Rev Bras Fisiol Exerc 2021;20(6):655-64
doi: 10.33233/rbfex.v20i6.4727
REVIEW
Benefit of
physical exercise programs for patients with permanent atrial fibrillation: A
systematic review with meta-analysis
Benefício de programas de exercício
físico para pacientes com fibrilação atrial permanente: Uma revisão sistemática
com metanálise
Angela Couto1, Áquilla
Couto2, Rodrigo Pereira3, Dilmar
P. Guedes3, Fabrício Madureira3, Claudio Scorcine3,4
1Hospital Ana Costa, Santos, SP, Brazil
2Universidade Federal de São Paulo, São
Paulo, SP, Brazil
3Universidade Metropolitana de Santos,
Santos, SP, Brazil
4Universidade do Oeste Paulista, Guarujá,
SP, Brazil
Received: April 13,
2021; Accepted: August 29, 2021.
Correspondence: Angela
Couto, Rua Tocantins 77, 11055-341 Santos SP
Angela Couto:
angelaa_couto@hotmail.com
Áquilla Couto:
aquillacouto@gmail.com
Rodrigo Pereira:
r.pereirads@hotmail.com
Dilmar P. Guedes:
dilmarpintoguedesjr@gmail.com
Fabrício Madureira:
shark_jaws@hotmail.com
Claudio
Scorcine: claudio-scorcine@uol.com.br
Abstract
Objective: The
aim of the present study was to highlight the effects of physical exercise for
patients with permanent atrial fibrillation trough a systematic review with
meta-analysis. Methods: A search was performed in the main academic
literature databases using the descriptors related to permanent atrial
fibrillation and physical exercise. After reviewing the articles, four
randomized clinical trial papers and a cross-over trial were selected for this
review. Results: The analyzed works evidenced the safety and the
benefits of different physical exercise programs on patients’ mobility and
quality of life with atrial fibrillation. Conclusion: The programs of
exercise proved to be safe and beneficial in the mobility and quality of life
of patients with permanent atrial fibrillation, since the literature showed
that drug therapies no longer aim at cardiac control at the stage of the
disease.
Keywords:
atrial fibrillation; exercise; quality of life.
Resumo
Objetivo: Evidenciar os efeitos do exercício
físico para pacientes com fibrilação atrial permanente através de uma revisão
sistemática com metanálise. Métodos: Foi
realizada uma busca nos principais bancos de dados da literatura acadêmica
utilizando os descritores relacionados a fibrilação atrial permanente e
exercício físico. Após a revisão dos artigos, foram selecionados quatro trabalhos
de ensaio clínico randomizado e um ensaio de cross-over
para esta revisão. Resultados: Os trabalhos analisados evidenciaram a
segurança e os benefícios de diferentes programas de exercício físico na
mobilidade e qualidade de vida dos pacientes com fibrilação atrial. Conclusão:
O exercício físico é uma forma de terapêutica não medicamentosa que
potencializa a mobilidade e qualidade de vida dos pacientes com fibrilação
atrial permanente, uma vez que a literatura sugere que as terapêuticas
medicamentosas não objetivam mais o controle cardíaco nessa fase da doença.
Palavras-chave: fibrilação atrial; exercício físico;
qualidade de vida.
Introduction
Atrial
fibrillation (AF) is the most common cardiac arrhythmia. Its incidence
increases with age and has significant associations with morbidity and
mortality [1]. This arrhythmia happens when there are electrophysiological
abnormalities in atrial tissue, favoring the formation of unbalanced electrical
impulse [2]. In this condition, the atriums lose their command capacity and,
consequently, the atrial systole occurs chaotically and irregular [3]. The
symptoms of this arrhythmia are associated with the heartbeat, which can reach
175 bpm at rest. The patient may experience dizziness, sweating, chest pressure,
dyspnea, tiredness and syncope [4]. The cause of this disease is still unknown,
although some factors can contribute to its development, for example: age,
uncontrolled hypertension, diabetes, previous heart attack, coronary diseases
and severe heart failure [5].
Its
prevalence is 2%, with a high incidence in the population over 70 years old
[6]. Projections for 2050 suggest that more than 50% of individuals over 80
years will present atrial fibrillation [7]. The morbidity of patients with
atrial fibrillation is not just related to cardiovascular outcomes. Others
comorbidities as cancer, sepsis, chronic obstructive pulmonary disease, sleep
apnea and chronic renal failure are also related with atrial fibrillation [8].
