Rev Bras Fisiol Exerc 2020;19(6):519-31
doi: 10.33233/rbfex.v19i6.4376
REVIEW
Effects
of high-intensity interval training on health-related physical fitness in
children and adolescents: a systematic review
Efeitos do treinamento
intervalado de alta intensidade na aptidão física relacionada à saúde em
crianças e adolescentes: uma revisão sistemática
Rafael Luiz Mesquita
Souza1,2, Felipe José Aidar1,2,3, Sílvia Schütz1,2,
Jymmys Lopes dos Santos2,3, Nara Michelle
Moura Soares4, Silvan Silva de Araújo2,5,
Anderson Carlos Marçal2,6
1Department of Physical
Education, Federal University of Sergipe, São Cristóvão,
SE, Brazil
2Program of Physical
Education, Federal University of Sergipe, São Cristóvão,
SE, Brazil
3Group of Studies and
Research of Performance, Sport, Health and Paralympic Sports - GEPEPS, Federal
University of Sergipe, São Cristóvão, SE, Brazil
4Department of Physical
Education, Tiradentes University, Aracaju, SE,
Brazil
5Secretary of State for
Education, Sport, and Culture (SEED/SE), Aracaju, SE, Brazil
6Department of
Morphology, Federal University of Sergipe, São Cristóvão,
SE, Brazil
Received
on: September 18, 2020; Accepted on: November 5, 2020.
Correspondence: Rafael Luiz Mesquita
Souza, Rua Quintino de Lacerda, 648, 49500-004 Itabaiana SE, Brazil
Rafael Luiz Mesquita
Souza: rlms2010@hotmail.com
Felipe
José Aidar: fjaidar@gmail.com
Sílvia Schütz: silvia_schutz@hotmail.com
Jymmys Lopes dos Santos,
e-mail: jymmyslopes@yahoo.com.br
Nara Michelle Moura
Soares: narasoares963@hotmail.com
Silvan Silva de Araújo:
silvan.ssa@gmail.com
Anderson Carlos Marçal:
acmarcal@yahoo.com
Abstract
Introduction: High-intensity interval training (HIIT) can improve health and
physical conditioning, and it also contributes to the increase of
cardiorespiratory capacity (VO2max), localized muscular resistance
and improvement of body composition. However, its effects on health-related
physical fitness in children and teenagers are not yet clear. Objective:
The objective of this paper was to analyze the effectiveness of HITT on
health-related physical fitness with children and teenagers. Methods:
This study analyzed papers from the following databases: SportDiscus,
Web of Science, Medline by way of PubMed, Scopus, Scielo
e Bireme. The PICO strategy was applied in order to select the papers, and
CONSORT was applied to assess the quality of randomized clinical trials. 511
papers were found. Out of this number, 101 papers were eligible for abstract
analysis. Results: At the end of the selection process, ten papers met
the inclusion criteria. The results suggest that among the variables analyzed
by the papers that addressed health-related physical fitness, HIIT demonstrated
efficacy in VO2max, body mass index and fat percentage in this
population. Conclusion: However, it was not possible to state that HIIT
promoted adjustments in flexibility, strength and localized muscular
resistance, requiring further studies to assess its effects on health-related
physical fitness.
Keywords: exercise; adolescent; primary health care
Resumo
Introdução: O treinamento
intervalado de alta intensidade (HIIT) é capaz de promover melhora da saúde e
condicionamento físico e contribuir para o aumento da capacidade
cardiorrespiratória (VO2máx), da resistência muscular localizada e
melhora da composição corporal. No entanto, seus efeitos sobre a aptidão física
relacionada a saúde de crianças e adolescentes ainda não são bem esclarecidos. Objetivo:
O objetivo do estudo foi analisar a eficácia do HIIT na aptidão física
relacionada a saúde de crianças e adolescentes. Métodos: O presente
estudo analisou artigos das bases de dados (SportDiscus,
Web of Science, Medline via PubMed,
Scopus, Scielo e Bireme). Foi aplicada a estratégia
PICO para selecionar os artigos e o CONSORT para avaliar a qualidade dos ensaios
clínicos randomizados. Foram encontrados 511 artigos. Desse total, 101 artigos
foram elegíveis para a análise do resumo. Resultados: Ao final do
processo de seleção resultaram em 10 artigos que compuseram os critérios de
inclusão. Os resultados sugerem que entre as variáveis analisadas pelos artigos
referentes a aptidão física relacionada a saúde, o HIIT demonstrou eficácia na
VO2máx, índice de massa corporal e percentual de gordura nessa
população. Conclusão: Contudo, não foi possível afirmar que o HITT promoveu
ajustes na flexibilidade, na força e na resistência muscular localizada, sendo
necessário maiores estudos para avaliar seus efeitos sobre a aptidão física
relacionada a saúde.
