Rev Bras Fisiol Exerc 2022;21(1):15-25
doi: 10.33233/rbfex.v21i1.4270
ORIGINAL ARTICLE
Strength training: the agreement between methodological standards and
prescription by fitness professionals
Treinamento da força
muscular: concordância entre os padrões metodológicos e a prescrição por
profissionais do fitness
Francys Paula Cantieri1, Gustavo
Aires de Arruda1, Diogo Henrique Constantino Coledam2, Antonio Carlos Gomes3, Ágata Cristina Marques
Aranha4, Mauro Virgilio Gomes de Barros1,
Marzo E. da Silva Grigoletto5
1Universidade de Pernambuco, Recife, PE, Brazil
2Instituto Federal de Educação, Ciência e
Tecnologia de São Paulo, São Paulo, SP, Brazil
3Instituto Olimpico
Brasileiro, Rio de Janeiro, RJ, Brazil
4Universidade Trás-dos-Montes
e Alto Douro, Vila Real, Portugal
5Universidade Federal de Sergipe,
Aracaju, SE, Brazil
Received: March 30, 2021; Accepted: November 5, 2021.
Correspondence: Francys Paula Cantieri, Rua Olavo
Bilac, 72/1204, 51021480 Recife PE
Francys Paula Cantieri:
francyspaulapersonal@gmail.com
Gustavo
Aires de Arruda: arrudaga@yahoo.com.br
Diogo
Henrique Constantino Coledam: diogohcc@yahoo.com.br
Antonio Carlos Gomes:
contatoacgomes@gmail.com
Ágata
Cristina Marques Aranha: aaranha@utad.pt
Mauro Virgilio Gomes de Barros: mauro.barros@upe.br
Marzo Edir
da Silva Grigoletto: marzogrigoletto@gmail.com
Abstract
Introduction: The scientific advances have resulted in proposed
methodologic standards to assist the prescription of physical exercise, but it
is not clear whether there is a practical application of these standards by
fitness professionals. Objective: To analyze the agreement between the
methodologic standard for strength training and the methodology used by the
fitness professionals. Methods: 461 professionals (men = 68.1%), aged
31.3 (± 6.8) years old, from the city of Londrina/PR and São Paulo/SP participated
in the study, who filled out a questionaire
containing 16 objective questions about strength training methodology. The
Binomial test (cutoffs: 50% and 70%) was used for statistical analysis (p <
0.05). Results: Agreement significantly greater than 70% was obtained
for 37.5% of the questions when considering agreement greater than 50%, plus
12.5% of the questions were added. Agreements significantly less than 50% were
identified for the number of repetitions for local muscle endurance (33.5%),
load percentage for muscle power (39.5%), as well as for the rest interval for
local muscle endurance (19.3%), hypertrophy (33.8%) and muscle power (20.3%). Conclusion:
In general, the prescriptions indicated by fitness professionals had low
agreement with the analyzed methodologic standards.
Keywords: resistance training; exercise; practice guidelines;
physical fitness; health.
Resumo
Introdução:
Avanços científicos resultaram em
padrões metodológicos propostos para auxiliar na
prescrição do exercício
físico, porém ainda não está claro se
há aplicação prática de tais padrões
por
profissionais do fitness. Objetivo: Analisar a concordância entre
padrões metodológicos para treinamento de força muscular e a metodologia
utilizada por profissionais que atuam na área do fitness. Métodos:
Participaram do estudo 461 profissionais (homens = 68,1%) com média de 31,3 (±
6,8) anos da cidade de Londrina/PR e São Paulo/SP, que preencheram um
questionário contendo 16 questões objetivas sobre metodologia do treinamento de
força. O teste Binomial (cutoffs: 50% e 70%) foi
utilizado para as análises estatísticas (p < 0,05). Resultados:
Concordância significativamente maior que 70% foi obtida para 37,5% das
questões. Ao considerar concordância maior que 50% mais 12,5% das questões foram
adicionadas. Concordâncias significativamente inferiores a 50% foram
identificadas para o número de repetições para a resistência muscular
localizada (33,5%), percentual de carga para potência (39,5%), bem como para o
intervalo de recuperação para resistência muscular localizada (19,3%),
hipertrofia (33,8%) e potência (20,3%). Conclusão: A prescrição apontada
pelos profissionais que atuam com fitness em geral apresentou baixa
concordância com os padrões metodológicos analisados.