Cumulative
hospital’s costs were considerably high; however, this difference loses meaning
during the years, possibly due to the number of deaths. The mortality is
significantly higher in patients with AF when compared to those without the
disease, regardless of age [9]. In addition, the occurrence of a stroke is
increased in five times in patients with this disease [10].
Atrial
fibrillation can be classified in five ways: first time diagnosed (not diagnose
previously regardless of the duration of the disease); paroxysmal AF (also
known as intermittent, with sporadic episodes); persistent AF (it last more
than seven days and it is not solved without pharmacological treatment);
longstanding persistent AF (continuous form, it last more than a year,
interventions are taken to control the rhythm); permanent AF (it represents a
therapeutic attitude, in which doctor and patient decide that the interventions
to control the rhythm should stop) [4]. Specifically, permanent AF is one of
the most severe forms of the disease. Individuals that present this type of AF
usually do not tolerate physical effort, leading to a decrease in activities of
daily life. Therefore, less global physical activity and lower overall quality
of life [11].
One
of the proven ways to increase day-to-day physical effort tolerance is training
through physical exercise [12]. Thereby, a patient who does not tolerate a
minimum effort to perform the daily life actions begins to perform them more
efficiently due to the increased tolerance to physical effort [13]. There is a
vast literature on the benefits of regular physical exercise in order to
attenuate the risks of comorbidities that can potentialize the development of
AF [14]. Among the protective factors, physical exercise is able to minimize
the chance of developing obesity [15], diabetes, hypertension [16],
atherosclerosis [17], acute myocardial infarction [18].
For
these benefits to be achieved, the American College of Sports Medicine
recommends a minimum of 150 minutes per week of moderate activities or 75
minutes per week of intense physical exercise [19]. On the other hand,
sedentary lifestyle predisposes the individual to a series of factors related
to the decrease in quality of life through lower functional capacity [20]. The
decrease in functional capacity is linked to a lower ability to move and
perform activities of daily living, making these people dependent on others
[21,22].
Physical
exercises for patients already diagnosed with AF promotes benefits as the
increase in the amount of walking footage in the six-minute walk tests, the
improvement in muscle power [23] and in the quality of life [24]. Even though
researches indicate that physical exercise can improve functional capabilities
and life’s quality of patients with permanent AF, a systematic review with
meta-analysis can direct the professionals’ intervention in relation to the
safety and efficiency of training.
Thereby
the objective of the present study was to elaborate a systematic review with
meta-analysis about the effects of physical exercise in patients with permanent
atrial fibrillation.
Methods
This
study is a systematic review with meta-analysis conducted from the checklist
Prisma (Prospero CRD42021248139). For a complete coverage about the subject,
databases were analyzed: Medline via Pubmed, Lilacs,
Cochrane e Academic Google. The descriptors used were “atrium fibrillation”,
“permanent atrium fibrillation”, “six-minute walk test”, “exercise”, “cardiac
rehabilitation”. The search contemplated articles in English and Portuguese
from 2000 to 2021. Two experienced researchers assisted by a librarian
experienced in systematic reviews performed data collection.
Only
original articles of randomized clinical trials were included in the review.
165 articles were identified using the first criteria. Of these articles, 42
were excluded for duplication in databases. Of the remaining 123 articles, 23
were excluded for not meeting the original article criteria (n = 13 reviews; n
= 2 case studies; n = 8 articles written in other languages; n = 3 researches
performed on animals). From the 97 articles selected after this filtering,
titles and abstracts were analyzed and 92 articles were excluded (n = 26
patients with other comorbidities; n = 61 with no physical activity intervention;
n = 5 non-randomized studies). According to the eligibility criteria, four
randomized articles and one-crossover articles with patients with permanent AF
who experienced physical exercise intervention to improve their functional
capacity and/or quality of life.
