heart rate (Frequency-Polar) and
peripheral oxygen saturation (Oximeter-Pulse Oximeter PM 50) were monitored at
each lap. Blood pressure and the subjective perception of effort (modified BORG
scale) were measured at baseline at the end and after two minutes of recovery
[19].
Two Glittre-ADL tests were performed within a maximum interval
of one week, and with an interval of at least twenty-four hours between them.
The data obtained for the fastest timed test were used for analyzing the
physiological responses. The formula used to calculate the estimated HRmax was:
HRmax.estimated=208-(0.7x age), described by Tanaka
H, Monahan K and Seals D [20].
Data analysis
Data were
analyzed using the SPSS software version 20.0. The Spearman correlation test was
used for the concurrent validation of the Glittre-ADL
test, and the intraclass correlation coefficient (ICC) and the Bland-Altman
method were used for the reliability evaluation. The results were presented as
mean and standard deviation, considering p < 0.05 as the level of
statistical significance.
Results
In figure 1 is
showed process of recruitment, allocation, follow-up
and analysis of the participants.
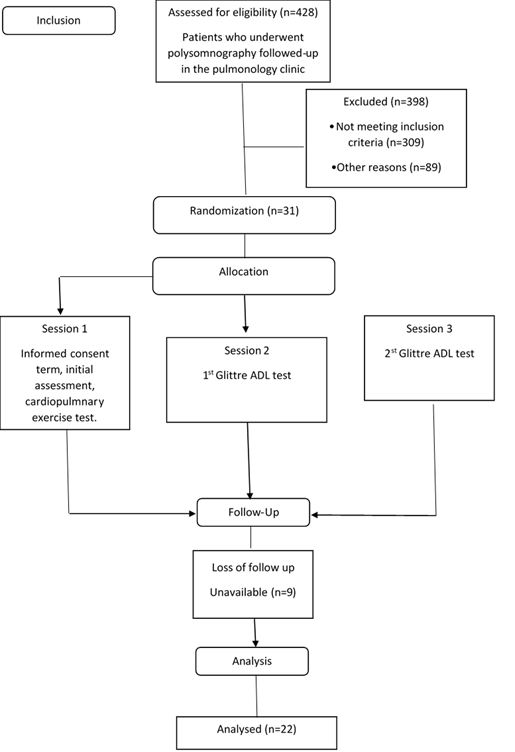
Figure 1 - Flow
diagram of patient recruitment and progress
Twenty-two
patients were evaluated (14 males (64%) and 8 females). The anthropometric and
clinical characteristics of the sample are shown in Table I. The sample mostly
consisted of individuals with OSA classified as severe (59.1%).
Table I - Characteristics
of the sample
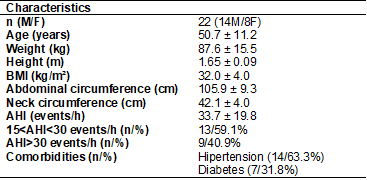
n = sample size; M =
males; F = females; BMI =body mass index; AHI = apnea-hipopnea
index. Data are reported as mean ± standard deviation and percentage
A negative and
moderate correlation (r = -0.424; p = 0.049) was found in figure 2 between the
VO2max obtained on CPET and the performance time for the Glittre-ADL test.
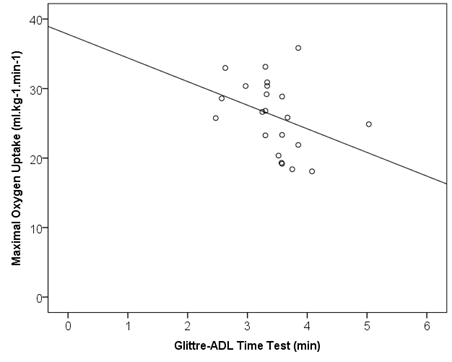
Figure 2 - Correlation
plot between maximal oxygen consumption and Glittre-ADL
time test (r = -0,424; p = 0,049)
Table II shows
the cardiorespiratory responses obtained on the maximum CPET and on the
submaximal Glittre-ADL test. The volunteers presented
VO2max values of 25.4 ± 5.3 ml/kg/min, VO2 at the first
threshold of 19.4 ± 3.9 ml/kg/min and HRmax of 161.3 ± 15.2 bpm. The HRmax was
130.6 ± 13.3 bpm for the Glittre-ADL test and the
HRmax (%predicted) for the Glittre-ADL test was 80.9
± 6.9% of the HRmax obtained on the CPET.
