Rev Bras Fisiol Exerc. 2024;23:e234417
doi: 10.33233/rbfex.v23i1.4417
ORIGINAL ARTICLE
Impact of active video games on the glycemic
profile and nutritional
status of adolescents
Impacto do videogame
ativo sobre o perfil glicêmico e o estado nutricional de adolescentes
Anna Larissa Veloso
Guimarães, Renata Cardoso Oliveira, Carla Campos Muniz Medeiros, Danielle Franklin de Carvalho
Universidade Estadual da
Paraíba, Campina Grande, PB, Brazil
Received: April 12, 2022; Accepted:
January 23, 2024.
Correspondence: Renata Cardoso Oliveira: renatacardoso09@hotmail.com
How to
cite
Guimarães ALV,
Oliveira RC, Medeiros CCM, Carvalho DF. Impact of
active video games on the glycemic
profile and nutritional
status of overweight adolescents: a controlled intervention study. Rev Bras Fisiol
Exerc. 2024;e234417. doi: 10.33233/rbfex.v23i1.4417
Abstract
Introduction: The interactive game is an intervention proposal to promote
physical activity, especially among young people, to promote
physical activity. Objective:
To test the
hypothesis of the impact of
physical activity using active video
games (AVG) on the glycidic profile of overweight adolescents. Methods: Controlled intervention study carried out in the second half
of 2018. The sample consisted
of 70 overweight adolescents, distributed in control and experimental groups, aged between
10 and 16 years old, enrolled between the 5th and 9th year of education elementary school II of public schools in the city ofCampina
Grande/PB. Sociodemographic, lifestyle,
nutritional status, and biochemical variables were studied and a gamification strategy was adopted. The data were analyzed in
SPSS 22.0 and the chi-suare and paired t-test were performed, adopting a significance
level of 5%. Results: The intervention improved BMI and reduced abdominal adiposity in adolescents but did not cause significant
changes in the glycemic profile. Conclusion:
The use of active video games to increase physical activity in overweight adolescents in an school environment is an effective
tool to improve the nutritional status of adolescents. Interventions with a longer duration
need to be
evaluated to verify possible effects on the
glycemic profile. This is a viable, low-cost
intervention that takes advantage of technological
resources in line with the interests
of the target population.
Keywords: obesity; adolescent; glycemic profile; physical activity.
Resumo
Introdução: O jogo interativo é uma proposta de intervenção, sobretudo
entre o público jovem, na promoção da atividade física. Objetivo: Testar
a hipotese do impacto da atividade física com uso de
videogame ativo sobre o perfil glicêmico de adolescentes com excesso de peso. Métodos:
Estudo de intervenção controlado realizado no segundo
semestre de 2018. A
amostra foi composta por 70 adolescentes com excesso de peso,
distribuídos nos
grupos controle e experimental, com idade entre 10 e 16 anos,
matriculados
entre o 5º e o 9º ano do ensino fundamental II de escolas
públicas do município
de Campina Grande/PB. Foram estudadas variáveis
sociodemográficas, de estilo de
vida, estado nutricional e bioquímicas e adotou-se une
estratégia de gamificação. Os dados foram
analisados no SPSS 22.0
e foram realizados os testes qui-quadrado e t-pareado, adotando-se um
nível de significância de 5%. Resultados: A
intervenção melhorou o IMC e reduziu a adiposidade abdominal dos adolescentes,
mas não causou alterações significativas sobre o perfil glicêmico. Conclusão:
O uso do videogame ativo para aumentar a atividade física em adolescentes com
excesso de peso em ambiente escolar é uma ferramenta eficaz para melhorar o
estado nutricional de adolescentes. Intervenções com maior tempo de duração
necessitam ser avaliadas para verificar os possíveis efeitos no perfil
glicêmico. Está é uma intervenção viável, de baixo custo e aproveita recursos
tecnológicos em sintonia com interesse da população alvo.
Palavras-chave: obesidade; adolescente; perfil
glicêmico; atividade física.
Introduction
Due to the epidemiological changes that have
occurred, it is believed that there
will be a higher percentage of adolescents with high-adiposity than malnourished adolescents in the coming years [1].
