Rev Bras Fisiol Exerc 2021;20(6):665-76
doi: 10.33233/rbfex.v20i6.4338
ATUALIZAÇÃO
High-intensity
interval training: a brief review on the concept and different applications
Treinamento intervalado de alta intensidade:
uma breve revisão sobre o conceito e diferentes aplicações
Alexandre Lopes Evangelista¹, Cauê V. La Scala Teixeira²,
Leandro Henrique Albuquerque Brandão3,5, Alexandre F. Machado4,
Danilo Sales Bocalini4, Letícia Menezes Santos¹, Marzo
Edir Da Silva-Grigoletto3
1Universidade Nove de Julho, São Paulo, Brazil
2Instituto Valorize de Educação, Vila
Velha, ES, Brazil
3Functional Training Group
(FTG by UFS), Universidade Federal de Sergipe, São Cristovão, SE, Brazil
4Universidade Federal do Espírito Santo,
ES, Brazil
5Universidade Federal de Minas Gerais,
Belo Horizonte, MG, Brazil
Received: August 13, 2020; Accepted:
September 13, 2021.
Correspondence: Marzo Edir
Da Silva-Grigoletto, Rua Prof. Aricio
Guimarães Fortes, 321/902, 49037-060 Aracaju SE, Brazil
Alexandre Lopes
Evangelista: contato@alexandrelevangelista.com.br
Cauê V La Scala
Teixeira: contato@caueteixeira.com.br
Leandro Henrique
Albuquerque Brandão: leeo.henriquee01@gmail.com
Alexandre F Machado:
xdmachado@gmail.com
Danilo Sales Bocalini: bocaliniht@hotmail.com
Letícia Menezes Santos:
lemenezesss@gmail.com
Marzo Edir Da Silva-Grigoletto: medg@ufs.br
Abstract
Introduction: Due
to its highly dynamic characteristic and the time efficiency generated in
relation to other training methods, High Intensity Interval Training (HIIT) has
become a strategy used in different contexts. HIIT is understood as a training
method that intersperses periods of effort performed at high intensity with
periods of active (when an activity is performed at low intensity) or passive
(when no activity is performed) recovery. Based on this concept that does not
discriminate types of exercises, different HIIT models can be found in the
literature, such as classic HIIT, Sprint Interval Training (SIT), HIIT with
bodyweight, High Intensity Functional Training (HIFT), High Intensity Circuit
Training (HICT), and High Intensity Resistance Training (HIRT), expanding the
possibilities of applying HIIT to different purposes and audiences. Aim:
a) to revisit, through a brief update, the concept of HIIT and its different
aspects; b) present, from a scientific perspective, different protocols that
can be applied based on the concept of HIIT and its effects. Conclusion:
Based on the exposed concept and on the HIIT intensity control variables, this
approach can be applied to different training modalities. In addition, it can
be used as a strategy to provide safe and efficient training across different
populations.
Keywords:
physical exercise; performance; healthy; physical fitness; high intensity
interval training
Resumo
Introdução: Devido à sua característica altamente
dinâmica e à eficiência do tempo gerado em relação a outros métodos de treinamento,
o Treinamento Intervalo de Alta Intensidade (HIIT) tem se tornado uma
estratégia utilizada em diferentes contextos. O HIIT é entendido como um método
de treinamento que intercala períodos de esforço realizados em alta intensidade
com períodos de recuperação ativa (quando uma atividade é realizada em baixa
intensidade) ou passiva (quando nenhuma atividade é realizada). Partindo desse
conceito que não discrimina tipos de exercícios, diferentes modelos de HIIT
podem ser encontrados na literatura, como o HIIT clássico, Sprint Interval Training (SIT), HIIT com peso corporal,
Treinamento Funcional de Alta Intensidade (HIFT), Treinamento em Circuito de
Alta Intensidade (HICT), e Treinamento Resistido de Alta Intensidade (HIRT),
ampliando as possibilidades de aplicação do HIIT para diferentes finalidades e
públicos. Objetivo: a) revisitar, através de uma breve atualização, o
conceito de HIIT e seus diferentes aspectos; b) apresentar, do ponto de vista
científico, diferentes protocolos que podem ser aplicados com base no conceito
de HIIT e seus efeitos. Conclusão: Com base no conceito exposto e nas
variáveis de controle de intensidade HIIT, esta abordagem pode ser aplicada a
diferentes modalidades de treinamento. Além disso, pode ser usado como uma
estratégia para fornecer treinamento seguro e eficiente para diferentes
populações.
Palavras-chave: exercício físico; desempenho; saúde;
aptidão física, treinamento intervalado de alta intensidade.