Palavras-chave: exercício físico;
adolescente; atenção primária à saúde
Introduction
Children and adolescents are affected by diseases resulting from
sedentary behavior. Nearly 23% of the world population under the age of 18
perform less than 150 minutes of weekly physical activities [1-3]. Therefore,
the prevalence of hypokinetic diseases, such as hypertension and obesity, tends
to increase in this age group, which contributes to higher health risk and a
low level of physical fitness [4].
Health-related physical fitness (HRPF) is a predictive tool for children's
health [5]. For children and adolescents, the principal indicators of HRPF are
body composition, cardiorespiratory conditioning, levels of flexibility, and
muscle strength [6-8].
For improvement of physical fitness, physical exercise is recommended by
physical educators for children, young people, or adolescents, as well as those
belonging to other age groups [9]. In this sense, some studies assess the
effects of high-intensity exercise on HRPF. Among the different modalities,
high-intensity interval training (HIIT) appears as an alternative that requires
a short period for its execution when compared to the traditional model of
moderate aerobic practice [10].
HIIT is an endurance method characterized by periods of high intensity,
interspersed with periods of low intensity or rest for recovery. Most protocols
employ 80-100% of the peak aerobic power (VO2peak) [11,12],
considering the maximum volume of oxygen consumed by the individual during the
assessment and not necessarily the maximum breathing capacity (VO2)
[13].
Some studies suggest that HIIT can promote adjustments of biological
markers, such as increases in aerobic capacity, ventricular ejection volume
fraction, expression of glucose transporter isoform four (GLUT-4) in muscle
cells, and VO2max and adjustments of other components, like the
reduction in the percentage of abdominal fat, greater capacity for muscle work
and changes in body composition in general [9,14,15].
Despite the existence of studies that address the effects of HIIT in
children and adolescents, the evidence is not conclusive as to whether this
type of training can promote beneficial adjustments on physical fitness in this
population. In this sense, the present study aims to assess the impact of HIIT
on the components of HRPF in children and adolescents.
Methods
Systematic
literature search strategy
The PICO strategy (Patient, Intervention, Comparison, and Outcomes) was
used following the Preferred Reporting Items for Systematic Reviews and Meta-Analyzes
(PRISMA) methodology. The search for the articles was carried out by two
researchers, using the databases Scielo, Pubmed, Scopus, SPORTDiscus, and
Medline. At Scielo and Pubmed,
keywords were used for a broader range of studies; at SPORTDiscus,
Health Sciences Descriptors (DeCS) and synonyms were
used; at Medline, Medical Subject Headings (MeSH)
were used for indexed articles. The keywords used were:
adolescent, children, teenager, physical fitness, high-intensity interval
training, and HIIT crossed with the Boolean connectors "AND, OR" or
"AND OR". There was no date limit for the starting period in the
selection of the articles, which ended in March 2020. The article was submitted
on the York University platform (https://www.crd.york.ac.uk/prospero/), which
the number of identification on the platform is
CRD42020213497.
Inclusion
and exclusion criteria
The inclusion criteria adopted were studies of the randomized clinical
trial type involving children and/or adolescents aged 6-19 years [16], having
applied HIIT and analyzing some of the related indicators (flexibility, body
composition, strength, and muscular resistance) with HRPF. As an exclusion
criterion, the training period of fewer than 4 weeks was analyzed.
The interventions of interest were those that showed results after 4
weeks of training with HIIT. This research verified the differences between the
intervention and control groups related to the variables: cardiorespiratory
fitness (VO2max and VO2peak) and body fat percentage
(%F).
Data
extraction
For data extraction, standardized Excel spreadsheets were used,
respecting CONSORT standards as a guide to randomized clinical trials [17].
Information about characteristics, sample, eligibility criteria, intervention
methods, and the results found were used by two reviewers. To analyze the level
of agreement between the reviewers, the Kappa Test was applied. There was 100%
(k = 1.00, P < 0.001, 95% CI) and 81.0% (k = 0.81, P < 0.001 and 95% CI)
of agreement for titles and abstracts, respectively. During the search for
articles in the databases, the titles, abstracts, complete articles, and their
eligibility for this systematic review were analyzed. In case of disagreement,
a third reviewer was consulted.