Table II - Results
of cardiopulmonary exercise testing and Glittre-ADL
test
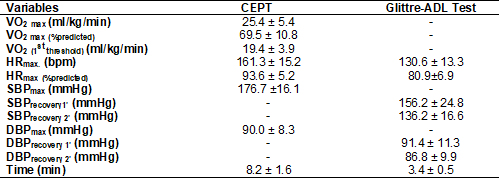
CEPT = cardiopulmonary
exercise testing; VO2max = maximal oxygen consumption; VO2
= oxygen consumption; HRmax = maximum heart rate; SBPmax = maximum systolic blood pressure;
SBPrecovery1’ = systolic blood pressure in the first minute of the recovery;
SBPrecovery2’ = systolic blood pressure in the second minute of the recovery; DBPmax = maximum diastolic blood pressure; DBPrecovery1’ =
diastolic blood pressure at the first minute of the recovery; DBPrecovery1’ =
diastolic blood pressure in the second minute of the recovery. Data are
reported as mean and standard deviation
In the
test-retest reliability for the total time to perform the Glittre-ADL
test, the intraclass correlation coefficient (ICC) presented high reliability
(0.865, 95% CI = 0.379-0.965, p < 0.0001) (Figure 3).
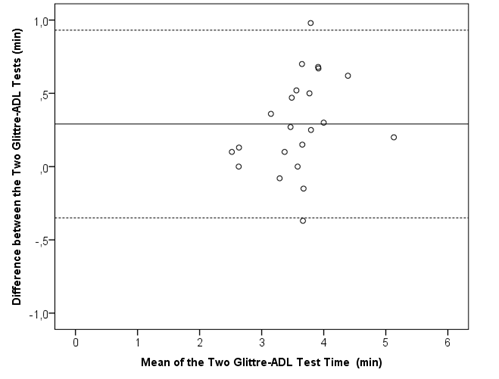
Figure 3 - Bland-Altman
plot of agreement between test and retest of Glittre-ADL
test
Discussion
This is the
first study to assess the concurrent validity and reliability of the Glittre-ADL test in OSA patients. The results showed a
moderate negative correlation between the performance time of the Glittre-ADL test and VO2max, showing an association
between the direct measurement of functional exercise capacity through the
CPET, and the indirect measurement of functional exercise capacity through
the Glittre-ADL test. Moreover, the test-retest
reliability found of the Glittre-ADL was excellent,
showing good agreement and consistency between the intra-rater measurements.
In the present
study, the Glittre-ADL test can be considered an
alternative to evaluate exercise tolerance, since a moderate concurrent
validity was found between the Glittre-ADL test
performance time and the VO2max obtained on the CPET. The Glittre-ADL
test has already been used to assess exercise capacity in healthy subjects and
in diseases such as COPD [14,15], heart failure [16] and obesity [17]. Although
all conclude that the Glittre-ADL test may be useful
in clinical practice to quantify functional capacity and functional capacity to
exercise in these populations, only Karloh et al.
[15] have compared their results with direct VO2max
measurement.
The study
conducted by Reis et al. [13] evaluated the Glittre-ADL
test total performance time in a sample of healthy adult subjects and found
that the mean time to finish the test was 2.62 ± 0.34 min. In the present
study, the time was 3.44 ± 0.54 min. The longer time demanded by patients with
OSA for completing the test can be attributed to the systemic repercussions
caused by reoccurring episodes of hypoxia/reoxygenation present in the disease.
The presence of associated comorbidities such as hypertension and diabetes which
may also limit performance on tests that assess functional exercise capacity
should also be evaluated. Silva et al. [21] determinated
the validity and the reliability of the Glittre-ADL
in subjects with Parkinson disease and observed that the time to execute the Glittre-ADL test was 3.69 min (2.96-4.48 min).
In this study,
the HRmax obtained during the Glittre-ADL test was
130.6 ± 13.3 bpm, which corresponds to 80.9 ± 6.9% of the HRmax observed on the
CPET, characterizing the Glittre-ADL test as a submaximal
test in our sample. The evaluation of the exercise tolerance in clinical
settings is related to the test type choice. Submaximal tests are low-cost,
simple to apply, and it is possible to perform them in regular facilities with
easy access to the professional and the patient who needs to perform it, thus
better representing the daily activities of the individual [22]. In addition,
OSA is a disease commonly associated with cardiovascular comorbidities that may
hinder the performance of maximal stress testing by these patients. Thus,
submaximal exertion tests appear as a safe alternative for data collection for
exercise prescription and follow-up of the evolution in these patients.