Introduction
The
regular practice of physical exercise is associated with numerous benefits that
positively impact the quality of life and maintenance of functional capacity of
its practitioners [1]. The American College of Sports Medicine [2] recommends
that all adults engage in cardiorespiratory training, accumulating a minimum of
75 to 150 minutes per week of vigorous or moderate activity, respectively. If
the goal is weight loss and/or control, at least twice the weekly volume of
moderate-intensity physical activity (> 300 minutes) is suggested. Associated
with this, the collegiate also postulates that strength training should be
carried out around 2 to 3 times a week.
However,
in Brazil, the percentage of adults who reach the minimum volume recommended
for the weekly practice of physical activity is still a minority. In the 27
capitals, the frequency of reported physical activity equivalent to 150 minutes
of moderate activity per week in free time was only 39% [3]. The main reasons
for this, according to a study by Pinheiro et al. [4] include excessive working
hours and family commitments, in addition to a lack of company and interest in
practicing more traditional activities, such as weight training.
Thus,
more dynamic strategies and efficient training time may be attractive to many
people, which could help to increase not only the level of physical activity,
but also the adherence of practitioners in the long term [5,6]. Among these
strategies, high intensity interval training (HIIT) has been gaining
popularity, occupying a prominent position in the lists of current market
trends in Brazil [7] and worldwide [8]. The growth in the number of adepts is
associated with the possibility of training with few or no material resources
[9], training sessions with short duration [10], and a modality can be performed
outside the gym environment [11], offering advantages for individuals who do
not have much time to train [12].
Since
it was first proposed, HIIT has enabled athletes and different clinical
populations to enjoy the benefits caused by the accumulation of high intensity
exercise, a principle that guides HIIT, for long periods [13]. In this sense,
due to its high versatility and application possibilities, HIIT is used in
multifaceted ways [14], which can generate a conflict of concepts and difficulty
in controlling variables, both in research and in practice. Therefore, the
objectives of this study were: a) to revisit, through a brief update, the
concept of HIIT and its different applications; b) present, from a scientific
perspective, different HIIT protocols that can be applied based on the concept,
in addition to the effects related to each modality.
Definition of
high intensity interval training
High-intensity
interval training, by definition, is a method in which a high-intensity stimulus
(effort) period is interspersed with an active or passive recovery period [13].
This training proposal has been applied for many decades in different
populations and its use is justified, above all, by two facts: 1) the
possibility of simulating every day and/or sporting situations in which
intermittent effort is present (e.g., application of HIIT based on reduced
games, used in different types of team sports); 2) an increase in the time
(volume) of stimuli at higher intensities through the partial recovery of the
metabolic pathways, provided by the recovery intervals between each effort
period and between sets (series) of stimuli [13,15].
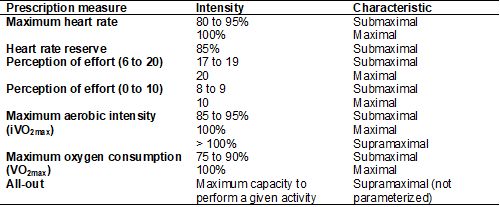
The
high intensity in this method is characterized by a level of effort that leads
different physiological systems to operate above some pre-established
thresholds [13], which have a submaximal, maximal, or supramaximal character.
Table I describes the prescription measures, intensity, and characteristic
rates by which popular protocols based on the HIIT concept are prescribed.
In
fact, intensity is a fundamental parameter for the prescription of HIIT, as it
is an important principle of the method [13]. However, this is not the only
dose control variable in HIIT. Buccheit and Laursen [16] describe nine variables related to stimulus
and recovery intervals in HIIT sessions: 1) intensity of effort; 2) duration of
effort; 3) intensity of recovery; 4) duration of recovery; 5) total duration of
the training session; 6) number of series; 7) type of exercise used; 8) duration
of series; and 9) interval between series, as well as environmental factors,
which are capable of altering acute and chronic responses [17,18].
Although
there are numerous manipulable parameters, in the
fitness context, the exercise modality in which HIIT is applied has been
significantly modified in different protocols [17,19,20,21]. Although it is not a
consensus, to our understanding, what characterizes HIIT is the magnitude of
effort in the stimulus intervals and not the modality (or type of exercise).
Considering this same perspective, different types of training and exercises
have been used to apply this proposal, which could expand the range of options
for training variation, as long as there is full knowledge of the
characteristics of each model.