Quality
assessment of individual studies
In this stage, the quality of original works was carefully checked, and
that used HIIT physical training. Articles with a percentage of ≥ 80%
were selected, following the CONSORT guidelines. Thus, the methodological
quality, risk of bias, as well as the inclusion and exclusion criteria,
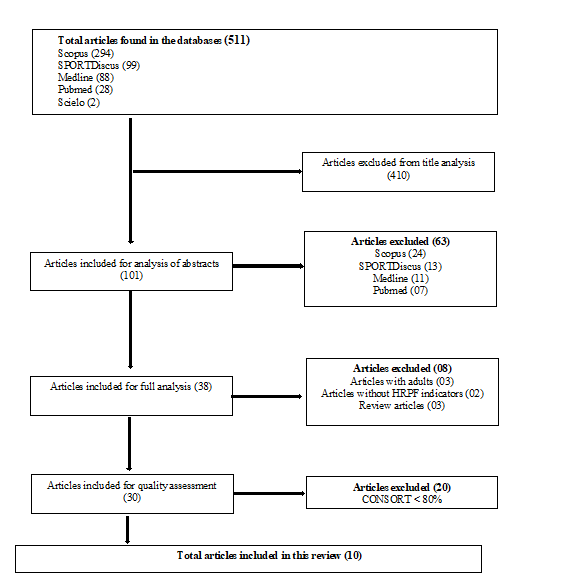
statistical data, and results were analyzed, with 10 articles selected in the
last step (Figure 1).
The risk of bias assessment was performed using the Risk of bias tool,
following the characteristics: generation of the random sequence; allocation
concealment; blinding of participants and professionals; blinding of evaluators
and outcome; incomplete outcomes; report of the selective result and other
sources of bias (Figure 2).
HRPF
= Health-Related Physical Fitness; CONSORT = Consolidated Standards of
Reporting Trials; Source: Elaborated by the authors
Figure
1 - Flowchart of study selection using the inclusion
criteria
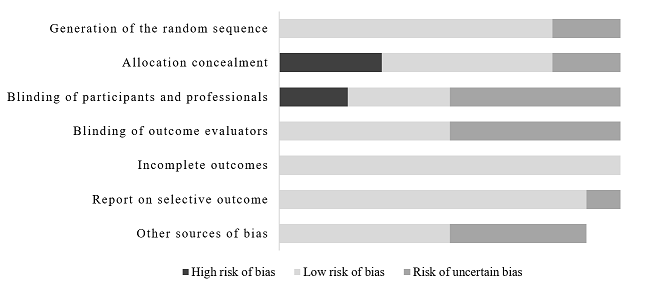
Figure
2 - Risk of bias assessment
Results
Inclusion
of studies
511 articles were found, of which 410 were rejected according to the
evaluation of the title, leaving 101 of them eligible for analysis of the
abstract. Of these, 38 studies were qualified for a full reading. At the end of
the research selection process, 10 articles remained that met the inclusion
criteria (Table I).
Table
I - Characteristics of the selected studies. (see
PDF annexed)
Design
and sample
The
eligible studies presented experimental design and randomization of individuals
for their allocation, had intervention and control groups. The works contained
19-197 participants of both sexes, whose physical condition varied between
obese, athletes, and schoolchildren.
Interventions
Some
studies showed variation in the duration of interventions. However, 5 studies
maintained the same constancy and used 12 weeks [20,22,23,25,26]. The other
authors used HIIT for 4 [18,27], 8 [19], 6 [21] and 28 weeks [24].
The works also demonstrated different forms of intervention: long HIIT
and Repeated-sprint training (RST) with a ratio between stimulus and rest over
1 minute in duration and intensity of 90% VO2peak, and 30 seconds
with an intensity of 170% of peak power [23]; only long HIIT between 90% and
100% of maximum heart rate (HRmax), in the form of
running on the treadmill [27].
There were comparisons between HIIT and diet: long HIIT in the running
mode on the treadmill between 80% and 90% of HRmax in
the intervention group and a reduction of 300 to 400 calories in the control
group [26]. Two studies [24,26] applied long HIIT in the intervention group and
activities in physical education classes in the control group, with intensities
of 80-95% of HRmax and 100% of maximum aerobic speed,
in free-running on the soccer field, respectively.
HIIT was also used in the form of exercises such as squats, short and long
jumps and sprints with maximum efforts in the main group, sports activities in
physical education classes, and aerobic exercise and sports activities in the
control group [20].
Long HIIT at 140% of the speed of the individual anaerobic threshold was
used in Small-Sided Games, with characteristics of interval training with high
intensity, in intensity equal to the previous one [26]. Short HIIT at 74% of HRmax was used in resistance training with squats with
bodyweight, jumps, push-ups, and skipping, in addition to activities in the
physical education class for the control group [19].