Regarding the
hemodynamic responses of the Glittre-ADL test in the
present study, we can consider that the test promoted a submaximal
physiological stress, since systolic (SBP) and diastolic blood pressure (DBP)
were moderately elevated during the recovery period. Evaluating subjects with
OSA submitted to CPET, Hargens et al. [23]
found higher values of systolic (196.9 ± 7.0 mmHg) and diastolic (90.7 ± 3.1
mmHg) blood pressure in the recovery period due to the maximum characteristic
of the applied test. In our study, the performance of a submaximal test such as
the Glittre-ADL test led to milder SBP and DBP values
in the recovery period.
Other submaximal
tests have already been used to assess exercise tolerance in subjects with OSA
[24,25,26]. Billings et al. [27] used the incremental shuttle walk test
(ISWT) to determine exercise capacity in patients with moderate to severe OSA
treated with Continuous Positive Airway Pressure (CPAP). They concluded that
the ISWT is safe, well-tolerated and easy to apply in this population. Masa et
al. [28] used the 6MWT to assess exercise capacity in subjects with severe
OSA treated with CPAP for two months. Similarly, Goel et al. [29] also
used the 6MWT to assess exercise capacity in subjects with moderate and severe
OSA. Both studies using the 6MWT found that this test is indicated to assess
functional capacity in individuals with OSA, requiring few resources and
without significant risks to the participants.
The present
study showed high reliability and excellent agreement between the measurements
of the two performed Glittre-ADL tests. When
comparing the total test time of both tests, no differences were observed
between them, demonstrating that there was no learning effect, and therefore
there is only the need to perform a single test for the clinical practice. A
study carried out by Santos et al. [30] in patients with chronic
obstructive pulmonary disease (COPD) presented similar results with an ICC of
0.97, also indicating high reliability between the measurements. Also, Reis et
al. [13] evaluated the Glittre-ADL total time in
a sample composed of healthy adults and found an ICC of 0.88 (p < 0.05)
between the times of the two Glittre-ADL
measurements, corroborating the results obtained in our study.
Clinical implications
Submaximal field
tests are a widely used option in daily clinical practice for the evaluation of
exercise capacity. This type of test allows for an efficient and simpler
approach, requiring fewer resources when compared to maximum effort tests. They
can be performed in any environment with the available space, making it
possible to evaluate and obtain data for exercise prescription. In addition to
its easy reproduction, the Glittre-ADL test has been
used due to being able to efficiently evaluate efforts, generating lower
cardiovascular physiological stress, but enough so that we can get an adequate
evaluation of the submaximal functional capacity of exercise for individuals
with OSA.
In this context,
the Glittre-ADL test is an interesting and viable
option for assessing exercise tolerance in OSA valid, independent of the
associated comorbidities. This kind of test promotes less physiological stress
and therefore, can be considered safe and not overloading the subjects.
Limitations of the study
The limitations
of the present study include the absence of subjects with mild OSA, as the
study just included patients with moderate and severe OSA. Mild sleep apnea
patients could have less effects of hypoxia and the adverse impact on the
cardiovascular system and in exercise tolerance of these patients with a low
AHI may be less pronounced.
Conclusion
Therefore,
according to the results of the present study, the Glittre-ADL
test shows concurrent validity and excellent intrarater
reliability in OSA patients.
Conflict of interest
No conflict of interest
with relevant potential.
Financing source
This study was financed
in part by the Coordenação de Aperfeiçoamento
de Pessoal de Nível
Superior – Brasil (CAPES) – Finance Code 001.
Author’s contributions
Conception and design
of study: Lima AMJ. Acquisition, analysis and/or interpretation of data: Souza,
AKF, Aguiar MIR, Nóbrega-Júnior JCN; Lima AMJ, Brasileiro-Santos MS; Drafting the manuscript: Nóbrega-Júnior JCN, Lima AMJ; Revising the manuscript
critically for important intellectual content: Pedrosa RP, Andrade AD, Brasileiro-Santos, MS.