Table I -
Parameters used in the prescription of interval training and characteristics
associated with the intensity rate
Based
on these parameters, HIIT has been performed through cyclic exercises
(pedaling, rowing, and running) [16], using calisthenics [22], strength [23],
and functional [20] exercises. When modifications are made in the modalities
used to perform HIIT, the way in which the intensity is monitored also changes,
since certain measures are inadequate for some exercises, which are often
performed in an "all out" manner on account due to the greater
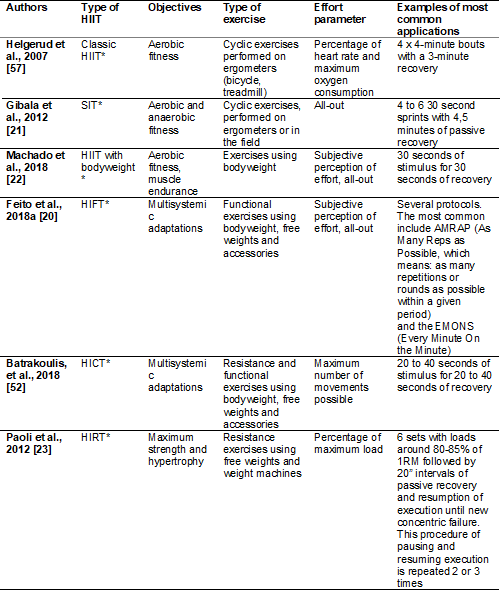
practicality and adequacy in controlling the intensity [19]. However, perceived
exertion is also a strategy used to prescribe HIIT in different exercise
modalities [13], and these models appear frequently in the scientific
literature, as described in table II.
Over
the years, HIIT has been shown to be an important training strategy to improve
performance, both for competitive athletes and for non-athletes, and it is very
effective in stimulating physiological adaptations, allowing for the
improvement of different components of physical fitness [24,25,26]. Although the
risk of musculoskeletal injury and cardiovascular events increases with higher
intensity exercise, HIIT performed as a component of sports training has
historically been associated with minimal risk [27]. Furthermore, this method
has been extensively studied in different specific groups, showing ample
safety, even in populations with different disorders [28] and during cardiac
rehabilitation [29].
Dun et
al. [30], in subjects who had suffered a myocardial infarction, suggested
that, when well supervised, HIIT may offer even more benefits than continuous
training of moderate intensity. In addition, although researchers continue to
assess the safety of HIIT, it appears that this training method can be
performed by people with a variety of health challenges. An HIIT prescription
model has also been suggested for populations with certain comorbidities, based
on different stimulus intervals and care that professionals should take before,
during, and after the session [31]. Therefore, application of this method is
recommended, as long as guidance and supervision (monitoring) are appropriate
[32,33,34].
Classic HIIT
Classic
HIIT is characterized by cyclical stimuli that can be performed through
activities such as running, cycling, swimming, or paddling. Regardless of the
modality in which it is performed, there are 2 traditional formats applied to
HIIT sessions [13]:
• Long intervals
HIIT: characterized by the performance of series of stimuli longer than 1
minute in duration (usually between 2 and 5 minutes) with intensity between 90%
and 100% of vVO2max (or higher) and passive (around 1 to 3 minutes
duration) or active recovery intervals (2 to 4 minutes of low intensity running
[< 65% vVO2max]).
• Short
intervals HIIT: characterized by the performance of series of stimuli between
10 and 60 seconds in duration with intensity >100% of vVO2max and
passive recovery intervals that obey the proportion varying between a shorter
recovery time in relation to work (1:0.5) and a longer recovery time in
relation to work (1:4) according to the intensity used.
Different
adaptations to HIIT have been demonstrated, including improvements in VO2max
parameters, anaerobic capacity, and physical performance [35]. These long-term
improvements are associated with central and peripheral readjustments resulting
from the high intensity provided by HIIT, improving cardiac output, and
peripheral vascular structure and function, including acceleration in
peripheral oxygen utilization, among other mechanisms that allow for increased
cardiometabolic health [36]. In addition, benefits also include decreased
insulin resistance [37], decreased body fat percentage [38], and reduced blood
pressure, with concomitant increases in strength in older adults [39].
Table II - Main
HIIT application models
Sprint interval
training
Sprint
interval training (SIT) is a method often used to improve sports activities in
different individual modalities [13]. The session consists of short stimuli of
supramaximal intensity that are not parameterized (all-out), which require a
great contribution from the anaerobic metabolism for energy supply [40].
Generally, the duration of each stimulus varies between 30 and 45 seconds, with
long recovery intervals (around 3 to 5 minutes or longer), performed passively
[16,21]. Stimuli with “all-out” intensity are understood as the maximum
capacity to perform a task of running, rowing, or pedaling on a non-motorized
treadmill or over ground [16].
SIT has been applied in different
populations with promising results related to health indicators, such as
increased cardiorespiratory fitness [24]. Although not parameterized, these
protocols can reach very high intensity values, which are closely related to
the increased activity of cell signaling pathways related to mitochondrial
biogenesis (increase in the number of mitochondria per cell) [33,41]. As a
result of this process, there is an increase in the lactate threshold, thus
allowing individuals to exercise for longer and at higher VO2max
percentages [41,42].
The
high intensity and non-parametrization of the stimuli are complicating factors
that can lead Physical Education professionals to insecurity about the use of
SIT in clinical populations. Because of this, it is suggested that further
studies be conducted to evidence safety and to establish recommendations on the
conduction and monitoring of complicating signals during the execution of
protocols with these characteristics in populations whose objective is to
improve general health.