Long HIIT between 85-95% of HRmax was also
used, with active rest between 50-70% of HRmax in the
intervention group, and the control group applied cardiorespiratory training of
moderate-intensity, maintaining the same volume of 40 minutes for both and
60-70 % of HRmax of intensity in the running mode on
the treadmill [22]. Finally, in another study that used treadmill running on a
long HIIT in the main group of 80-95% HRmax, together
with motivational messages [21]. In the second group, the same HIIT model was
applied, but without motivational messages. Although the training is high
intensity, no study has reported severe controversial effects during and after
the intervention season.
Results
and intervention measures (primary)
From the analysis of the selected articles, variables directly related
to HRPF were highlighted, according to the guidelines recommended by FitnessGram, American Alliance for Health, Physical
Education, Recreation and Dance, and Projeto Esporte Brasil [28-30]. The
cardiorespiratory capacity (VO2max and VO2peak), based on
Léger's tests [31], better known as the 20m Shuttle Run, Yo-Yo Intermittent
Endurance test or Vaivém [12,19,20,25] and those
recommended by German National Teams [18].
The other estimates were performed using ergospirometry
using a treadmill ramp protocol [22,27]. Two studies used the lower limb cycle
ergometer [23,26]. However, there was an article that applied the 6MWT
(6-minute walk test) walk test protocol to assess cardiorespiratory fitness
[24].
BMI and %F variables were also analyzed. The methods used were the
classification by Cole et al. [32] for BMI and tetrapolar bioimpedance
(BIA) [25]. Two other studies used the formula Kg/Height² to measure %F and
BMI, respectively [23,26]. Also, the other studies evaluated these same
parameters by the differentiated equations regarding sex [21,24].
Results
and intervention measures (secondary)
The selected studies also evaluated waist circumference (WC),
waist-to-hip ratio (WHR), and WHtR/WHR ratio [21,24].
WHtR and WHR are related to obesity and overweight,
as well as low rates of physical fitness [32]. The WC measurement was measured
using the umbilicus line as a reference [21,23], and also as the smallest
abdominal circumference, the region located between the 10th rib and the border
of the iliac crest considered as the midpoint [20,21,24].
Maximum heart rate was assessed to determine cardiorespiratory fitness
[26,27] during the 6-minute run test [21]; from the HR predicted from age [23];
the highest mean HR after performing the exercises in both groups [19] in the
20m Shuttle Run test [20], using the "220-age” equation [26] and
the Yo-Yo Intermittent Endurance test [25].
Quality
of studies
According to CONSORT, out of a total of 30 studies, 20 had a
classification of 50-79.9% and 10 ≥ 80%. Of the total of 30 articles,
25%, 60%, and 70% indicated the study model in the title, how the sample was
calculated; and 70% described the method used to generate randomization,
respectively. Also, 85%, 80%, and 45% reported the adverse effects of the
interventions, the limitations of the studies, and informed the source of study
funding, respectively.
Discussion
The present review found that HIIT, despite the model applied, promotes
beneficial adjustments in the juvenile population. The main ones were:
increased cardiorespiratory capacity [20,22,23,35]; decreased BMI
[19,21,24-26]; reduction in %F [21,24-26], improvement in maximum heart rate
[23,25]; widening of the anaerobic threshold [18]; attenuation of the waist-hip
ratio and waist circumference [21,24].
Of the studies evaluated, 4 showed differences between the pre- and
post-training in cardiorespiratory fitness [20,22,23,27]. Regarding such
parameters, other authors corroborating these findings showed that HIIT
improved both anaerobic and aerobic parameters, predictive measures of good
cardiovascular health in healthy and obese students [18,36,37].
For HRPF, cardiorespiratory fitness is an important predictor and is
inversely related to the development of comorbidities such as obesity,
hypertension, and diabetes. Thus, cardiorespiratory conditioning is the best
indicator of physical fitness related to longevity [38,39]. Besides, an inverse
relationship between BMI and VO2max was demonstrated. These results
suggest that physical inactivity contributes to a greater propensity to the
development of body adiposity and obesity in this sample population [40].
However, the mechanism involved is still not completely elucidated and requires
further research to demonstrate the relationship between VO2max and
the genesis of body adiposity in this population.
Regarding HRmax, although not directly
involved in HRPF assessment, it is related to VO2max [25,35]. Short
HIIT improved both HRmax and VO2max [25].
However, there is still no consensus on the effects of HIIT on body mass and
composition. The BMI and/or %F were reduced according to some authors
[19,20,24-26], as well as reported an improvement in the level of physical
conditioning and less probability of developing diseases related to HRPF.