References
- Patel SR. Obstructive sleep apnea. Ann Intern Med
2019;171(11):ITC81-ITC96. doi: 10.7326/AITC201912030 [Crossref]
- Sauleda J, Garcia-Palmer FJ, Tarraga S, Maimo A, Palou A, Augusti AGN. Skeletal Muscle changes in patients with obstructive sleep apnoea syndrome. Respir Med 2006;97(7):806-10. doi: 10.1016/S0954-6111(03)00034-9 [Crossref]
- Rundo JV. Obstructive sleep apnea basics. Cleve Clin J Med 2019;86(9Suppl1):2-9. doi: 10.3949/ccjm.86.s1.02 [Crossref]
- Marillier M, Gruet M, Baillieul S, Wuyam B, Tamisier R, Levy P et al.s. Impaired erebral oxygenation and exercise tolerance in patients with severe obstructive sleep apnea syndrome. Sleep Med 2018;51:37-46. doi: 10.1016/j.sleep.2018.06.013 [Crossref]
- Berger M, Kline CE, Cepeda FX, Rizzi CF, Chapelle C, Laporte S, et al. Does obstructive sleep apnea affect exercise capacity and the hemodynamic response to exercise? An individual patient data and aggregate meta-analysis. Sleep Med Rev 2019;45:42-53. doi: 10.1016/j.smrv.2019.03.002 [Crossref]
- Vitacca M, Paneroni M, Braghiroli A, Balbi B, Aliani M, Guido P, et al. Exercise capacity and comorbidities in patients with obstructive sleep apnea. J Clin Sleep Med 2020;16(4):531-38. doi: 10.5664/jcsm.8258 [Crossref]
- Chien MY, Wu YT, Lee PL, Chang YJ, Yang PC. Inspiratory muscle disfunction in patients with severe obstructive sleep apnoea. Eur Respir J 2010;35(2):373-80. doi: 10.1183/09031936.00190208 [Crossref]
- Van Offenwert E, Vrijsen B, Belge C, Troosters T, Buyse B, Testelmans D. Physical activity and exercise in obstructive
sleep apnea. Acta Clin Belg 2019;74(2):92-101. doi: /10.1080/17843286.2018.1467587 [Crossref]
- Sant´Ana LO, Scartoni FR, Portilho LF, Scudese E, Oliveira CQ, Senna GW. Comparação das variáveis cardiovasculares em idosos ativos em diferentes modalidades físicas. Rev Bras Fisiol Exerc 2019;18(4):186-94. doi: 10.33233/rbfe.v18i4.3232 [Crossref]
- American Thoracic Society, American college of chest physicians ATS/ACCP Statement on cardiopulmonary exercise testing. Am J Respir Crit Care Med 2003; 167(2): 211-77. doi: 10.1164/rccm.167.2.211 [Crossref]
- Andrade
CHSD, Cianci R, Malaguti C, Dal Corso S. O uso de
testes do degrau para a avaliação da capacidade de exercício em pacientes com
doenças pulmonares crônicas. J Bras Pneumol 2012;38(1):116-24. doi: 10.1590/S1806-37132012000100016 [Crossref]
- Pessoa
BV, Jamami M, Basso RP, Regueiro EMG, Di Lorenzo VAP,
Costa D. Teste do degrau e teste da cadeira: comportamento das respostas metábolo-ventilatórias e cardiovasculares na DPOC. Fisioter Mov
2012;25(1):105-15. http://doi.org/10.1590/S0103-51502012000100011 [Crossref]
- Reis
CM, Silva TC, Karloh M, Araujo
CLP, Gulart AA, Mayer AF. Performance of
healthy adult subjects in Glittre ADL-test. Fisioter Pesqui
2015;22(1):41-7. http://doi.org/10.590/1809-2950/13125722012015 [Crossref]
- Corrêa
KS, Karloh M, Martins LQ, Dos Santos K, Mayer AF. O
Teste de AVD-Glittre é capaz de diferenciar a
capacidade funcional de indivíduos com DPOC da de saudáveis? Rev
Bras Fisioter
2011;15(6):467-73. doi: 10.1590/S1413-35552011005000034 [Crossref]
- Karloh M, Karsten M, Pissaia FV, Araujo
CLP, Mayer AF. Physiological responses to the Glittre-ADL
test in patients with cronic obstructive pulmonar disease. J
Rehabil Med 2014;46:88-94. doi: 10.2340/16501977-1217 [Crossref]
- Valadares
YD, Correa KS, Silva BO, Araujo CCP, Karloh M, Mayer AF. Aplicabilidade de testes de atividade
de vida diária em indivíduos com insuficiência cardíaca. Rev
Bras Med Esporte