HIIT with
bodyweight
Like
traditional HIIT, HIIT with bodyweight is also characterized by training
sessions with high intensity stimuli, followed by recovery periods that can be
passive or active, in which only bodyweight is used as resistance [11].
HIIT
studies using bodyweight adopt different nomenclatures, namely: whole-body
training [10], high-intensity intermittent calisthenic training [9], whole-body
High-intensity Interval Training [43], and HIIT body work [19,44].
The
relationship between stimulation time and session recovery can present 3
characteristics, being they: 1) the load ratio between the stimulus time and
the recovery time and 2) the exercises selected in the session. Didactically,
the exercises can be classified as simple, those that have a single movement
pattern (e.g., jumping jack), or complex, those with a combined movement
pattern (e.g., Burpee) [11].
The
session load ratio can present three distinct characteristics, namely: a)
stimulus time less than recovery time (2:1), b) stimulus time equal to recovery
time (1:1), and c) stimulus time greater than recovery time (2:1) [11].
Session
duration varies from ~4 to ~30 minutes [44] and intensity control is based on
the use of PSE, however the practitioner must be instructed to perform the
maximum number of repetitions of each exercise possible at the high interval
intensity, obeying previously established intensity criteria (RPE) [11].
In
one study [22], a significant reduction in body mass was observed in a group of
individuals who participated in an HIIT with bodyweight program of four weeks
duration, a weekly frequency of training of three times a week, and a 30 min
training session duration. These results are in line with those observed in the
previously proposed experiment [9], demonstrating that 6 weeks of training,
with a frequency of three times a week, and a session duration of 20 minutes,
did not induce improvements in parameters of general physical fitness and in
muscle thickness. However, limitations regarding progression and organization
of the training session were indicated as possible parameters that can be
manipulated to optimize the session, with the objective of improving physical
fitness and also promoting changes in body composition.
Two
other studies [10,43], based on the application of extremely short models of
HIIT with bodyweight (8 sets of 20 seconds of “all-out” stimulus interspersed
with 10 seconds of passive recovery), showed interesting results on different
variables of general physical fitness, highlighting cardiorespiratory fitness.
However, in both works, dumbbells (~3 kg) were used for the execution of one of
the proposed exercises, which mischaracterizes the exclusive use of bodyweight.
Despite this, as it presents interesting results, this HIIT model must be considered,
particularly given the opportunity to use few implements.
High Intensity
Functional Training
High-intensity
functional training (HIFT) is a model in which the concepts of HIIT (exercise
at high intensity) are emphasized, with the application of multisegmental,
multiplanar, and integrated tasks performed at a high intensity of effort. For
this, exercises that use movement patterns such as squatting, pushing, pulling,
and carrying are selected to compose the HIFT training session. Control of the
high intensity of effort in this modality can be carried out through the PSE or
it can be performed in an all-out way. These stimuli are also interspersed with
recovery periods, which may or may not follow a specific duration, and are
generally passive, as observed in other HIIT models [45,46,47,48,49].
In
many contexts, HIFT sessions can be divided into three blocks: 1) movement
preparation, 2) neuromuscular conditioning, and 3) cardiometabolic conditioning
[50]. In the scientific literature, HIFT has often been associated with
"cross" modalities (Cross Training, Mix Modalities Training – MMT,
and Functional Fitness), methods that are capable of promoting multisystem
adaptations, through the concomitant improvement of different parameters of physical
fitness [45]. Based on this, studies have shown that HIFT is able to promote
positive benefits to both body composition [20] and improved performance in
different biomotor abilities [48].
Ratifying
the above, Sperlich et al. [49] verified the
effects of nine weeks of HIFT compared to training associated with high-volume,
low-intensity exercise. After the intervention period, the authors found
significant improvement in body mass, percentage of fat-free mass, fat mass,
body mass index, and muscle strength in both training methods. However, the
HIFT showed greater improvements when the maximum oxygen consumption was
analyzed. In the same vein, Kliszczewicz et al.
[48] observed an increase in aerobic and anaerobic capacity in trained
individuals submitted to four weeks of HIFT.
Although
there are different pre-established HIFT models in the scientific literature
(AMRAP and EMONS), the prescription of this type of protocol can be targeted
and specific, based on work, sports, or daily life activities. This makes it
possible to apply HIFT in different populations, enabling an increase in
functional capacity, in addition to promoting an improvement in physiological
parameters, arising from the accumulation of time spent at high intensity, the
main proposal of HIIT.
High-Intensity
Circuit Training
According
to Clayton et al. [51], high-intensity circuit training (HICT) is a
model generally based on the application of exercises that mimic the movements
used in activities of daily living (squatting, pulling, pushing), which provide
benefits to the physical fitness components related to functionality. HICT is
usually applied with stimuli performed at a high intensity, for about 20 to 40
seconds, followed by pauses, with a work:recovery
ratio ranging from 1:2 to 2:1 [52].