Palavras-chave: treinamento resistido; exercício;
diretrizes práticas; aptidão física; saúde.
Introduction
The popularization of strength training stimulated the
investigation of this phenomenon to identify its health benefits, as well as
its applicability in the prevention and treatment of degenerative diseases
related to physical inactivity [1,2]. Scientific evidence has pointed out many
possible health benefits of strength training to different population groups at
various stages of life. Among these effects are increase resting metabolic rate
and a decrease of low-density lipoprotein [3], post-exercise hypotension [4],
benefits in the neuromuscular system [5,6] along cognitive and mental health
aspects [7].
In 2007, the descriptor “muscle strength” was
introduced in the National Library of Medical Subject Headings and defined as
the amount of force generated by muscle contraction. Stimuli of different
magnitudes applied to the muscular system through strength training promote
distinct functional and morphological adaptations in the body [8,9]. Therefore,
the prescription process must be based on the aspect of the neuromuscular
activity specificity, the percentage of musculature involved in the action, the
type of fiber, muscle work and motor necessity [10,11].
The total training intensity is represented as the
product of the total number of sets and repetitions performed in one session
multiplied by the load used in each repetition [12,13] and directly depends on
the rest interval adopted between the sets.
Muscle adaptations depend both on the type of program
used and the manipulation of total training intensity [1,9,10,14]. It can alter
the final result in the maximal muscle strength (MS) which could be described
as the increase in the capacity to generate strength against maximum
resistance, in muscle hypertrophy (MH) represented by an increase in muscle
volume, local muscle endurance (ME) characterized by higher resistance to
fatigue during prolonged efforts, as well as muscle power (MP) that could be
defined as the ability of the neuromuscular system to overcome resistance by
applying high contraction speeds [1,10,12,15,16].
Although there is the understanding that professional
practice is guided by scientific knowledge acquired during academic training
[17], there seem to be divergences between methodologic standards and the
practical application of professionals. The knowledge of professionals about
such guidelines was previously investigated [18,19]; however, to the best of
our knowledge, there are no studies that verify the agreement between the
scientific standards and professional practice. This information can contribute
to professional practices, just like in the curriculum reformulation of higher
education courses.
In this perspective, the present study aimed to
analyze the agreement between the methodologic standards for muscle strength
training and the methodology used by the fitness professional.
Methods
This is an observational study with a cross-sectional
design as part of a larger project with data collected in 2014 over two months.
All participants signed the consent form, and the study protocol was approved
by the Human Research Ethics Committee No: 1.013.727.
Participants
The sample consisted of 461 Physical Education
professionals who attend postgraduate courses in Londrina/PR or São Paulo/SP.
Only professionals enrolled in the Federal Council of
Physical Education (CONFEF) were included in the study. Those who did not
answer all of the instrument's questions regarding strength training or
indicated more than one alternative for the same question were excluded from
the analysis.
Instrument
A questionnaire was specifically constructed for this
study containing 46 objective questions with six alternatives for each question
[20]. For this study, were used 16 questions comprising aspects such as
training method, motor performance, and exercise volume and intensity variables
related to strength training variables, as described in chart 1.
Chart 1 - Questions related to strength training variables
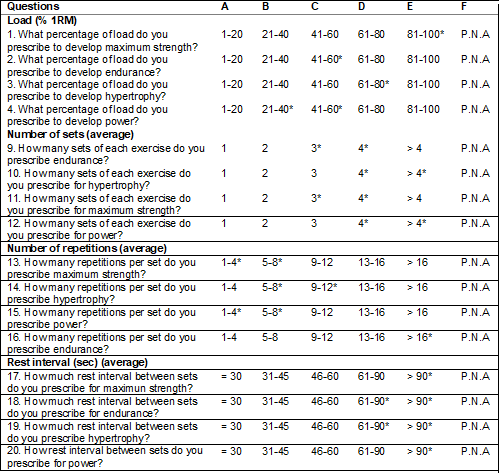
P.N.A = I prefer not to answer; *the alternative
considered to be in accordance with the standard
The instrument had acceptable test-retest reliability
by Kappa test (fair to good), and Cronbach’s Alpha was 0.8, the questions used
were just those related to muscle strength training.