Adolescence is considered the most critical period
for obesity occurrence and, consequently, associated problems, as this phase is
characterized by a low level of
physical activity, the development and consolidation of sedentary behaviors,
and changes in body composition. These facts make this period important for carrying out
intervention and prevention measures [2].
Changes caused by physical exercise
are already predicted in the lipid profile [3], blood glucose, blood pressure [4], and inflammation levels assessed by c-reactive
protein (CRP) in obese individuals.
In a randomized clinical trial [5], which evaluated the impact
of one year
of physical exercise on obese
children and adolescents, beneficial changes were found in glycemic
control (fasting blood glucose) in individuals undergoing the proposed intervention.
In this context, it is necessary to
adopt strategies that motivate children
and adolescents to practice physical
activity, such as active games or exergames — technological games (video games) that require the participant's body movements to function
[6].
This study was developed to
test the hypothesis of the
impact of a physical activity intervention using active video games (AVG) on the glycidic
profile of overweight adolescents.
Methods
A controlled gamified intervention study, with two comparison
groups: “control” - with no intervention, and “experimental” - active video game use, three times a week, for 50 minutes, for eight weeks. A hundred twenty-nine (129) eligible individuals with overweight/obesity were initially evaluated; after applying the exclusion
criteria, 105 remained in the study. With
the record of losses and
dropouts (35), 70 adolescents
made up the
final sample. (Figure 1).
Two public schools in the top quartile of students in Campina Grande/PB were drawn. The intervention was allocated per school, one for the intervention and the other for the control, to avoid bias due to contact between the groups. In the urban area of the city, there are 20 municipal schools, of middle school, in the morning and/or afternoon shifts. The population of this study consists of adolescents aged between 10 and 16 years, 11 months and 29 days, overweight or obese, enrolled between the 5th and 9th year of middle school in the selected schools. In each school, all students who met these criteria were invited to participate in the study, respecting the minimum sample size according to the following parameters: average effect size of 0.75, alpha error of 0.05, and power of 80.0%, totaling a minimum of 29 individuals in each group.
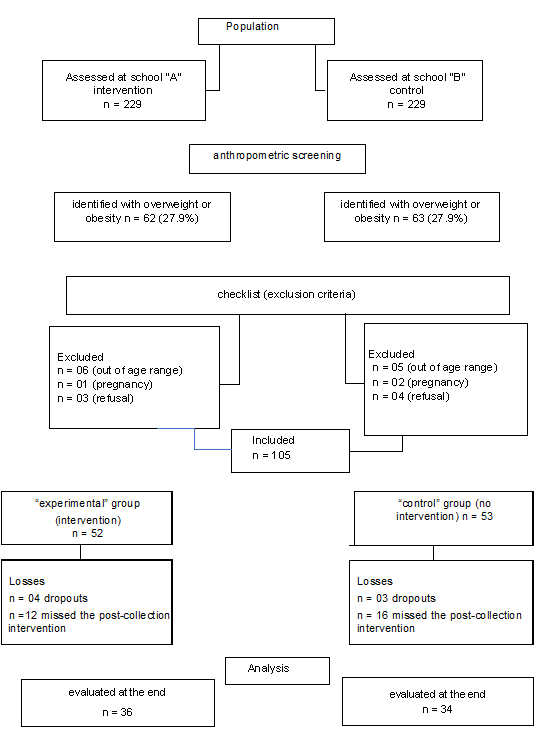
Figure 1 - Flowchart of participants in the study, Campina Grande, PB, 2018
The inclusion criteria used were: adolescents
aged between 10 and 16 years, 11 months and 29 days;
be a student enrolled between the 5th and 9th year of middle
school in the selected schools of Campina Grande/PB; present a nutritional status characterized
as overweight or obesity, according to age and gender,
according to z-score.
Individuals who presented at least
one of the
following situations were excluded from
the study: a condition that did not allow
them to perform
physical activity, such as motor or mental limitations, or diseases in which physical activity could be harmful,
such as exercise-induced bronchospasm and cardiac arrhythmia; patients with hyperthyroidism,
decompensated diabetes mellitus, genetic
syndrome; being on some weight loss treatment; pregnancy, postpartum period or breastfeeding;
active video game user. Cases of individuals who did not collect
blood after the intervention or who gave up
were considered losses.