As
the name suggests, the organization of the session follows the traditional
circuit model (all sessions based on circuit) or blocks (minicircuits),
covering between 6 and 12 exercises [53]. In both situations (blocks or
circuit) it is possible to use more than one round, being common the use of 2
to 3 rounds. The average duration of training sessions is usually between 20
and 40 minutes [52]. Overall, the benefits of HICT mainly involve the
improvement in cardiorespiratory fitness and strength and changes in body
composition [52,54].
High-Intensity
Resistance Training
High
Intensity Resistance Training (HIRT) has been used, based on advanced methods
of strength training, with the aim of inducing levels of stress/stimuli beyond those
provided by maximum sets or those conducted up to concentric failure [55]. As
the models use high intensity stimuli interspersed with brief intervals of
passive recovery, the concept of HIIT is present.
The
most popular HIRT protocol was proposed by Paoli et al. [23] and is
based on the rest-pause model. In this protocol, multi-joint exercises are
applied, in which maximal sets are performed (concentric failure) with high
loads (80-85% of 1RM), followed by 20” intervals of passive recovery and resumption
of execution until a new concentric failure. This procedure of pausing and
resuming performance is repeated 2 or 3 times after the first set,
characterizing the rest-pause. Although the study by Paoli et al. [23]
only assessed issues related to energy expenditure, a study by Prestes et al. [56] analyzed the effects of 6 weeks
of training with a similar protocol and observed an increase in muscle strength
and endurance in the upper and lower limbs, as well as muscle hypertrophy in
the thigh of trained men.
Conclusion
The
concept of HIIT is based on the alternation between periods of stimulus
(performed at high intensity) and recovery. From this point on, it is possible
to state that, based on the main objective of HIIT (accumulation of maximum
exercise time at high intensity), using high intensity as a guiding principle,
several exercise models with different neuromuscular stimuli can be applied.
Obviously, the impacts of HIIT and the adaptations in physiological systems in
the medium and long term may vary between the protocols used, however, it seems
to be a consensus that the different models can promote different benefits to
health and physical fitness in general. In addition, the versatility of HIIT
allows it to be performed in different conditions and populations, enabling
broad benefits and minimal complications arising from the practice of this
training method, provided that the information on the application and
monitoring of the variables is observed, making this approach extremely attractive
in the current context of society. Nevertheless, it is suggested that further
studies be conducted in order to increase knowledge about the application of
different protocols based on the HIIT concepts mentioned throughout this
manuscript. In addition, it is recommended that studies are conducted with the
aim of observing possible differences in the acute response and chronic effects
that the different forms of application of HIIT provide to different
populations.
Potential
conflict of interest
No
conflicts of interest have been reported for this article.
Financing
The
present study was carried out without funding.
Authors’
contributions
Conception
and design of the research: Evangelista AL, La Scala
Teixeira CV, Da Silva-Grigoletto ME; Writing of
the manuscript: Evangelista AL, La Scala Teixeira CV, Brandão
LHA, Machado AF, Bocalini DS, Santos LM, Da Silva-Grigoletto ME; Critical review of the manuscript for
important intellectual content: Evangelista AL, La Scala Teixeira CV, Brandão LHA, Da Silva-Grigoletto
ME
References
- Kokkinos P.
Physical activity, health benefits, and mortality risk. ISRN Cardiol 2012;2012(1):1-14.doi: 10.5402/2012/718789 [Crossref]
- Garber CE, Blissmer B, Deschenes MR, Franklin BA, Lamonte MJ, Lee IM, et al. Quantity and quality of exercise for developing and maintaining cardiorespiratory, musculoskeletal, and neuromotor fitness in apparently healthy adults: Guidance for prescribing exercise. Med Sci Sports Exerc 2011;43(7):1334-59. doi: 10.1249/MSS.0b013e318213fefb [Crossref]
- 2019 BV Brasil. Estimativas sobre frequência e distribuição
sociodemográfica de fatores de risco e proteção para doenças crônicas nas
capitais dos 26 estados brasileiros e no distrito federal em 2019. Secretaria
de Gestão Estratégica e Participativa. In: Secretaria de Vigilância em Saúde.
Brasília: Ministério da Saúde (MS); 2020.
- Pinheiro KC, Augusto D, Silva S. Barreiras percebidas para prática de musculação em adultos desistentes da modalidade. Rev Bras Ativ Fís Saúde 2012;15(3):157–62. doi: 10.12820/rbafs.v.15n3p157-162 [Crossref]
- Heinrich KM, Patel PM, O’Neal JL, Heinrich BS. High-intensity compared to moderate-intensity training for exercise initiation, enjoyment, adherence, and intentions: An intervention study. BMC Public Health 2014;14(1):1-6. doi: 10.1186/1471-2458-14-789 [Crossref]
- La Scala Teixeira CV. Musculação time-efficient
otimizando o tempo e maximizando os resultados. Vol1. São Paulo:
Phorte; 2016. p.430-36.