To respond to the objective of the present study and
considering a large amount of information available regarding the prescription
of strength training, it was decided to adopt the training standard described
by scientific studies with international recognition for each strength training
variable, as described in chart 2.
Chart 2 - Description of the scientific training standard
used as criteria for analysis of strength training

Adapted from: Garber et al. [1]; Ratamess et al. [9]; Schoenfeld et al. [10]; Verkhoshansky and Stiff [11]; Fleck and Kraemer [12];
Krieger [13]; Bird et al. [15]; Schoenfeld et al. [16]; Perterson et al. [21]; Schoenfeld et al. [23];
Kraemer and Ratamess [24]; Wernbom
et al. [26]; Grgic et al. [27]; Bottaro et al. [28]; Hill-Haas et al. [29]
Procedures
All participants were instructed to answer all
questions in the questionnaire, indicating only one of the options and, in case
of doubt, when not solved, choose the option “Prefer not to answer” (P.N.A).
The collection was carried out in predetermined dates and times, during the
intervals of the specialization classes and under the supervision of the
researcher responsible for the study. No clarification on methodological doubts
was provided to the participants also were not allowed consultations with
specialized literature, or search sites.
The data were analyzed using measures of frequency for
the 16 questions. For dichotomized questions, the confidence intervals of 95%
for frequencies were performed with Bootstrap (1000 samples). The binomial test
was used to verify if the proportion of participants who agreed or disagreed
with the methodologic standards was significantly different (proportion 50%).
Considering that 70% is an acceptable cutoff in several evaluation
institutions, binomial tests were used to identify whether the proportion of
professionals who agree with the methodologic standards differs significantly
from these criteria [21]. The variables percentual of load (%), number of sets
and repetitions and rest intervals between sets were analyzed for all types of
strength. The level of significance adopted was p < 0.05. All analyses were
performed with IBM SPSS Statistics for Windows, version 20 (IBM Corp., Armonk,
N.Y., USA).
Results
The sample consisted of 314 men with an average age of
31.1 (± 6.6) years and 147 women with an average age of 31.4 (± 6.9) years.
Concerning the MS, a higher percentage of respondents
opted for loads between 81 and 100% of 1RM, 3 sets, between 1 to 4 repetitions
per set and adopted rest intervals above 90 seconds. For ME prescription, the
majority opted for loads between 41 to 60% of 1RM, 3 series, between 13 to 16
repetitions and indicated between 31 to 45 seconds of the rest interval. The
prescription aiming at MH presented a higher frequency for percentages of loads
between 61 to 80, most use 4 sets, between 9 to 12 and rest interval varying
from 46 to 60 seconds. Finally, for MP, most participants prescribed loads
between 61 to 80% of 1RM, adopted 4 sets, with repetitions between 5 to 8 and a
rest interval of 45 to 60 seconds (Table I).
In general, using the cutoff of 70% the MH presented
the highest number of questions that showed significant agreement with three
questions (75%) and a lower number of questions were found for ME and MP, both
with just one question (25%). Considering the analysis by variables, the one
with the highest number of questions that agree was the number of sets (75%)
and the lowest was the rest interval, which did not present any question with a
significant agreement (Table II).
From the cutoff of 50%, the MS was the variable with
the highest number of agreement questions (100%) and the lowest number found
for MP (25%). Considering only the variables of strength training, the number
of sets showed 100% agreement of the questions and the rest interval was the
one with the lowest number of agreement questions (25%) (Table II).