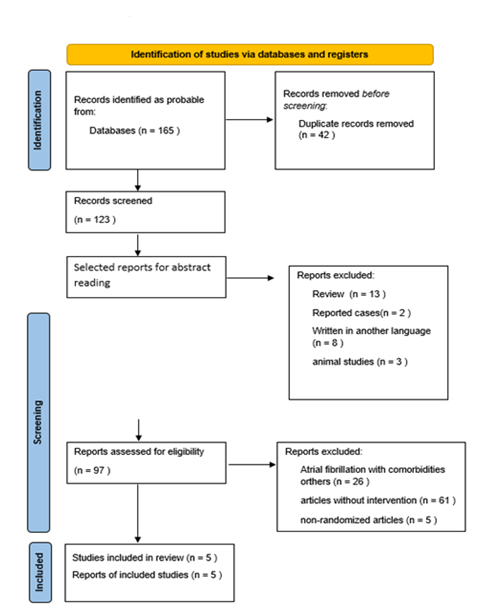
Figure 1 – Selection
of articles included in the systematic review
All
the selected articles were analyzed and carefully reviewed to data extractions
(figure 1). To evaluate the risk of publication bias, the Cochrane Risk of Bias
Tool model was used (figure 2). For statistical analysis was used measures of
effect size (Cohen d). For the creation of the Forest Plot, the variables
present in three or more articles were used (six-minute walk test). The adopted
effect size stratification was 0.2 for small effects; 0.5 moderate effects and
0.8 for large effects.
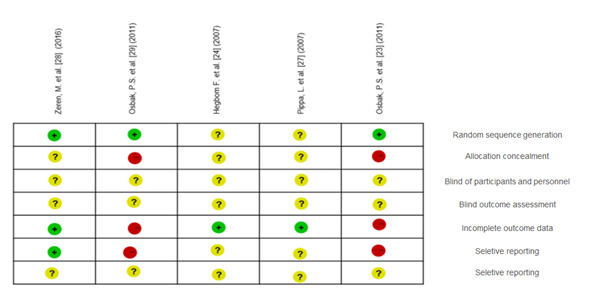
Figure 2 - Cochrane
Risk of Bias Tool
Results
Five
articles were selected to the results of this systematic review, three articles
for analyze meta-analysis that evaluated mobility through the walk test and two
that evaluated the levels of quality of life through the SF-36 questionnaire.
Table I - Description
of the studies included in the analysis of statistical data and/or
meta-analysis that contains exercise intervention in patients with permanent
atrial fibrillation
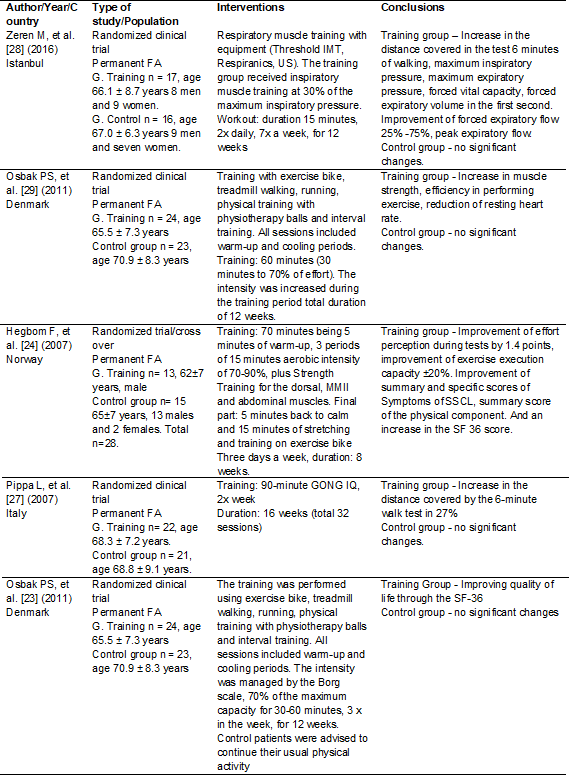
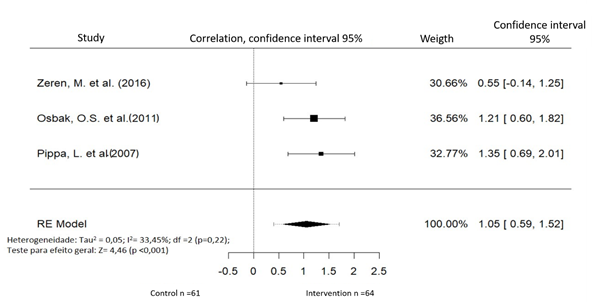
Figure 3 - Forest
Plot Graph comparing the control and training groups in the variable distance
of the six-minute walk test
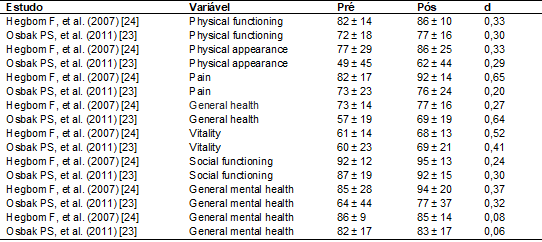
Table II -
Quality of life indexes measured using the SF-36 questionnaire stratified in
eight distinct domains in the two studies statistically analyzed. The data are
expressed in the form of mean and standard deviation and the size of effect
through the Cohen d (d).