- Amaral PC, Palma DD. Brazil and Argentina survey of fitness trends for 2020. ACSM’s Heal Fit J 2019;23(6):36-40. doi: 10.1249/FIT.0000000000000525 [Crossref]
- Thompson WR. Worldwide survey of fitness trends for 2020. ACSM’s Heal Fit J 2019;23(6):10-8. doi: 10.1249/FIT.0000000000000526 [Crossref]
- Evangelista AL, La Scala Teixeira C, Machado AF, Pereira PE, Rica RL, Bocalini DS. Effects of a short-term of whole-body, high-intensity, intermittent training program on morphofunctional parameters. J Bodyw Mov Ther 2019;23(3):456-60. doi: 10.1016/j.jbmt.2019.01.013 [Crossref]
- Mcrae G, Payne A, Zelt JGE, Scribbans TD, Jung ME, Little JP, et al. Extremely low volume, whole-body aerobic- resistance training improves aerobic fitness and muscular endurance in females. Appl Physiol Nutr Metab 2012;37(6):1124-31. doi: 10.1139/h2012-093 [Crossref]
- Machado AF, Baker JS, Figueira Junior AJ, Bocalini DS. High-intensity interval training using whole-body exercises: training recommendations and methodological overview. Clin Physiol Funct Imaging 2017;378-83. doi: 10.1111/cpf.12433 [Crossref]
- Langton B, King J. Utilizing body weight training with your personal training clients. ACSM’s Heal Fit J 2018;22(6):44-51. doi: 10.1249/FIT.0000000000000433 [Crossref]
- Laursen P, Buchheit M. Science and application of high-intensity
interval training. Champaign: Human Kinetics Publishers; 2019. 672 p.
- Buchheit M, Laursen PB. High-intensity interval training, solutions to the programming puzzle. Part II: anaerobic energy, neuromuscular load and practical applications. Sports Med 2013;43(10):927-54. doi: 10.1007/s40279-013-0066-5 [Crossref]
- Laursen PB, Jenkins DG. The scientific basis for high-intensity interval training: optimising training programmes and maximising performance in highly trained endurance athletes. Sport Med 2002;32(1):53-73. doi: 10.2165/00007256-200232010-00003 [Crossref]
- Buchheit M, Laursen PB. High-intensity interval training, solutions to the programming puzzle part I: Cardiopulmonary emphasis. Sport Med 2013;43(5):313-38. doi: 10.1007/s40279-013-0029-x [Crossref]
- Gosselin L, Kozlowski K, DeVinney-Boymel L, Hambridge C. Metabolic response of different high-intensity aerobic interval training exercise protocols. J Strength Cond Res 2012;26(10):2866-71. doi: 10.1519/JSC.0b013e318241e13d [Crossref]
- Garciá-Pinillos F, Cámara-Pérez JC, Soto-Hermoso VM, Latorre-Román PA. A high intensity interval training (HIIT)- Based running plan improves athletic performance by improving muscle power. J Strength Cond Res 2017;31(1):146-53. doi: 10.1519/JSC.0000000000001473 [Crossref]
- Machado AF, Evangelista AL, Miranda JMQ, Teixeira CVS, Rica RL, Lopes CR, et al. Description of training loads using whole-body exercise during high-intensity interval training. Clinics (Sao Paulo) 2018;29:73:e516. doi: 10.6061/clinics/2018/e516 [Crossref]
- Feito Y, Hoffstetter W, Serafini P, Mangine G. Changes in body composition, bone metabolism, strength, and skill-specific performance resulting from 16-weeks of HIFT. PLoS One. 2018;13(6):1-15. doi: 10.1371/journal.pone.0198324 [Crossref]
- Gibala MJ, Little JP, Macdonald MJ, Hawley JA. Physiological adaptations to low-volume, high-intensity interval training in health and disease. J Physiol 2012;590(5):1077-84. doi: 10.1113/jphysiol.2011.224725 [Crossref]
- Machado AF, Miranda MLJ, Rica RL, Figueira Junior A, Bocalini DS, Carvalho F, et al. Frequência de treinamento no HIIT body work e redução da massa corporal: um estudo piloto. Motricidade 2018;73(1):184-9. doi: 10.6063/motricidade.14321 [Crossref]
- Paoli A, Moro T, Marcolin G, Neri M, Bianco A, Palma A, et al. High-Intensity Interval Resistance Training (HIRT) influences resting energy expenditure and respiratory ratio in non-dieting individuals. J Transl Med 2012;10(1):1-8. doi: 10.1186/1479-5876-10-237 [Crossref]
- Weston M, Taylor KL, Batterham AM, Hopkins WG. Effects of low-volume high-intensity interval training (HIT) on fitness in adults: A meta-analysis of controlled and non-controlled trials. Sport Med 2014;44(7):1005-17. doi: 10.1007/s40279-014-0180-z [Crossref]
- Milanović Z, Sporiš G, Weston M. Effectiveness of high-intensity interval training (HIT) and continuous endurance training for VO 2max improvements: a systematic review and meta-analysis of controlled trials. Sport Med 2015;45:1469-81. doi: 10.1007/s40279-015-0365-0 [Crossref]
- Su LQ, Fu JM, Sun SL, Zhao GG, Cheng W, Dou CC, et al. Effects of HIIT and MICT on cardiovascular risk factors in adults with overweight and/or obesity: A meta-analysis. PLoS One 2019;14(1):1-21. doi: 10.1007/s40279-015-0365-0 [Crossref]
- Shiraev T.