Table I - Frequency of responses in training variables
(load, number of sets, number of repetitions, and rest interval) in the
different strength training
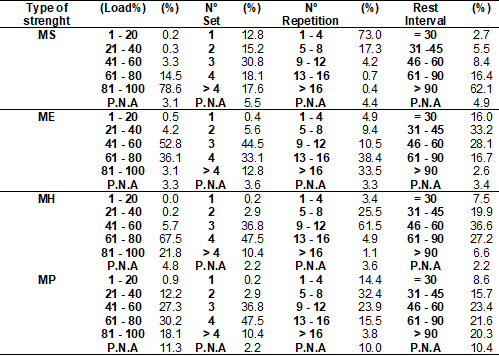
MS = maximal muscular strength; ME = endurance; MH =
hypertrophy; MP = power; P.N.A = I Prefer not to answer
Table II - Agreement between methodological scientific
training standard for strength training prescription and fitness professionals’
practice
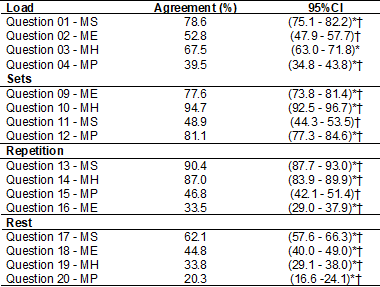
*Significantly different (p < 0.05) from desagree by Binomial test (proportion 50%); † Significantly
different (p < 0.05) from reference cutoff (proportion 70%) by Binomial
test. MS = maximal muscular strength; ME = endurance; MH = hypertrophy; MP =
power
Based on the results obtained by the binomial
analysis, the proportion of agreement was significantly higher than 50% on the
following questions: 1 and 3, related to (% of load MS and MH) 9, 10, 12, (sets
ME, MH, MP respectively) 13 and 14 (repetitions MS and MH) and 17 (rest MS).
Questions 2 (% load ME), 11 (sets MS) and 15 (repetitions MP) had similar
proportions of agreement and disagreement. The proportion of agreement for
questions 4 (% of load MP), 16 (repetitions ME), 18, 19 and 20 (rest ME, MH, MP
respectively) was significantly less than 50%. Using the 70% cutoff point, it
was observed that 37.5% of the questions agree with the standards, they are,
questions 1 (% of load MS), 9, 10,12 (sets ME, MH, MP respectively), 13 and 14
(repetitions MS and MH). Questions 2 and 4 (% of load ME and MP), 11 (sets MS),
15 and 16 (repetitions MP and ME), 17, 18, 19 and 20 (rest MS, ME, MH, MP) were
significantly below the cutoff point and only question 3 (% of load MH) it did
not differ significantly from 70% agreement (table II).
Discussion
Professionals, in general, do not prescribe strength
training according to scientific recommendations. A relevant proportion of
questions showed agreement below the minimum cut-off point adopted. Considering
the type of adaptation, muscle hypertrophy was the training that showed the
highest agreement, while the muscle power training was the one that showed the
lowest agreement with the scientific training standards. When observing the
training variables regardless of the type of training, the one with the highest
number of concordance questions was the number of series and the rest interval
was the variable that showed the least agreement with methodologic standards.
Although there is no cut-off point established in the
literature regarding the agreement between the prescription adopted by the
professionals and the scientific recommendations because it is not objectively
an assessment of the knowledge, it was expected that most professionals would
answer the questions in a manner corresponding to the methodologic standard.
Studies suggest that MS training should prioritize
loads close to maximum capacity, with a number of average sets, reduced number
of repetitions and intervals above 90 seconds, to promote neural adaptations
with increased recruitment of motor units and optimization of intramuscular
coordination [9,11,12,22,23,24]. In the present study, all questions related to
the variables of the training of MS presented agreement greater than 50%, with
emphasis on the percentage of load and number of repetitions that exceeded 70%
of agreement.
Considering the ME, only two of the four variables
analyzed had an agreement greater than 50% and only the number of sets exceeded
the cutoff point of 70%. In general, it was expected that, if not all, most
variables would obtain an agreement greater than 70%, since the literature
indicates the development of ME in all areas of physical exercise, due to its
relevance in maintaining the parameters health of individuals, as well as in
the general phases of sports training, due to its preparatory nature for the
development of other types of specific training. The low agreement observed
evidence the need for future studies that aim to diagnose the importance
attributed by professionals to the development of endurance for health and
sports performance and the frequency with which these prescriptions are carried
out.
It is essential to highlight the high percentage of
professionals who opted for the number of repetitions between 1 and 12, and a
rest interval below the recommended. The training aimed at increasing local
muscle endurance requires a high number of repetitions with not too long
intervals, which allow partial recovery of energy substrates and promote an
increase in mitochondrial and capillary numbers, fiber type transitions and
buffer capacity [1,12,15,25]. The portion of professionals who opted for very
short intervals may be referring to circuit training, however, the
recommendation for this type of prescription suggests lower loads than those
indicated by professionals [12].