Discussion
The
results of the present review suggest that physical training can be an
efficient strategy to improve the mobility of patients with AF. However, this
fact should be considered with caution, as consistent studies specifically
related to the topic are scarce. Systematized and well-oriented physical
exercise can be an efficient strategy to improve the physiological parameters
of these patients. The therapeutic recommendation suggested by the national
guidelines for atrial fibrillation in patients with permanent AF does not
include the attempt to change the patients' heart rate. Therefore, therapies
that can enhance greater tolerance to small efforts, such as activities of
daily living, can significantly change the quality of life of these patients.
The
results of this study about the significant improvement in mobility in the
six-minute test demonstrate that patients are capable to better tolerate
efforts when they are physically active [23,25,26,27,28].
In a
pilot study performed in 2007, the researchers found that after 12 weeks of
training the heart beats at rest significantly decreased and the patients with
permanent AF increased their tolerance to physical effort and improved the life
quality scores [25]. Physical exercise can significantly improve the
chronotropic and inotropic function of the heart [29]. Therefore, physical
exercise is an effective, low-cost form that has the potential to improve the
functional capacity of these patients.
In
relation to quality of life, it is usually measured subjectively, through
instruments that measure the perception of the interviewed individuals about
different parameters. The two studies that investigated this variable
demonstrated a positive fact size (mild to moderate) for all the domains
related to life quality.
Therefore,
despite little evidence, it is possible to suggest that physical exercise can
alter the patients' perception of effort on these parameters [24,30]. The
physical exercise considered efficient and safe to this population is of
moderate intensity (60-70% of the peak VO2) with duration of 20-60 minutes per
training session at least three sessions per week [19,26].
These
recommendations aim to achieve all the goals that the physical exercise can
potentialize in this population, among these: reduction of pressure levels,
blood glucose control, improvement in cardiac function, mainly due to changes
in the left ventricle, decrease in fat percentage, improvement of physical,
functional abilities and stress levels.
Conclusion
The
results of this review allow us to infer that physical exercise significantly
and positively can alter the functional capacities of patients with permanent AF.
However, the data must be viewed with caution due to the paucity of
high-quality evidence.
Academic
affiliation
This
article represents a scientific initiation by Angela Couto, a resident
physician at Hospital Ana Costa, supervised by Professor Dr. Claudio Scorcine at the Metropolitan University of Santos.
Conflict
of interests
The
authors of this study have no conflicts of interest related to the theme,
development and publication of this article.
Financing
source
Not
applicable.
Authors'
contribution
Conception
and design of the research: Couto A, Pereira R; Data
retrieval: Couto A, Couto A; Data analysis and interpretation: Scorcine C; Statistical analysis: Scorcine C; Writing of the manuscript: Scorcine C, Couto A. Critical review of the manuscript
for important intellectual content: Madureira F,
Guedes DP.
References
- Santos EB, Salles ALF, Tavares LR, Lima MV, Santos WB,
Silva GP, et al. Características clínicas e demográficas e perfil terapêutico
de pacientes hospitalizados com fibrilação atrial: Estudo EPIFA. Rev
SOCERJ [Internet]. 2009 [cited 2021 Nov 17];22(1):9-14. Available from:
http://sociedades.cardiol.br/socerj/revista/2009_01/a2009_v22_n01_a01eduarda.pdf
- Guyton AC, Hall JE, Zocchi
L, Aicardi G. Fisiologia médica. Madrid: Elsevier;
2017.