Evidence based exercise clinical benefits of high intensity interval training.
Aust Fam Phys 2012;41(12):960–2. Available from:
https://www.racgp.org.au/afp/2012/december/evidence-based-exercise
- Grace F, Herbert P, Elliott AD, Richards J, Beaumont A, Sculthorpe NF. High intensity interval training (HIIT) improves resting blood pressure, metabolic (MET) capacity and heart rate reserve without compromising cardiac function in sedentary aging men. Exp Gerontol 2018;109:75-81. doi: 10.1016/j.exger.2017.05.010 [Crossref]
- Guiraud T, Gremeaux V, Meyer P, Juneau M. High-intensity interval training in cardiac rehabilitation. Sport Med 2012;42(7):587-605. doi: 10.1016/j.cger.2019.07.011 [Crossref]
- Dun Y, Thomas RJ, Medina-Inojosa JR, Squires RW, Huang H, Smith JR, et al. High-intensity interval training in cardiac rehabilitation: Impact on fat mass in patients with myocardial infarction. Mayo Clin Proc 2019;94(9):1718-30. doi: 10.1016/j.mayocp.2019.04.033 [Crossref]
- Ribeiro PAB, Boidin M, Juneau M, Nigam A, Gayda M. High-intensity interval training in patients with coronary heart disease: Prescription models and perspectives. Ann Phys Rehabil Med 2017;60(1):50-7. doi: 10.1016/j.rehab.2016.04.004 [Crossref]
- Batacan RB, Duncan MJ, Dalbo VJ, Tucker PS, Fenning AS. Effects of high-intensity interval training on cardiometabolic health: A systematic review and meta-analysis of intervention studies. Br J Sports Med 2017;51(6):494-503. doi: 10.1136/bjsports-2015-095841 [Crossref]
- Gibala MJ.
Interval training for cardiometabolic health: Why such a HIIT? Curr Sports Med Rep 2018;17(5):148-50. doi: 10.1249/JSR.0000000000000483 [Crossref]
- Campbell WW, Kraus WE, Powell KE, Haskell WL, Janz KF, Jakicic JM, et al. High-intensity interval training for cardiometabolic disease prevention. Med Sci Sports Exerc 2019;51(6):1220-6. doi: 10.1249/MSS.0000000000001934 [Crossref]
- Laursen PB, Shing CM, Peake JM, Coombes JS, Jenkins DG. Influence of high-intensity interval training on adaptations in well-trained cyclists. J Strength Cond Res 2005;19(3):527-33. doi: 10.1519/15964.1 [Crossref]
- Gibala MJ, Gillen JB, Percival ME. Physiological and health-related adaptations to low-volume interval training: Influences of nutrition and sex. Sport Med 2014;44(2):127-37. doi: 10.1007/s40279-014-0259-6 [Crossref]
- Wormgoor SG, Dalleck LC, Zinn C, Harris NK. Effects of high-intensity interval training on people living with type 2 diabetes: A narrative review. Can J Diabetes 2017;41(5):536-47. doi: 10.1016/j.jcjd.2016.12.004 [Crossref]
- Nunes PRP, Martins FM, Souza AP, Carneiro MAS, Orsatti CL, Michelin MA, et al. Effect of high-intensity interval training on body composition and inflammatory markers in obese postmenopausal women: A randomized controlled trial. Menopause 2019;26(3):256-64. doi: 10.1097/GME.0000000000001207 [Crossref]
- Nemoto K, Gen-no H, Masuki S, Okazaki K, Nose H. Effects of high-intensity interval walking training on physical fitness and blood pressure in middle-aged and older people. Mayo Clin Proc 2007;82(7):803-11. doi: 10.4065/82.7.803 [Crossref]
- Keating SE,
Johnson NA, Mielke GI, Coombes JS. A systematic review and meta-analysis of
interval training versus moderate-intensity continuous training on body
adiposity. Obes Rev 2017;18(8):943-64. doi: 10.1111/obr.12536 [Crossref]
- MacInnis MJ, Gibala MJ. Physiological adaptations to interval training and the role of exercise intensity. J Physiol 2017;595(9):2915-30. doi: 10.1113/JP273196 [Crossref]
- Joyner MJ, Coyle EF. Endurance exercise performance: The physiology of champions. J Physiol 2008;586(1):35-44. doi: 10.1113/jphysiol.2007.143834 [Crossref]
- Schaun GZ, Pinto SS, Silva MR, Dolinski DB, Alberton CL. Whole-body high-intensity interval training induce similar cardiorespiratory adaptations compared with traditional high-intensity interval training and moderate-intensity continuous training in healthy men. J Strength Cond Res 2018;32(10):2730-42. doi: 10.1519/JSC.0000000000002594 [Crossref]
- Machado AF, Miranda MLJ, Rica RL, Figueira Junior A, Bocalini DS. Bodyweight high-intensity interval training: A systematic review. Rev Bras Med do Esporte 2018;24(3):234–7. doi: 10.1590/1517-869220182403176199 [Crossref]
- Feito Y, Heinrich K, Butcher S, Poston W. High-Intensity Functional Training (HIFT): Definition and research implications for improved fitness. Sports 2018;6(3):76. doi: 10.3390/sports6030076 [Crossref]
- Murawska-Cialowicz E, Wojna J, Zuwala-Jagiello J. Crossfit training changes brain-derived neurotrophic factor
and irisin levels at rest, after wingate and
progressive tests, and improves aerobic capacity and body composition of young
physically active men and women. J Physiol Pharmacol [Internet] 2015 [cited 2021 Dec 23];66(6):811-21.