Variables, procedures and
data collection instruments
Sociodemographic variables (economic class, age, gender, and color), level of physical
activity (active/inactive), nutritional status (overweight or obesity),
and glycidic profile (fasting blood glucose, glycated hemoglobin, and insulin resistance,
using the TyG index) were evaluated. Except for sociodemographic variables, all variables were
evaluated in both groups (experimental and control) before and after the
intervention. Emphasizing that the control
group (without intervention) underwent only blood collections
and questionnaires.
A form was applied
to obtain sociodemographic and lifestyle information. The
assessment of age, gender, and color was based
on criteria from the Brazilian
Institute of Geography and Statistics
[7], the economic class was defined
based on criteria from the
Brazilian Association of Research Companies
[8], and the level of physical
activity was analyzed using the “International Physical Activity Questionnaire” (IPAQ), short version
[9].
Nutritional status was assessed using the body mass index (BMI), constructed from the ratio of
weight (in kg) to the square of
height (in meters), following the recommendations
of the World Health Organization (WHO, 2006), for the
age group, considering: overweight when ≥ +1 BMI
< +2 Z-Score and obesity
when BMI ≥ +2 Z-Score.
Height and weight were measured
in duplicate, considering the average values
of the two
measurements. To measure height, a portable stadiometer, Avanutri® brand, with an accuracy of
0.1 cm, was used; and to identify
the weight, a Tonelli®
digital scale was used, with a capacity
of 150 kg and an accuracy of
0.1 kg. To obtain the measurements, the procedures recommended by the WHO were
followed, and the adolescent had to be
without shoes, accessories, or carrying objects.
Insulin resistance was assessed using
the TyG index calculated from the equation: Tyg
index = [log(fasting triglycerides (mg/dL) x fasting blood glucose (mg/dL)/2. Since there
is no specific cutoff point for insulin resistance by the
TyG index in this age group, the 90th percentile was adopted as a reference, with values equal
to or greater
than it being considered altered [10].
Waist circumference
was measured with the adolescent
in an upright position, with a relaxed abdomen, arms at
their sides, feet together, weight equally supported by both
legs, and breathing normally. The end of the
last rib was located and
marked; then, a measuring tape was positioned horizontally in the midline between
the end of
the last rib and the
iliac crest and maintained so that it remained
in position around the abdomen at the
level of the umbilical scar, allowing the circumference
to be read
to the nearest
millimeter. Values above the 90th percentile were considered increased according to the
International Diabetes Federation (IDF), but with a maximum
limit of 88 cm for girls and 102 for boys, according to the National
Cholesterol Education Program Adult Treatment
Panel III [11].
Abdominal
adiposity was considered present when the waist
circumference/height ratio was ≥ 0.5 [12].
Intervention and gamification
The intervention was carried out with adolescents in the experimental group. They used the active video
game for 50 minutes, 3
times a week, for 8 weeks.
To carry out the intervention, the XBox 360 platform was used, with
the Kinect accessory
(Microsoft®) to enable the user to
control and interact only with
the command of body movements, making them perform physical
activity. Just Dance (2014 to
2018) was the game selected, as in addition to the fact
that most dances can lead teenagers to achieve moderate intensity of physical
activity, it is also reported in the literature [13] as the one that
arouses the greatest interest among teenagers, in addition to allowing the
intervention to be carried out in a group of four adolescents
at the same
time.
The intervention was carried out in reserved rooms at the
selected school, at times available in the morning and
afternoon shifts, and was supervised and controlled. To this end,
the presence of adolescents on the day
of the activity
was recorded, and heart rate was monitored using
a multilaser® Atrio frequency meter before (to calculate training frequency), during (to monitor exercise intensity) and after the activity
(to assess hemodynamic stability). This equipment is a wireless transmitting heart strap to
the wrist heart monitor.
Measurements were obtained during the intervention period to ensure
that exercise was maintained at moderate intensity.
The activities were carried out in sub-groups of up to
four participants, guided and supervised by physical education
professionals, physiotherapists,
master's students, scientific initiation and/or extension
students linked to the project,
all previously trained.