The scientific literature advises that training aimed
at hypertrophy should be programmed with loads between 60 to 80% of maximum
capacity, with a number of sets greater than 3 and repetitions ranging from 5
to 12, with rest intervals above 60 seconds. Three of the four questions,
percentage of load, number of sets and repetitions related to MH were in
accordance with the standard above 70% [1,9,11,13,26], with only the question
regarding the agreement rest interval being presented below 50%. This high
agreement observed between professionals' prescriptions and scientific
recommendations can be justified by the fact that it is a training modality
widely used among professionals both for health promotion and sports
performance. In addition, the preference of practitioners for stronger and
muscle definition can lead professionals working with fitness to prioritize
this type of prescription. This interest observed in practice is reflected by
the high number of scientific papers published annually on the subject.
It was expected that the rest interval would also show
an agreement greater than 70%, since the adequate rest interval is essential
for the good development of muscle hypertrophy. Results indicate that intervals
longer than 60 seconds allow the energetic substrates to be adequately replaced
in the muscle in action [1,12,27,28,29,30] and shorter intervals can generate early
fatigue and impair the performance of subsequent series and not allow
significant gains in hypertrophy [29,30]. However, in the present study, these
standards were adopted by less than 40% of professionals.
When analyzing the prescription for the development of
MP, only the question regarding the number of sets had an agreement greater
than 70%. The questions related to the percentage of load and rest interval
were below 50% of the scientific recommendations. The MP occurs when a greater
number of movements is performed in a certain period of execution or when the
same number of movements is performed in a shorter period [11]. In this sense,
the recommendation for the development of MP involves moderate loads not
exceeding 60% of 1RM with a rest interval similar to those proposed to develop
maximum strength (≥ 90 seconds) allowing adequate replacement of muscle phosphogen [1,9,11,12].
The development of MP through traditional training has
good results, however, the current literature proposes other alternatives as
efficient forms of training that were not included in this questionnaire, such
as plyometrics. In addition, strength training is generally related to sports
performance and most professionals who took part in this study develop physical
fitness programs focused on health. These particularities related to MP
training may explain the low agreement observed in most of the analyzed
variables.
The low agreement observed in the present study
between the prescription of variables that make up a strength training program
and scientific recommendations is worrying, since such recommendations,
proposed with a high level of scientific evidence, seem to be neglected by most
fitness professionals.
The exponential increase in the number of university
students in physical education courses observed in recent decades and the low
rate of failure, associated with the curricular contents of academic training
that do not include every phenomenon observed in practice, can influence the
prescription made by professionals. The absence of a single guideline can make
the process of professional training difficult, as it does not allow for
adequate preparation for evidence-based decision-making. On the other hand, the
ease of access to content through digital platforms, which in some cases
disclose information with low scientific rigor, can influence professionals in
their decisions.
In the present study, only one component of the
training was evaluated, however, it should be considered that its prescription
occurs concomitantly with the other components of physical fitness. In
addition, the form of prescription was analyzed through a questionnaire, not
allowing to verify its applicability in the real context. However, the use of
this type of instrument allows the analysis of large samples.
Regarding the choice of the 70% cutoff point, it may
not indicate an ideal proportion of agreement in all contexts, but it is a
reference widely used in several academic evaluation processes, as the minimum
acceptable. Another aspect to be considered is that the present study may not
represent the level of knowledge of Brazilian professionals, since the
professionals who participated in the research were already at a postgraduate
training level. Finally, it was not evaluated whether the 1RM load was obtained
using any specific tests or by predictive equations.
Conclusion
A low agreement was observed between the professional
prescription and the training standards proposed in the scientific literature.
Muscle hypertrophy was the training that showed the highest agreement, while
endurance and power training were the ones that least agreed with the
recommendations. When considering the training variables regardless of the type
of training, the one with the highest number of concordant questions was the
number of sets and the rest interval was the variable that showed the least
agreement with the methodologic standards.
Acknowledgment
National Postdoctoral Program of CAPES (PNPD/CAPES)
and Foundation for Science and Technology Support from Pernambuco (FACEPE).
Potential conflict of interest
No conflicts of interest with potential potential for this article have been reported
Financing source
There were no external sources of funding for this
study.
Authors’ contributions
Conception and research design: Cantieri
FP, Gomes AC, Aranha ACM; Obtaining data: Cantieri FP, Arruda GA; Data analysis and interpretation: Cantieri FP, Arruda GA, Aranha
ACM, Coledam DHC; Writing of the manuscript: Cantieri FP, Arruda GA, Coledam
DHC, Gomes AC, Barros MVG, Silva-Grigoletto ME.