Available from: https://pubmed.ncbi.nlm.nih.gov/26769830/
- Willis EA, Szabo-Reed AN, Ptomey LT, Honas JJ, Steger FL, Washburn RA, Donnelly JE. Energy expenditure and intensity of group-based high-intensity functional training: a brief report. J Phys Act Health 2019;16(6):470-6. doi: 10.1123/jpah.2017-0585 [Crossref]
- Kliszczewicz B,
McKenzie M, Nickerson B. Physiological adaptation following four-weeks of
high-intensity functional training. Mil Med Pharm J Serbia 2017;76(3):272-7. doi: 10.2298/VSP170228095K [Crossref]
- Sperlich B, Wallmann-sperlich B, Zinner C, Stauffenberg V Von. Functional high-intensity circuit training improves body composition, peak oxygen uptake, strength, and alters certain dimensions of quality of life in overweight women. PLoS One 2017;8:1-9. doi: 10.3389/fphys.2017.00172 [Crossref]
- Silva-Grigoletto ME, Resende-Neto AG, La Scala Teixeira CV. Treinamento funcional: um “update” conceitual. Rev Bras Cineantropometria e Desempenho Hum 2020. doi: 10.1590/1980-0037.2020v22e72646 [Crossref]
- Clayton BC, Tinius RA, Winchester
LJ, Menke BR, Reece MC, Maples JM. Physiological and perceptual responses to
high-intensity circuit training using body weight as resistance: Are there
sex-specific differences? Int J Exerc Sci [Internet].
2019 [cited 2021 Dec 23];12(4):245–55. Available from:
https://pubmed.ncbi.nlm.nih.gov/30899349/
- Batrakoulis A, Jamurtas AZ, Georgakouli K, Draganidis D, Deli CK, Papanikolaou K, et al. High intensity, circuit-type integrated neuromuscular training alters energy balance and reduces body mass and fat in obese women: A 10-month training-detraining randomized controlled trial. PLoS One 2018;13(8):1-21. doi: 10.1371/journal.pone.0202390 [Crossref]
- Muñoz-Martínez FA, Rubio-Arias J, Ramos-Campo DJ, Alcaraz PE. Effectiveness of resistance circuit-based training for maximum oxygen uptake and upper-body one-repetition maximum improvements: A systematic review and meta-analysis. Sport Med 2017;47(12):2553-68. doi: 10.1007/s40279-017-0773-4 [Crossref]
- Klika B, Jordan C. High-intensity circuit training using body weight: Maximum results with minimal investment. ACSM’s Heal Fit J 2013;17(3):8-13. doi: 10.1249/FIT.0b013e31828cb1e8 [Crossref]
- Giessing J, Eichmann B, Steele J, Fisher J. A comparison of low volume “high-intensity-training” and high-volume traditional resistance training methods on muscular performance, body composition, and subjective assessments of training. Biol Sport 2016;33(3):241-9. doi: 10.5604/20831862.1201813 [Crossref]
- Prestes J, Tibana RA, Sousa EA, Nascimento DC, Rocha PO, Camarço NF, et al. Strength and muscular adaptations after 6 weeks of rest-pause vs. traditional multiple-sets resistance training in trained subjects. J Strength Cond Res 2019;33:S113-21. doi: 10.1519/JSC.0000000000001923 [Crossref]
- Helgerud J, Høydal K, Wang E, Karlsen T, Berg P, Bjerkaas M, et al. Aerobic high-intensity intervals improve VO2max more than moderate training. Med Sci Sports Exerc 2007;39(4):665-71. doi: 10.1249/mss.0b013e3180304570 [Crossref]