However, in other studies, HIIT has not been able to promote adjustments in
these variables [22,23]. Also, other authors suggest that the higher the BMI
values, the lower the level of cardiorespiratory and muscle fitness [41].
Therefore, these results suggest a need for further investigation of the
influence of these variables on physical fitness. It is relevant to note that
60% of the studies evaluated were composed of overweight or obese children
and/or adolescents, indicating that other pathologies, as well as an increase
in cardiovascular risk, are associated with a decrease in the level of physical
activity and/or an increase in behavior sedentary; conditions antagonistic to
HRPF [42,43].
HIIT was effective in improving VO2max and/or BMI parameters
in eutrophic children and adolescents [19]. In another study, in
obese/overweight individuals, HIIT was more effective in decreasing BMI and %F
[44]. We confirm the hypothesis demonstrated by these same authors, who suggest
that this effect is due to the higher release of catecholamines, which could
induce an exacerbated lipolytic effect in this population after the practice of
HIIT by mechanisms still unknown.
Sex is a factor that can influence the parameters evaluated. Some
authors suggest that the physiological responses, fat percentage, and muscle
mass levels are different [45] in the maturation stages of girls and boys. A
male group obtained better adjustments in VO2max, flexibility,
muscle strength, and endurance, BMI, and %F than the female group [46]. In this
same article, the authors suggest that due to the lower level of physical
activity, girls show a more pronounced response when submitted to some form of
exercise, which may have contributed to the improvement of BMI and VO2max
parameters.
However, some evidence is contradictory. In another study that assessed
the HRPF level of adolescents, boys had better HRPF scores, except for
flexibility [47]. In this study, it was also proposed that due to the high
variability in the age group of children and adolescents, the different
maturation levels may have influenced the interpretation of the results.
In this sense, although both sexes show changes in BMI and %F after HIIT,
girls obtained better results in these variables [24]. The mixed control group,
which performed moderate activities in physical education classes, showed an
increase in BMI. However, moderate physical activity was not able to change the
BMI and %F in children and adolescents, respectively [19,25].
It is important to note that the influence of training time and duration
of interventions with HIIT on the variables BMI, %F, and VO2max
still need further investigation. The training period capable of inducing
adjustments in the body was 4 to 28 weeks, as well as the session time between
4 to 60 minutes in duration. Even with these variations, it is noted that there
was an improvement in BMI, %F or VO2max, for HRPF. However, the
study that used the supra HIIT (RST) lasting 4 minutes per session, only
promoted an improvement in VO2max.
It is noteworthy that most protocols that maintained intensities between
85 to 100% of heart rate or MAS (Maximal Aerobic Speed), with an average
duration of 40 minutes, had positive effects both on body composition and on
cardiorespiratory capacity. For the latter, significant adjustments occurred
after 4 weeks of training [21-26].
It should be noted that among the different types of existing HIIT, the
most used were: long HIIT, greater than 1 minute of stimulus/rest; Short HIIT,
up to 1 minute of stimulus/rest; Sprint Interval Training (SIT), up to 30sec of
stimulus/4min of rest; and RST, 10sec of stimulus/20sec of rest. Among them,
the one that most provided positive changes for HRPF was the long HIIT that
promoted beneficial adjustments in cardiorespiratory capacity, BMI, and %F
[20-24,26,38-40]. Short HIIT and SIT, in turn, were also able to promote
adjustments in BMI, while RST modulated only VO2max [48]. Regarding
the comparisons made in the study mentioned above, it is relevant to note that
the type of exercise used in the form of HIIT (running, cycling or rowing) has
been shown to influence the magnitude of the results, thus limiting
generalizations and more accurate comparisons.
Conclusion
HIIT was effective in improving BMI, %F, and VO2max,
indicating that this training methodology promotes positive adjustments in
these HRPF parameters. However, it was not possible to state that HIIT was
effective in improving local muscle strength and endurance, as well as
flexibility. Also, long HIIT was more effective in promoting beneficial
adjustments in some components of HRPF (body mass index, cardiorespiratory
capacity, and fat percentage) and secondary variables (heart rate, hip
circumference, and waist-to-hip ratio). Therefore, it is recommended a minimum
time between 4 and 8 weeks with minimum intensities of 85% of HRmax and an average time of 40 minutes of session duration
to be able to modulate BMI, %F, and/or VO2max. Besides, it is
crucial to standardize and/or normalize the groups according to the age groups
with the smallest interval, according to the maturation level of each
participant.