Statistical analysis: Arruda GA, Gomes AC, Barros MVG; Critical revision of the
manuscript for important intellectual content: Silva- Grigoletto
ME, Barros MVG, Aranha ACM
References
- Garber CE, Blissmer B, Deschenes MR, Franklin
BA, Lamonte MJ, Lee I, et al. American College of Sports Medicine position stand.
Quantity and quality of exercise for developing and maintaining
cardiorespiratory, musculoskeletal, and neuromotor fitness in apparently
healthy adults: guidance for prescribing exercise. Med Sci Sports Exerc 2011;43;7:1334-59. doi: 10.1249/MSS.0b013e318213fefb [Crossref]
- Powell KE, King AC, Buchner DM, Campbell WW, DiPietro L, Erickson KI,
cols. The Scientific Foundation for the Physical Activity Guidelines for
Americans, 2nd Edition. Journal of Physical Activity and Health 2019;16:1-11. doi: 10.1123/jpah.2018-0618 [Crossref]
- Westcott WL. Resistance training is medicine: effects of strength training on health. Curr Sports Med Rep 2012;11(4):209-16. doi: 10.1249/JSR.0b013e31825dabb8 [Crossref]
- MacDonald HV, Johnson BT, Huedo-Medina TB, Livingston J, Forsyth KC, Kraemer WJ, et al. Dynamic resistance training as stand-alone antihypertensive lifestyle therapy: a meta-analysis. J Am Heart Assoc 2016;5(10):e003231. doi: 10.1161/ jaha.116.003231 [Crossref]
- Walker S, Santolamazza F., Kraemer WJ, Häkkinen K. Effects of prolonged hypertrophic resistance training on acute endocrine responses in young and older men. J Aging Phys Act 2015;23:230-6. doi: 10.1123/japa.2013-0029 [Crossref]
- Calle MC, Fernandez ML. Effects of resistance training on the inflammatory response. Nutrition Research and Practice 2010;4(4):259-69. doi: 10.4162/nrp.2010.4.4.259 [Crossref]
- O’Connor PJ, Herring MP, Caravalho A. Mental health benefits of strength training in adults. Am J Lifestyle Med 2010;4(5):377-96. doi: 10.1177/1559827610368771 [Crossref]
- Folland JP, Williams AG. The adaptations to strength training: Morphological and neurological contributions to increased strength. Sports Med 2007;37(2):145-68. doi: 10.2165/00007256-200737020-00004 [Crossref]
- Ratamess NA, Alvar BA, Evetoch TK, Housh TJ, Kibler WB, Kraemer WJ cols. Progression models in resistance training for healthy adults. American College of Sports Medicine 2009:687-780. doi: 10.1249/MSS.0b013e3181915670 [Crossref]
- Schoenfeld BJ, Grgic J, Ogborn D, Krieger JW. Strength and hypertrophy adaptations between low- vs. high-load resistance training. J Strength Cond Res 2017;31;12:3508-23. doi: 10.1519/jsc.0000000000002200 [Crossref]
- Verkhoshansky Y, Stiff MC. Supertraining 2009. 6th ed. Ed.Verkhoshansky.com
- Fleck SJ, Kraemer
WJ. Fundamentos do treinamento de força muscular. 4ª ed. Porto Alegre: Artmed;
2017.
- Krieger JW. Single vs. multiple sets of resistance exercise for muscle hypertrophy: a meta-analysis. J Strength Cond Res 2010;24;4:1150-9. doi: 10.1519/JSC.0b013e3181d4d436 [Crossref]
- Baz-Valle E, Schoenfeld BJ, Torres-Unda J, Santos-Concejero J, Balsalobre-Fernandez C. The effects of exercise variation in muscle thickness, maximal strength and motivation in resistance trained men. PLoS ONE 2019;14;12: e0226989. doi: 10.1371/journal.pone.0226989 [Crossref]
- Bird SP, Tarpenning KM, Marino FE. Designing resistance training programmes to enhance muscular fitness: A review of the acute programme variables. Sports Med 2005;35(10):841-51. doi: 10.2165/00007256-200535100-00002 [Crossref]
- Schoenfeld BJ, Vigotsky AD, Grgic J, Haun C, Contreras B, Delcastillo K, et al. Do the anatomical and physiological
properties of a muscle determine its adaptive response to different loading
protocols? Physiol Rep 2020;8(9):e14427. doi: 10.14814/phy2.14427 [Crossref]
- Verenguer RCG, Campanelli
JR, Kallas D, Freire ES, Costa FC. Mercado de trabalho em Educação Física:
significado da intervenção. Motriz
[Internet]. 2008 [cited 2022 Feb 8];14(4):452-61.