- Cintra FD, Figueiredo MJO. Fibrilação atrial (Parte 1):
fisiopatologia, fatores de risco e bases terapêuticas. Arq
Bras Cardiol
2021;116(1):129-39. doi: 10.36660/abc.20200485 [Crossref]
- Magalhães L, Figueiredo M, Cintra F, Saad E, Kuniyoshi R, Teixeira R, et al. II Diretrizes brasileiras
de fibrilação atrial. Arq Bras
Cardiol 2016;106(4):1-22. doi: 10.5935/abc.20160055 [Crossref]
- Benjamin EJ, Levy D, Vaziri SM, D'Agostino RB, Belanger AJ, Wolf PA. Independent risk factors for atrial fibrillation in a population-based cohort: the Framingham Heart Study. Jama 1994;271(11):840-4. doi: 10.1001/jama.1994.03510350050036 [Crossref]
- Wilke T, Groth A, Mueller S, Pfannkuche M, Verheyen F, Linder R, et al. Incidence and prevalence of atrial fibrillation: an analysis based on 8.3 million patients. Europace 2012;15(4):486-93. doi: 10.1093/europace/eus333 [Crossref]
- Go AS, Hylek EM,
Phillips KA, Chang Y, Henault LE, Selby JV, et al. Prevalence of
diagnosed atrial fibrillation in adults: national implications for rhythm
management and stroke prevention: the AnTicoagulation and Risk Factors in Atrial Fibrillation
(ATRIA) Study. Jama 2001;285(18):2370-5. doi: 10.1001/jama.285.18.2370 [Crossref]
- Ferreira C, Providência R, Ferreira M, Gonçalves L. Fibrilação atrial e doenças não cardiovasculares: uma revisão sistemática. Arq Bras Cardiol 2015;105(5):519-26. doi: 10.5935/abc.20150142 [Crossref]
- Wolf PA,
Mitchell JB, Baker CS, Kannel WB, D'Agostino RB.
Impact of atrial fibrillation on mortality, stroke, and medical costs. Arch Intern Med 1998;158(3):229-34. doi: 10.1001/archinte.158.20.2265 [Crossref]
- Marianelli M, Marianelli
C, Lacerda Neto TP. Principais fatores de risco do avc
isquêmico: Uma abordagem descritiva. Braz J Health Review 2020;3(6):19679-90. doi: 10.22533/at.ed.07621090215 [Crossref]
- Saad EB, d’Avila A. Fibrilação
atrial (parte 2) Ablação por cateter. Arq Bras Cardiol 2021;116(2):334-43. doi: 10.36660/abc.20200477 [Crossref]
- Oliveira JC, Vinhas W, Rabello LG. Benefícios do exercício físico regular para idosos. Braz J Development 2020;6(3):15496-504. doi: 10.34117/bjdv6n3-429 [Crossref]
- Couto LHN. Comparação da autonomia funcional de idosos
praticantes e não praticantes de atividades físicas [TCC] [Internet]. Cruz
Alta: Universidade de Cruz Alta; 2018. [cited 2021 Nov 17]. Available from:
https://home.unicruz.edu.br/wp-content/uploads/2019/02/COMPARA%C3%87%C3%83O-DA-AUTONOMIA-FUNCIONAL-DE-IDOSOS-PRATICANTES-E-N%C3%83O-PRATICANTES-DE-ATIVIDADES-F%C3%8DSICAS.pdf
- Kesaniemi YA,
Danforth E, Jensen MD, Kopelman PG, Lefèbvre P,
Reeder BA. Dose-response issues concerning physical activity and health: an
evidence-based symposium. Med
Sci Sports Exerc
2001;33(6):S351-S8. doi: 10.1037/e603442007-001 [Crossref]
- Jesus LAS, Gravina EPL, Neto MNF,
Miguel CRCE, Ribeiro JR, Talma AJM, et al. Exercício
físico e obesidade: prescrição e benefícios. HU Rev
2018:269-76. doi: 10.34019/1982-8047.2018.v44.13953 [Crossref]
- Maia RHS, Navarro AC. O exercício físico leve a moderado
como tratamento da obesidade, hipertensão e diabetes. Revista Brasileira de
Obesidade, Nutrição e Emagrecimento [Internet]. 2017 [cited
2021 Dec 23];11(66):393-402. Available from: http://www.rbone.com.br/index.php/rbone/article/view/535
- Gonçalves MPM, Anjos JC, Lemos ACG, Gonçalves RD, Silva VN.