References
- World
Health Organization. Summary report of the update of systematic reviews of the
evidence to inform the WHO guidelines on physical activity, sedentary behavior
and sleep in children under 5 years of age. Geneva: World Health
Organization; 2018. https://doi.org/10.1123/jpah.2019-0457
- American
College of Sports Medicine. Diretrizes do ACMS para os testes de esforço e sua
prescrição. 9th ed. Rio de Janeiro: Guanabara Koogan; 2014.
https://doi.org/10.1249/01.mss.0000496000.56508.f6
- World
Health Organization. WHO Guidelines on physical activity, sedentary behavior
and sleep for children under 5 years of age. Geneva: WHO; 2019.
https://doi.org/10.1123/jpah.2019-0457
- Block
KV, Klein CH, Szklo M, Kuschnir
MCC, Abreu GA, Barufaldi LA et al. ERICA: prevalências de
hipertensão arterial e obesidade em adolescentes brasileiros. Rev Saúde Pública 2016;50(Supl.1):1–13.
https://doi.org/10.1590/s01518-8787.2016050006685
- Vian F, Pedretti A, Gaya A,
Gaya AR, Volkweis Junior JM. Aptidão física
relacionada à saúde de escolares de Canoas/RS. Saúde (Santa Maria) 2018;44(2):1-14.
https://doi.org/10.5902/2236583432767
- World
health organization. WHO Guidelines on physical activity, sedentary behaviour; 2019.
https://doi.org/10.1007/springerreference_70205
- Montoro APPN, Leite CR,
Espíndola JA, Alexandre JM, Reis MS, Capistrano R et al. Aptidão física
relacionada à saúde de escolares com idade de 7 a 10 anos TT - Physical fitness related to the health
of 7-10 year-olds student. ABCS Health Sciences
2016;41(1):29-33. https://doi.org/10.7322/abcshs.v41i1.842
- Mancilla R, Torres P, Álvarez
C, Schifferli I, Sapunar J,
Díaz E. Ejercicio físico interválico
de alta intensidad mejora el control glicêmico y la capacidad aeróbica en pacientes com intolerancia a la glucosa. Revista Médica de
Chile 2014;142(1):34-9. https://doi.org/10.4067/s0034-98872014000100006
- Gomes PP, Silva HJG,
Lira CTC, Lofrano-Prado MC, Prado WL. Efeitos de diferentes intensidades de
treinamento aeróbio sobre a composição corporal em adolescentes obesos. Rev Bras Cineantrop
Desempenho Hum 2013;15(5):594-603.
https://doi.org/10.5007/1980-0037.2013v15n5p594
- Gibala
MJ, Gillen JB, Percival ME. Physiological and
health-related adaptations to low-volume interval training: influences of
nutrition and sex. Sports Med 2014;44(Suppl 2):S127-S137. https://doi.org/10.1007/s40279-014-0259-6
- Weston
KS, Wisløff U, Coombes JS. High-intensity interval
training in patients with lifestyle-induced cardiometabolic disease: A
systematic review and meta-analysis. Br J Sports Med 2014;48(16):1227-34.
https://doi.org/10.1136/bjsports-2013-092576
- Menezes
Junior FJ, Jesus IC, Leite N. Predictive equations of
maximum oxygen consumption by shuttle run test in children and adolescents: a
systematic review. Rev Paul Pediatria
2019;37(2):241–251.https://doi.org/10.1590/1984-0462/;2019;37;2;00016
- Keating
SE, Machan EA, O’Connor HT, Gerofi JA, Sainsbury A, Caterson ID et al. Continuous exercise but not high
intensity interval training improves fat distribution in overweight adults. J Obes
2014;2014:834865. https://doi.org/10.1155/2014/834865
- Del Vecchio FB,
Galliano LM, Coswig VS. Aplicações do exercício
intermitente de alta intensidade na síndrome metabólica. Rev
Bras Ativ Física e Saúde
2013;18(6):669-87. https://doi.org/10.12820/rbafs.v.18n6p66
- World
Health Organization. Young people’s health – a challenge for society: report of
a WHO study group on young people and health for all. Geneva: WHO; 1986.
https://doi.org/10.1002/hpm.4740050310
- World
Health Organization. WHO Guidelines on physical activity, sedentary behaviour; 2019.