- Zenko Z, Ekkekakis P. Knowledge of exercise prescription guidelines among certified exercise professionals. J Strength Cond Res 2015;29;5:1422-32 doi: 10.1519/JSC.0000000000000771 [Crossref]
- Ceschini F, Figueira Junior A, Andrade EL de, Araújo TL, Rica, RL, Miranda, ML, et al. Nível de conhecimento dos profissionais de educação física sobre prescrição de exercício aeróbico e de resistência para idosos. Rev Bras Med Esporte 2018;24;6:465-470. doi: 10.1590/1517-869220182406188634 [Crossref]
- Cantieri FP, Gomes AC, Arruda GA, Coledam DHC, Ribeiro EAG, Barros MVG, Aranha ACM. Methodology of physical exercise: A proposal and reliability of a questionnaire for fitness professionals. Baltic Journal of Health and Physical Activity 2021;13(4). doi: 10.29359/BJHPA.13.4.01 [Crossref]
- Zieky MJ, Perie M, Livingston SA. Cutscores: a manual for setting standards of performance on educational and occupational tests book; Princeton, NJ: Educational Testing Service September 2008;230. doi: 10.1177/0013164413502037 [Crossref]
- Peterson MD, Rhea MR, Alvar BA. Applications of the dose-response for muscular strength development: a review of meta-analytic efficacy and reliability for designing training prescription. J Strength Cond Res 2005;19;4:950-8. doi: 10.1519/R-16874.1 [Crossref]
- Ronnestad BR, Egeland W, Kvamme NH, Refsnes PE, Kadi F. Raastad T. Dissimilar effects of one- and three-set strength training on strength and muscle mass gains in upper and lower body in untrained subjects. J Strength Cond Res 2007;21;1:157-63. doi: 10.1519/R-19895.1 [Crossref]
- Schoenfeld BJ, Wilson JM, Lowery RP, Krieger JW. Muscular adaptations in low- versus high-load resistance training: A meta-analysis, Eur J Sport Sci 2014;16;1:1-10. doi: 10.1080/17461391.2014.989922 [Crossref]
- Kraemer WJ, Ratamess NA. Fundamentals of resistance training: progression and exercise prescription. Med Sci Sports Exerc 2004;36(4):674-88. doi: 10.1249/01.mss.0000121945.36635.61 [Crossref]
- Lasevicius T, Ugrinowitsch C, Schoenfeld BJ, Roschel H, Tavares,LD, Souza EO, et al. Effects of different intensities of resistance training with equated volume load on muscle strength and hypertrophy. Eur J Sport Sci 2018;18(6):772-80. doi: 10.1080/17461391.2018.1450898 [Crossref]
- Wernbom M, Augustsson J. Thomee R. The influence of frequency, intensity, volume and mode of strength training on whole musclecross-sectional area in humans. Sports Med 2007;37;3:225-64. doi: 10.2165/00007256-200737030-00004 [Crossref]
- Grgic J, Schoenfeld BJ, Skrepnik M. Davies TB, Mikulic P. Effects of rest interval duration in resistance training on measures of muscular strength. Sports Med 2017;48;1:137-51 doi: 10.1007/s40279-017-0788-x [Crossref]
- Bottaro M, Martins B, Gentil P, Wagner D. Effects of rest duration between sets of resistance training on acute hormonal responses in trained women. J Sci Med Sport 2009;12:73-8. doi: 10.1016/j.jsams.2007.10.013 [Crossref]
- Hill-Haas S, Bishop D, Dawson B, Goodman C, Edge J. Effects of rest interval during high-repetition resistance training on strength, aerobic fitness, and repeated-sprint ability. J Sports Sci 2007;25;6:619-28. doi: 10.1080/02640410600874849 [Crossref]