2011;17(5):310-14. doi: 10.1590/S1517-86922011000500003 [Crossref]
- Monteiro F, Ponce DA, Silva H, Carrilho
AF, Pitta F. Validity and reliability of the Glittre
ADL-Test in obese and post-bariatric surgery patients. Obes Surg
2017;27(1):110-14. doi: 10.1007/s11695-016-2244-7 [Crossref]
- Silva
OB, Filho DC. A new proposal to guide velocity and inclination in
the ramp protocol for treadmill ergometer. Arq Bras Cardiol 2003;81:48-53. doi: 10.1590/S0066-782X2003000900004 [Crossref]
- Skumlien S, Hagelund T, Bjortuft O, Ryg MA. Field test of functional status as performance of
activities of daily living in CODP patients. Respir Med 2006;100:316-23. doi: 10.1016/j.rmed.2005.04.022 [Crossref]
- Tanaka H, Monahan KD, Seals DR. Age-predicted maximal
heart rate revisited. J Am
Coll Cardiol
2001;37(1):153-6. doi: 10.1016/S0735-1097(00)01054-8
- Silva D, Corrêa J, Sá M, Normando V, Silva SM., Dal Corso S, et al. Validation and reproducibility of the Glittre activities of daily living test for individuals with Parkinson's disease. Rev Neurol 2019;69(10):395-401. doi: 10.33588/rn.6910.2019217 [Crossref]
- Arena R, Myers J, Williams MA, Gulati M, Kligfield P, Balady GJ, et al.
Assessment of functional capacity in clinical and research settings: A
scientific statement from the American Heart Association Committee on Exercise,
Rehabilitation and Prevention of the council on clinical cardiology and the
council on cardiovascular nursing. Circulation 2007;116:329-63. doi: 10.1161/CIRCULATIONAHA.106.184461 [Crossref]
- Hargens TA, Guill SG, Zedalis D, Gregg JM, Nickols-Richardson SM, Herbert WG. Attenuated heart rate
recovery following exercise testing in overweight young men with untreated
obstructive sleep apnea. Sleep
2008;31(1):104-10. doi: 10.1093/sleep/31.1.104 [Crossref]
- Pływaczewski R, Stokłosa A, Bieleń P, Bednarek M, Czerniawska J, Jonczak, et al.
Six-minute walk test in obstructive sleep apnoea. Pneumonol Alergol Pol 2008;76:75-82.
- Rami K, William A, Patt B,
Roy M, Keding H, Jarjoura D. Cardiac effects of continuous
and bilevel positive airway pressure for patients with heart failure and
obstructive sleep apnea. Chest
2009;134(6):1162-8. doi: 10.1378/chest.08-0346 [Crossref]
- Abdelghani A, Ben Saad H, Ben Hassen I, Ghannouchi I, Ghrairi H, Bougmiza I e cols. Evaluation
of the deficiency and the submaximal exercise capacity in obstructive sleep
apnea patients. Rev Mal Respir 2010;27:266-74. doi: 10.1016/j.rmr.2010.02.004 [Crossref]
- Billings CG, Aung T, Renshaw SA., Bianchi SM. Incremental shuttle walk test in the assessment of patients with obstructive sleep apnea-hypopnea syndrome. J Sleep Res 2013;22:471-7. doi: 10.1111/jsr.12037 [Crossref]
- Masa
JF, Corral J, Caballero C, Barrot E, Terán-Santos J, Alonso-Álvarez ML, et al. Non-invasive
ventilation in obesity hypoventilation syndrome without severe obstructive
sleep apnoea. Thorax
2016;71(10):899-906. doi: 10.1136/thoraxjnl-2016-208501 [Crossref]
- Goel AK, Talwar D, Jain SK. Evaluation of short-term
use of nocturnal nasal continuous positive airway pressure for a clinical
profile and exercise capacity in adult patients with obstructive sleep
apnea-hypopnea syndrome. Lung India 2015;32:225-32. doi: 10.4103%2F0970-2113.156226 [Crossref]
- Santos K, Gulart AA, Munari AB, Cani KC, Mayer AF. Reliability of ventilatory parameters, dynamic hyperinflation, and performance in the Glittre-ADL test in COPD patients. COPD J Chronic Obstr Pulm Dis 2016;13(6):700-5. doi: 10.1080/15412555.2016.1177007 [Crossref]