Rev Bras Fisiol Exerc 2021;20(5):542-51
doi: 10.33233/rbfex.v20i5.4824
ORIGINAL ARTICLE
Cardiorespiratory fitness during cardiopulmonary
exercise testing in individuals with unilateral lower limb amputation
Aptidão
cardiorrespiratória durante o teste cardiopulmonar de esforço de indivíduos com
amputação unilateral de membro inferior
Roberto
Miranda Ramos Costa1, Patrícia Marques Aroso
Lisboa de Castro1, Mauro Augusto dos Santos2,3, Míriam
Raquel Meira Mainenti4, Agnaldo José Lopes1, Patrícia dos
Santos Vigário1
1Centro Universitário Augusto Motta
(UNISUAM), Rio de Janeiro, Brazil
2Instituto Nacional de Cardiologia (INC),
Rio de Janeiro, Brazil
3ACE Cardiologia do Exercício, Rio de
Janeiro, Brazil
4Escola de Educação Física do Exército (EsEFEx), Rio de Janeiro, Brazil
Received:
June 24, 2021; Accepted: September 29, 2021.
Correspondence: Prof. Dr. Patrícia dos Santos Vigário, Programa de
Pós-graduação em Ciências da Reabilitação, Centro Universitário Augusto Motta
(PPGCR/UNISUAM), Rua Dona Isabel, 94 Bonsucesso 21041-020 Rio de Janeiro RJ.
patriciavigario@yahoo.com.br
Roberto Miranda Ramos Costa: betomrcosta@hotmail.com
Patrícia Marques Aroso Lisboa de
Castro: patimarques13@yahoo.com.br
Mauro Augusto dos Santos: msaugusto@terra.com.br
Míriam Raquel Meira Mainenti: miriam.mainenti@hotmail.com
Agnaldo José Lopes: agnaldolopes.uerj@gmail.com
Patrícia dos Santos Vigário: patriciavigario@yahoo.com.br
Abstract
Introduction: The lower limb
amputation impacts the mobility of individuals, which can lead to low
cardiorespiratory fitness. Maximum oxygen consumption (VO2max) is
traditionally used to describe cardiorespiratory fitness. However, its
achievement is not always feasible in populations with functional limitations
and, therefore, analysis at submaximal levels of effort can be an efficient
strategy. Objective: To test the hypothesis that individuals with
unilateral lower limb amputation have lower cardiorespiratory fitness at
different effort intensities compared to individuals without amputation. Methods:
Cross-sectional study with 6 individuals with lower limb amputation and 10
individuals without amputation. Cardiorespiratory fitness was investigated by
the cardiopulmonary exercise test, considering absolute and relative VO2peak,
ventilatory threshold 1 (VT1) and Optimal Cardiorespiratory Point (POC). Results:
The amputees had lower absolute and relative VO2peak than
non-amputates. The absolute value of POC, time and load did not differ between
groups, but the group with amputation presented the POC in a higher percentage
of VO2peak (p = 0.007) and in a lower relative and absolute VO2
(p = 0.004 and p = 0.009, respectively). In LV1, there was no difference
between groups in time, load and percentage of VO2peak,
however amputees had lower relative and absolute VO2 (p = 0.046 and
p = 0.032, respectively). Conclusion: Individuals with lower limb
amputation had lower cardiorespiratory fitness at different effort intensities
when compared to individuals without amputation, but they had the highest
efficiency between the respiratory and circulatory systems in a higher
%VO2peak.
Keywords: disabled persons; oxygen
consumption; rehabilitation.
Resumo
Introdução: A amputação de membros inferiores
impacta na mobilidade dos indivíduos, podendo levar a uma baixa aptidão
cardiorrespiratória. O consumo máximo de oxigênio (VO2máx)
é
tradicionalmente utilizado para descrever a aptidão
cardiorrespiratória.
Contudo, a sua obtenção nem sempre é viável
em populações com limitações funcionais
e, por isso, análises em níveis submáximos de
esforço podem ser uma estratégia
eficiente. Objetivo: Testar a hipótese de que indivíduos com amputação
unilateral de membro inferior possuem aptidão cardiorrespiratória menor em
diferentes intensidades de esforço comparados a indivíduos sem amputação. Métodos:
Estudo seccional com 6 indivíduos com amputação de membro inferior e 10
indivíduos sem amputação. A aptidão cardiorrespiratória foi investigada pelo
teste de esforço cardiopulmonar, sendo considerados: VO2pico
absoluto e relativo, limiar ventilatório 1 (LV1) e Ponto Ótimo
Cardiorrespiratório (POC). Resultados: Os indivíduos amputados
apresentaram menor VO2pico absoluto e relativo que os não amputados.
O valor absoluto do POC, o tempo e a carga, não se diferiram entre os grupos,
porém o grupo com amputação apresentou o POC em um maior percentual do VO2pico
(p = 0,007) e em um menor VO2 relativo e absoluto (p = 0,004 e p =
0,009, respectivamente). No LV1, não houve diferença entre os grupos no tempo,
carga e percentual do VO2pico, contudo os amputados apresentaram
menor VO2 relativo e absoluto (p = 0,046 e p = 0,032,
respectivamente). Conclusão: Indivíduos com amputação de membro inferior
apresentaram menor aptidão cardiorrespiratória em diferentes intensidades de
esforço quando comparados com indivíduos sem amputação, porém apresentaram a
maior eficiência entre os sistemas respiratório e circulatório em um maior %VO2pico.