The
dances used for intervention
were previously selected, including those that could
lead to moderate intensity, and gathered in a block of 10 (GBLOCK). This selection was carried
out by physical education students with experience in using this technology
to promote physical activity.
To increase adolescents' engagement in the intervention activity, a gamification strategy was adopted,
with the creation of new blocks of songs
per week and the development of challenges measured
by a properly calibrated team. The group earned points based on criteria
created by the researchers, such as punctuality, group encouragement, posts about the intervention
on social media, and
individual and group
performance (achieving a number
of stars). There were weekly awards
and a final award for the group that
accumulated the most points at the end of
the intervention.
Adolescent adherence was based on
the frequency of attendance at
physical activity sessions, as well as the performance of supervised activity.
In the control group,
measurements were only taken in the
same periods as in the experimental group.
Data analysis
procedures and ethical aspects
The data were double-entered, initially submitted to Epi Info validation, and analyzed in SPSS 22.0. Normality distribution was assessed using
the Kolmogorov-Sminorv
test.
The chi-square test was
applied to carry out a comparative analysis between sociodemographic characteristics
(economic class: C, D, and E; A and B; gender: male and female; color: white and non-white); level of physical
activity: (not active and active);
nutritional status (overweight
and obese); abdominal adiposity (WC/H ≥ 0.5 and
WC/H < 0.5) and glycidic
profile (fasting blood
glucose ≥ 100.0 and < 100.0 mg/dL; glycated hemoglobin
≥ 5.7 and < 5.7 and
insulin resistance ≥
P90 and < P90 of the TyG index) of adolescents in the two comparison
groups at the beginning of
the study. To evaluate the
effect of the intervention on the measurement
of waist circumference in each group, the paired
t-test was used.
The study was developed
in accordance with Resolution 466/2012 of the National Health Council and was
approved by the Research Ethics
Committee, CAAE: 84019518.3.0000.5187. In accordance with WHO recommendations, it was registered in Clinical Trials
(NCT03532659) and REBEC (RBC-2xn3g6).
Results
Seventy (70) adolescents
were evaluated, 36 in the experimental group and 34 in the control
group. The two groups were similar in all characteristics, except gender, as there were more boys in the experimental group compared to the
control. The majority of students were
self-reported non-white
(87%) and belonged to economic classes C, D, or E (68.6%).
Regarding lifestyle,
34.3% declared themselves
as non-active, 40% were obese, and 61.4% had excess abdominal adiposity. None had changes in fasting blood glucose. However, 11.4% of the adolescents showed changes in glycated hemoglobin (Table I).
Table I – Comparison of sociodemographic characteristics related to the practice
of physical activity, nutritional status, and glycidic profile of adolescents from “experimental” and “control” schools at baseline. Campina Grande/PB, 2018
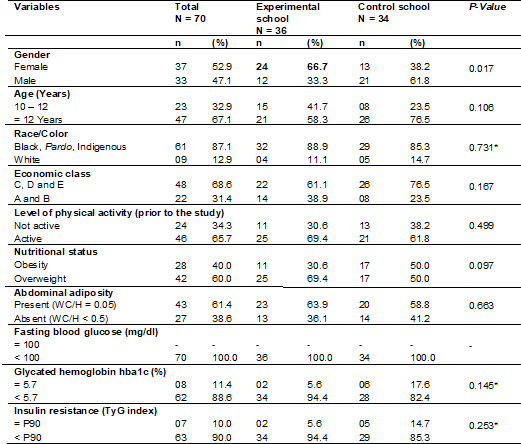
WC/H = waist circumference/height ratio; *Fisher's exact test
At the end of
the intervention, it was found that
the number of adolescents considered physically active increased to 56 (80.0%), although they were not
associated with the group. Regarding
nutritional status, of the total of 42 adolescents who were overweight, eight were classified
as eutrophic, and cases of obesity were
higher in the control school (n = 16; 55.8%).
It was found that insulin resistance
was no longer associated with the group (Table
II).

WC/H = waist circumference/height ratio; *Eight adolescents reached the nutritional
status of eutrophy; **Fisher's exact test
Discussion
In the present study,
it was observed that obesity was
present in 40.0% of them and abdominal adiposity in 61.4%. Although no change in fasting blood glucose was recorded (above 100 mg/dL), there was
an increase in glycated hemoglobin in 11.4% and insulin resistance
in 10.0%. Of the total,
34.3% were classified as
non-active (inactive or irregularly active).