https://doi.org/10.1007/springerreference_70205
- Schulz
KF, Altman DG, Moher D. CONSORT 2010 Statement: updated guidelines for
reporting parallel group randomised trials. BMJ
2010;340:c332. https://doi.org/10.1136/bmj.c332
- Faude O, Steffen A, Kellmann
M, Meyer T. The effect of short-term interval training during the competitive
season on physical fitness and signs of fatigue: a crossover trial in
high-level youth football players. Int J Sports Physiol
Perform 2014;9(6):936-44. https://doi.org/10.1123/ijspp.2013-0429
- Costigan
SA, Eather N, Plotnikoff
RC, Taaffe DR, Lubans DR. High-intensity interval
training for improving health-related fitness in adolescents: a systematic
review and meta-analysis. Br J Sports Med
2015;49(19):1253-61. https://doi.org/10.1136/bjsports-2014-094490
- Martínez SR, Ríos LJC, Tamayo IM, Almeida LG,
López-Gomez MA, Jara CC. An
after-school, high-intensity, interval physical activity program improves
health-related fitness in children. Motriz. Rev Educ Fis 2016;22(4):359-7.
https://doi.org/10.1590/s1980-6574201600040022
- Herget S, Reichardt S, Grimm A, Petroff
D, Käpplinger J, Haase M et
al. High-intensity interval training for overweight adolescents: Program
acceptance of a media supported intervention and changes in body composition.
Int J Environ Res Public Health 2016;13(11).
https://doi.org/10.3390/ijerph13111099
- Dias
KA, Ingul CB, Tjønna AE,
Keating SE, Gomersall SR, Follestad
T et al. Effect of high-intensity interval training on fitness, fat mass and
cardiometabolic biomarkers in children with obesity: a randomized controlled
trial. Sports Med 2018;48(3):733-46.
https://doi.org/10.1007/s40279-017-0777-0
- Chuensiri N, Suksom
D, Tanaka H. Effects of high-intensity intermittent training on vascular
function in obese preadolescent boys. Child Obes
2018;14(1):41-9. https://doi.org/10.1089/chi.2017.0024
- Delgado-Floody P, Espinoza-Silva M, García-Pinillos
F, Latorre-Román P. Effects of 28 weeks of
high-intensity interval training during physical education classes on
cardiometabolic risk factors in Chilean schoolchildren: a pilot trial. Eur J Pediatr
2018;177(7):1019-27. https://doi.org/10.1007/s00431-018-3149-3
- Cvetković, N, E Stojanović E, Stojiljković
N, Nikolić D, Scanlan AT, Milanović
Z. Exercise training in overweight and obese children: Recreational football
and high-intensity interval training provide similar benefits to physical
fitness. Scand J Med Sci Sports 2018;28:18-32.
https://doi.org/10.1111/sms.13241
- Plavsic L, Knezevic
OM, Sovtic A, Minic P, Vukovic R, Mazibrada I et al.
Effects of high-intensity interval training and nutrition advice on
cardiometabolic markers and aerobic fitness in adolescent girls with obesity.
Appl Physiol Nutr Metab 2020;45(3):294-300.
https://doi.org/10.1139/apnm-2019-0137
- Seo MW, Lee JM, Jung HC, Jung SW, Song
JK. Effects of various work-to-rest ratios during high-intensity interval
training on athletic performance in adolescents. Int J Sports Med 2019;40(8):503-10.
https://doi.org/10.1055/a-0927-6884
- Plowman
SA, Meredith MD, eds. Fitnessgram/Activitygram
reference guide. 4th ed. Dallas:
The Cooper Institute; 2013.
https://doi.org/10.1123/jpah.3.s2.s5
- Gaya A, Silva G.
Projeto Esporte Brasil, observatório permanente dos indicadores de saúde e
fatores de prestação esportiva em crianças e jovens: manual de aplicação de
medidas e testes, normas e critérios de avaliação. Rio
Grande do Sul: UFRGS; 2016.
- American
Alliance for Health, Physical Education, Recreation, and Dance. Health related
physical fitness test manual. Washington: AAHPERD; 1980.
https://doi.org/10.1080/07303084.1982.10631187
- Léger
L, Gadoury C. Validity of the 20 m shuttle run test
with 1 min stages to predict VO2 max in adults. Canadian Journal of
Sports Science 1989;14(1):21-6.
- Cole
TJ, Bellizzi MC, Flegal KM,
Dietz WH. Establishing a standard definition for child overweight and obesity
worldwide: international survey. BMJ 2000;320(7244):1240-1243.
https://doi.org/10.1136/bmj.320.7244.1240
- Pelegrini A, Silva DAS,
Silva JMFL, Grigollo L, Petroski
EL. Anthropometric indicators of obesity in the prediction
of high body fat in adolescents. Rev Paul Pediatr 2015;33(1):56–62.
https://doi.org/10.1016/s2359-3482(15)30031-2
- Moghiseh M, Habibi
E, Aramesh N, Hasanzadeh A,
Khorvash MK, Poorrahmatian
AH. The association between VO2max and heart
rate of casting industry workers. J Occup Health
Epidemiol 2013;2(1):20-6. https://doi.org/10.18869/acadpub.johe.2.1.2.20
- Sharma
VK, Subramanian SK, Radhakrishnan K, Rajendran R, Ravindran BS, Arunachalam V.