Nutrição e exercício físico como forma de prevenção ou regressão da
aterosclerose. Revista Saúde UniToledo [Internet] 2017
[cited 2021 Nov 17];1(1). Available from:
http://www.ojs.toledo.br/index.php/saude/article/view/26
- Costa FC, Silva AFT, Macedo BFS, Silva GVN, Silva TMMF,
Brito MVH. Efeitos do exercício físico na prevenção e tratamento de lesões por
isquemia: uma revisão de literatura. Rev Med 2020;99(5):480-90. doi: 10.11606/issn.1679-9836.v99i5p480-490 [Crossref]
- Morey MC.
Physical activity and exercise in older adults. UpToDate, Waltham;
2019. doi: 10.1093/oxfordhb/9780195394313.013.0018 [Crossref]
- Ribeiro DBG, Silva ASC, Ferreira GLS. Análise da capacidade
funcional em idosas praticantes de hidroginástica. Braz J Developm
2020;6(5):27206-11. doi: 10.34117/bjdv6n5-246 [Crossref]
- Oliveira DV, Nascimento J, Lima MCC, Leme DEC, Antunes MD, Bertolini S. Capacidade funcional e qualidade de vida em mulheres idosas praticantes e não praticantes de hidroginástica. Rev Rene 2017;18(2):156-63. doi: 10.15253/2175-6783.2017000200003 [Crossref]
- Lozado YA, Barbosa RS, Silva Caires S, Bomfim
BSM, dos Santos L. Implicações do elevado comportamento sedentário à saúde de
idosos: uma revisão de literatura. Práticas e cuidado. Rev
Saúde Coletiva 2020;1:e9994-e.
https://www.revistas.uneb.br/index.php/saudecoletiva/article/view/9994
- Osbak PS,
Mourier M, Henriksen JH, Kofoed KF, Jensen GB. Effect
of physical exercise training on muscle strength and body composition, and
their association with functional capacity and quality of life in patients with
atrial fibrillation: a randomized controlled trial. J Rehabil
Med 2012;44(11):975-9. doi: 10.2340/16501977-1039 [Crossref]
- Hegbom F, Stavem K, Sire S, Heldal M, Orning OM, Gjesdal K. Effects of short-term exercise training on symptoms and quality of life in patients with chronic atrial fibrillation. Int J Cardiol 2007;116(1):86-92. doi: 10.1016/j.ijcard.2006.03.034 [Crossref]
- Plisiene J,
Blumberg A, Haager G, Knackstedt
C, Latsch J, Norra C, et
al. Moderate physical exercise: a simplified approach for ventricular rate
control in older patients with atrial fibrillation. Clin Res Cardiol
2008;97(11):820-6. doi: 10.1007/s00392-008-0692-3 [Crossref]
- Giacomantonio NB,
Bredin SS, Foulds HJ, Warburton DE. A systematic
review of the health benefits of exercise rehabilitation in persons living with
atrial fibrillation. Can J Cardiol 2013;29(4):483-91. doi: 10.1016/j.cjca.2012.07.003 [Crossref]
- Pippa L, Manzoli L, Corti I, Congedo G, Romanazzi L, Parruti G. Functional capacity after traditional Chinese
medicine (qi gong) training in patients with chronic atrial fibrillation: a
randomized controlled trial. Prev Cardiol
2007;10(1):22-5. doi: 10.1111/j.1520-037x.2007.05721.x [Crossref]
- Zeren M, Demir
R, Yigit Z, Gurses HN.
Effects of inspiratory muscle training on pulmonary function, respiratory
muscle strength and functional capacity in patients with atrial fibrillation: a
randomized controlled trial. Clin Rehabil
2016;30(12):1165-74. doi: 10.1177/0269215515628038 [Crossref]
- Santos M, West E, Skali H, Forman DE, Junior WN, Shah AM. Resting heart rate and chronotropic response to exercise: Prognostic implications in heart failure across the left ventricular ejection fraction spectrum. J Card Fail 2018;24(11):753-62. doi: 10.1016/j.cardfail.2018.09.015 [Crossref]
- Osbak PS, Mourier M, Kjaer A, Henriksen JH, Kofoed KF, Jensen GB. A randomized study of the effects of exercise training on patients with atrial fibrillation. Am Heart J 2011;162(6):1080-7. doi: 10.1016/j.ahj.2011.09.013 [Crossref]