In a study carried out [13] with 54 obese and
overweight adolescents aged between 15 and 19 years, in which a 20-week intervention was carried out to evaluate whether
the exergame would produce weight
loss. It was concluded that the use of active
video games increased significantly caloric expenditure of these adolescents, in addition to promoting weight loss. Likewise,
an active video game intervention was carried out in overweight children for 24 weeks, and a significant
decrease in BMI was observed among participants [14]. A previous study also carried
out with adolescents no
positive effects of AVG on BMI had been
found. The authors attributed the lack of change
in nutritional status to the intervention time, which was considered
short in the 2017 study (12
weeks); however, longer than that
of the present
study, which was eight weeks,
and managed to record a reduction
in BMI and abdominal adiposity
[15].
This reinforces the need to
evaluate body composition since it is already
known that when starting to
practice physical exercise, muscles begin to develop,
which can affect weight [16]. It also highlights the importance of checking the
intensity of the exercise, in addition to the
frequency and duration, as well as other aspects of
the lifestyle, such as food consumption, aspects that can
affect the outcomes in question [17].
Furthermore, unlike the studies mentioned,
the present study was controlled
and supervised so that the
adolescents carried out the intervention in front of one of
the researchers, who applied gamification
techniques (collaboration, encouragement, and carrying out the activity in groups, for example) to ensure moderate
exercise intensity throughout the execution time (50 minutes). In 2012, Staiano
et al. [14] stated that
cooperative games were capable of producing
greater intrinsic motivation and are more often associated with greater energy
expenditure during the game. A systematic review published in 2019 indicated that cooperative games involving exergames were more attractive to overweight children
and adolescents compared to those
with normal weight, generating greater satisfaction, self-efficacy, and positive expectations, which may favor adherence and commitment
among young people [18].
The ability of exergame
to promote an increase in energy expenditure has been described
in the literature [19]. However, its effects on the metabolic
profile require more attention.
Although
diabetes mellitus (DM) mainly affects individuals from the fourth decad
of life onwards, an increase in incidence has been noticed in children
and young people [20]. A study carried out in some
American states between
2002 and 2012 observed an increase of
7% per year in the prevalence of DM in this population [21].
Although the population in this study is young
and considered normoglycemic, the changes observed in glycated hemoglobin and insulin resistance
may already demonstrate changes in glucose metabolism. Furthermore, this is an
overweight population and it is already
well established that obesity is
associated with a multitude
of metabolic and clinical restrictions,
which result in a greater risk of
developing cardiovascular complications
and metabolic diseases, particularly resistance to insulin
and type 2 diabetes [21].
Methodological differences, especially regarding the method adopted
and the cutoff
points for diagnosing IR using
the TyG index, make it difficult to compare previously published results. One of
the possibilities for not having observed
an impact of the intervention
on the glycidic
profile is that this is an
initially normoglycemic population, and fasting blood glucose is used to
calculate the TyG index, adopted to assess insulin
resistance. The values of triglycerides are also included in the calculation of this index, which can be
reduced during exercise but increase
again immediately after the so-called
“detraining” so that these possible
fluctuations can end up interfering
with the values of the
TyG index [21].
After the intervention with AVG, it was observed that
there was a reduction in AC. This result is similar to that found
in a study [22] in Turkey, which analyzed 50 overweight or obese
adolescents. After an exercise program
using the AVG over 8 weeks, participants' AC values decreased significantly.
Some studies have been
carried out to evaluate the effectiveness
of AVG in combating obesity in children and adolescents [23]. In an experimental study [24] carried out in New Zealand with
20 adolescents, the effects of AVG on the anthropometric
profile and level of physical activity
were evaluated over 12 weeks. After the
intervention, the group showed higher
levels of physical activity and decreased body weight and waist
circumference, corroborating
the results of the present
study.
The use of AVG as an innovative
tool for controlling childhood
obesity has been observed by
health professionals since the benefits
include adherence and increased levels of physical activity,
reduced consumption of low-nutrition foods, and increased
energy expenditure, with direct repercussions on the main
comorbidities associated with childhood obesity [25].