Comparison of structured and unstructured physical activity training on
predicted VO2max and heart rate variability in adolescents - a
randomized control trial. J Basic Clin Physiol Pharmacol 2017;28(3):225-38.
https://doi.org/10.1515/jbcpp-2016-0117
- Foster
C, Farland CV, Guidotti F,
Harbin M, Roberts B, Schuetle J et al. The effects of
high intensity interval training vs steady state training on aerobic and
anaerobic capacity. J Sports Sci Med 2015;14(4):747-55.
- Alonso-Fernández
D, Fernández-Rodríguez R, Taboada-Iglesias Y, Gutiérrez-Sánchez A. Impact of a
HIIT protocol on body composition and VO2max in adolescents. Sci Sports
2019;34(5):341-7. https://doi.org/10.1016/j.scispo.2019.04.001
- Silva PR, Faria WF,
Silva JM, Santos GC, Santos RG, Stabelini Neto A.
Aptidão física e fatores de risco cardiometabólicos
em adolescentes: um estudo longitudinal. Revista Contexto
& Saúde 2020;20(38):170-6. https://doi.org/10.21527/2176-7114.2020.38.170-176
- Buchan
DS, Boddy LM, Young JD, Cooper SM, Noakes TD, Mahoney C et al. Relationships
between cardiorespiratory and muscular fitness with cardiometabolic risk in
adolescents. Res
Sports Med 2015;23(3):227-39. https://doi.org/10.1080/15438627.2015.1040914
- Borfe L, Rech
DC, Benelli TES, Paiva DN, Pohl
HH, Burgos MS. Associação entre a obesidade infantil e a capacidade
cardiorrespiratória: revisão sistemática. Rev
Bras Promoç Saúde
2017;30(1):118-124. https://doi.org/10.5020/18061230.2017.p118
- Eddolls WTB, McNarry MA, Stratton G, Winn CON, Mackintosh KA.
High-intensity interval training interventions in children and adolescents: a
systematic review. Sports Med 2017;47(11):2363-74.
https://doi.org/10.1007/s40279-017-0753-8
- García-Hermoso A, Correa-Bautista JE, Olloquequi
J, Ramírez-Vélez R. Health-related physical fitness
and weight status in 13- to 15-year-old latino
adolescents. A pooled analysis. J Pediatr
2019;95(4):435-42. https://doi.org/10.1016/j.jpedp.2018.04.010
- Twig
G, Reichman B, Afek A, Derazne
E, Hamiel U, Furer A et al.
Severe obesity and cardio-metabolic comorbidities: a nationwide study of 2.8
million adolescents. Int J Obes
2019;43(7):1391-9. https://doi.org/10.1038/s41366-018-0213-z
- Maillard
F, Pereira B, Boisseau N. Effect of high-intensity
interval training on total, abdominal and visceral fat mass: a meta-analysis. Sports Med 2018;48(2):269-88.
https://doi.org/10.1007/s40279-017-0807-y
- Cordel PT, Souza WC,
Lima VA, Hykavei Junior P, Danziato
AVHA, Oliveira VM et al. Comparação da aptidão física relacionada à saúde e a
prática esportiva em crianças. Saúde (Santa Maria) 2018;44(1).
https://doi.org/10.5902/2236583425765
- Bianchini JAA, Silva
DF, Lopera CA, Antonini VDS, Nardo Junior N.
Intervenção multiprofissional melhora a aptidão física relacionada à saúde de
adolescentes com maior efeito sobre as meninas em comparação aos meninos. Rev Bras Educação Física Esporte
2016;30(4):1051-59. https://doi.org/10.1590/1807-55092016000401051
- Weston
KL, Azevedo LB, Bock S, Weston M, George KP, Batterham
AM. Effect of novel, schoolbased high-intensity
interval training on cardiometabolic health in adolescents: Project FFAB (Fun
Fast Activity Blasts) - an exploratory controlled before-and-after trial. PLoS One
2016;11(8):e0159116. https://doi.org/10.1371/journal.pone.0159116
- Rosenblat MA, Perrotta AS, Thomas SG. Effect
of high-intensity interval training versus sprint interval training on
time-trial performance: a systematic review and meta-analysis. Sports Med 2020;50(6):1145-61.
https://doi.org/10.1007/s40279-020-01264-1