Conclusion
In this study, active
video games did not cause a reduction in glycemic values in overweight and obese adolescents. However, we observed
a reduction in body mass
index and abdominal adiposity
in the sample that played the active
video game. Therefore, the use of active video
games to increase physical activity in adolescents with obesity or overweight
in a school environment can be an
effective tool for a better
lifestyle and changing sedentary habits.
Academic affiliation
Article from
the Master's Thesis by: Anna Larissa Veloso
Guimarães, Master's in Public
Health, State University of Paraíba, 2020.
Conflicts of
interest
There is
no conflict of interest
Funding sources
Ministry of
Science, Technology and Innovation.
Authors' contributions
Conception and
design of the research: Guimarães ALV, Carvalho DF; Data collect:
Guimarães ALV, Carvalho D; Data analysis and interpretation: Guimarães
ALV, Carvalho DF; Manuscript writing: Guimarães ALV, Carvalho DF, Oliveira RC; Critical
review of the manuscript for important intellectual content:
Guimarães ALV, Carvalho DF, Oliveira RC
References
- World Health Organization. (WHO) OMS, OPAS. Obesidade entre crianças e
adolescentes aumentou dez vezes em quatro décadas, revela novo estudo do
Imperial College London e da OMS [internet]. [citado
2020 ago 16]. Disponível em:
https://www.paho.org/braobesidade-entre-criancas-e-adolescentes-aumentou-dez-vezes-em-quatro-decadas-revela-novo-estudo-do-imperial
college-london-e-da-oms
- Alberga AS, Sigal RJ, Goldfield G, Prud HD, KGP. Overweight and obese teenagers: why is adolescence a critical period? Pediatric Obesity.
2012;7(4):261–73. doi: 10.1111/j.2047-6310.2011.00046.x [Crossref]
- Prado ES, Dantas EHM. Efeitos dos exercícios físicos aeróbio e de força nas lipoproteínas HDL, LDL e Lipoproteína(a). Arq Bras Cardiol. 2002;79(4);429-33. doi: 10.1590/S0066-782X2002001300013 [Crossref]
- Oka R, Yagi K, Sakurai M, Nakamura K, Nagasawa
S, Miyamoto S, Nohara A, Kawashiri
M, Hayashi M, Takeda O, Yamagishi M. Impact of visceral adipose tissue and subcutaneous
adipose tissue on insulin resistance in middle-aged japanese. J Atheroscler Thromb.
2012;19(1);814–22. doi: 10.5551/jat.12294 [Crossref]
- Blüher S, Panagiotou
G, Petroff D, Markert J,
Wagner A, Klemm T, et al. Effects
of a 1-year exercise and lifestyle intervention
on irisin, adipokines, and inflammatory markers in obese children. Obesity. 2014;22(7):1701–8. doi: 10.1002/oby.20739 [Crossref]
- Biddiss E, Irwin J. Active video
games to promote physical activity in children and youth.
Arch Periatr Adolesc Med.
2010;164(7);664-72. doi: 10.1001/archpediatrics.2010.104 [Crossref]
- Instituto Brasileiro de
Geografia e Estatística - IBGE [Internet]. Indicadores Sociodemográficos e de
Saúde no Brasil | 2009 [Internet]. [citado 2020 ago
12]. Disponível em:
https://www.ibge.gov.br/estatisticas/sociais/populacao/9336-indicadores
sociodemograficos-e-de-saude-no-brasil.html
- ABEP. Associação Brasileira
de Empresas de Pesquisa. Critério de Classificação Econômica Brasil [Internet].
[citado 2020 ago 12]; Disponível em:
https://www.abep.org/criterio-brasil
- Saucedo MT, Jiménez JR, Macías LAO, Castillo
MV, Hernández RCL, Cortés TLF. Relacion entre el índice de masa corporal, la actividad fisica
y los tiempos de comida en adolescentes mexicanos. Nutr
Hosp. 2015 [citado 2020 ago 12];32(3);1082–90.
Disponível em: http://www.aulamedica.es/nh/pdf/9331.pdf
- American Diabetes Association. 2: Classification and diagnosis of diabetes. Diabetes Care. 2019;42(Suppl1):S13-28. doi: 10.2337/dc19-S002 [Crossref]
- National Cholesterol Education Program Adult Treatment Pannel III (NCEP-ATPIII, 2001). J Manag Care Pharm. 2003;9(Suppl1):2-5. doi: 10.18553/jmcp.2003.9.s1.2 [Crossref]
- Brasil. Ministério da Saúde.
Agência Nacional de Saúde Suplementar. Vigitel Brasil
2015 – Vigilância de fatores de risco e proteção de doenças crônicas por
inquérito telefônico. Brasília: Ministério da Saúde.; 2017. 173p.
- Jelsma D, Geuze RH, Mombarg R, Smits EBC. The impact of Wii Fit intervention on dynamic balance control in children with probable
Developmental Coordination Disorder and balance problems. Hum Mov Sci. 2014;33:404-18. doi: 10.1016/j.humov.2013.12.007 [Crossref]
- Staiano AE, Abraham AA, Calvert SL. Motivating effects of cooperative exergame play for overweight and obese adolescents. J Diabetes Sci Technol. 2012;6(4):812-9. doi: 10.1177/193229681200600412 [Crossref]
- Christison AL, Evans TA, Bleess
BB, Wang H, Aldag JC, Binns
HJ. Exergaming for health:
a randomized study of community-based exergaming curriculum in pediatric
weight management. Games for Health Journal. 2016;5(6);413–21. doi: 10.1089/g4h.2015.0097 [Crossref]
- Silva MM, Carvalho RSM, Freitas MB. Bioimpedância para avaliação da composição corporal: uma proposta didático-experimental para estudantes da área da saúde. Revista Brasileira de Ensino de Física. 2019;2:e20180271. doi: 10.1590/1806-9126-RBEF-2018-0271 [Crossref]
- Staiano AE, Beyl RA, Guan W, Hendrick CA, Hsia DS, Newton RLJR. Home-based exergaming among children with overweight and obesity: a randomized clinical trial. Pediatr Obes. 2018;13(11);724-33. doi: 10.1111/ijpo.12438 [Crossref]
- Kumar S, Kaufman T. Childhood obesity. Panminerva Med. 2018; 60(4);200-12. doi: 10.23736/S0031-0808.18.03557-7 [Crossref]
- Kracht CL, Joseph ED, Staiano
AE. Video Games, obesity, and children. Curr
Obes Rep. 2020;9(1):1-14. doi: 10.1007/s13679-020-00368-z [Crossref]
- Andrade A, Correia CK, Coimbra DR. The psychological effects of exergames for children and adolescents with obesity: a systematic review and meta- analysis. Cyberpsychol Behav Soc Netw. 2019;22(11);724-35. doi: 10.1089/cyber.2019.0341 [Crossref]
- Pereira JC, Rodrigues ME,
Campos HO, Amorin PRDS. Exergames como alternativa
para o aumento do dispêndio energético: uma revisão sistemática. Revista
Brasileira de Atividade Física e Saúde. 2012;17(5):332-40. doi: 10.12820/rbafs.v.17n5p332-340 [Crossref]
- Mayer DEJ, Lawrence JM, Dabelea D, Divers J, Isom S, Dolan
L, et al. Incidence trends of
type 1 and type 2 diabetes among youths, 2002-2012. New Eng J Med.
2017;376(15):1419-29. doi: 10.1056/NEJMoa1610187 [Crossref]
- García HA, Carmona LMI, Saavedra JM, Escalante Y. Physical exercise, detraining and lipid profile in obese children: a systematic review. Arch Argent Pediatr. 2014;112(6):519-25. doi: 10.5546/aap.2014.519 [Crossref]
- Duman F, Kokacya MH, Dogru E, Katayifci N, Canbay O, Aman F. The role of active video-accompanied exercises in improvement of the obese state in children: a prospective study from Turkey. J Clin Peditr Endocrinal. 2016;8(3):334-34. doi: 10.4274/jcrpe.2284 [Crossref]
- Gao Z, Chen S. Arefield-based exergames useful in preventing childhood obesity? A systematic review. Obesity Reviews. 2014;15(8):676-91. doi: 10.1111/obr.12164 [Crossref]