Palavras-chave: pessoa com deficiência; consumo de
oxigênio; reabilitação.
Introduction
Amputation of
lower limbs has clinical and functional problems that negatively affect
mobility [1]. Impaired mobility associated or not with the inadaptation of
prostheses and orthotics, and the reduced number of equipment and accessible spaces
for physical exercise contribute to inadequate daily physical activity levels
in the population of individuals with amputation. Other factors that contribute
to this process are emotional problems such as low self-esteem, self-image, and
self-confidence [2,3]. In this context, it is known that one of the main
problems related to a sedentary lifestyle is the increased risk of
cardiovascular morbidity and mortality [4], as individuals with amputations
naturally already present this increased risk [5].
On the other
hand, good cardiorespiratory fitness is associated with better general health
status, with the direct measure of maximum oxygen consumption (VO2max) being
the gold standard for its quantification. The VO2max is an important
predictor of mortality [6,7], and its achievement depends on the performance of
a maximum effort. However, in individuals with functional limitations, this
level of intensity is not always reached, with the effort being commonly
interrupted by peripheral factors [8] and limiting the interpretation and
application of results. In situations like this, oxygen consumption at peak
effort (VO2peak) is used.
To minimize this
problem, Ramos et al. [9] proposed the Cardiorespiratory Optimal Point
(COP), the lowest value of the ventilatory equivalent of oxygen during
exertion. Reflects the ventilatory economy for obtaining oxygen to meet the
metabolic demands of active muscles during exercise. The analysis of COP has
already been described in the population of non-athlete men and women, without
obesity and cardiorespiratory diseases [9], and professional adult soccer
players [10]. But interestingly, in searches previously carried out in the
scientific databases PubMed/Medline and SciELO, no
evidence was found about its application in populations with physical
limitations, particularly in individuals with amputation.
Physical-motor
disability is the second most prevalent in Brazil [11]. Considering the
negative repercussions on general health status related to low energy
expenditure commonly described in individuals with amputations [2], strategies
and measures must be taken to promote an active lifestyle in this group. In
this context, knowing the cardiorespiratory fitness of people with amputation
is relevant, as professionals who deal directly with this audience need to know
the characteristics and physiological demands to plan and prescribe exercises
properly. Understanding that the maximum effort in individuals with functional
limitations is not always reached, the use of COP can be a good strategy since
its analysis is performed at submaximal intensities. The study of COP in
individuals with an amputation will be an original approach in the scientific
literature and may provide support for further studies in this area of knowledge.
In this sense, this study aims to test the hypothesis that individuals with unilateral
lower limb amputation have lower cardiorespiratory fitness at different effort
intensities compared to individuals without amputation.
Methods
Study design and sample
A comparative
observational cross-sectional study was carried out with 16 individuals divided
into two groups: with amputation (N = 6) and without amputation (N = 10). The
amputated group was composed of men aged 18 years or over, with unilateral
transtibial or transfemoral amputation and physically active (all recreational paracanoe
practitioners, with a minimum time of three months). The sample was selected
for convenience because it was all participants in a sports project of the
modality in Rio de Janeiro, Brazil. Information related to the amputation of
the participants is described in Table I. Smokers and individuals with
musculoskeletal limitations that could make it impossible to carry out the
protocol were excluded from the study. For comparison purposes, a group of
individuals without amputation was also considered respecting the same
inclusion and exclusion criteria, except for amputation and the practice of
paracanoeing. The physical activity level in the non-amputee group was
investigated by completing the International Physical Activity Questionnaire
(IPAQ) short version [12], including individuals classified as “active” or
“very active” who practice aerobic and strength training. The outcome variables
considered for the cardiorespiratory fitness assessment were VO2peak,
ventilatory threshold 1 (VT1), and COP.
Table I - Variables
related to the amputation of each participant

The study was
submitted and approved by the institutional Research Ethics Committee (CAAE:
17691113.1.0000.5235), and all participants signed an informed consent form to
participate in the study.
Cardiopulmonary exercise testing
The
cardiopulmonary exercise test (CPET) was performed in a cycle ergometer for
upper limbs (TopExcite; TechnoGym;
Italy) in an environment with controlled temperature (≈22oC)
and humidity (≈60%) [13]. The protocol adopted was an initial load of
20w and successive increments of 5w every minute, with cycling between 50-60
rpm [14]. Participants were verbally encouraged to perform maximum effort, and
CPET was interrupted by maximum voluntary exhaustion or upon the appearance of
some criterion under recommendations proposed by the American College of Sports
Medicine [15].
During CPET, the
metabolic analysis of respiratory gases was performed using a gas analyzer
(VO2000; MedGraphics; Brazil), in which the readings
of pulmonary ventilation (VE; L/min) and the expired fractions of oxygen (FeO2;
%) and carbon dioxide (FeCO2; %) were taken to calculate the
ventilatory variables: relative and absolute oxygen consumption (VO2;
mL.kg-1.min-1 and L/min, respectively) and ventilatory
equivalents of oxygen (VE/VO2) and carbon dioxide (VE/VCO2).
The information was recorded breath-by-breath and analyzed as a mean of 30
seconds. For standardization purposes, the highest value presented in the curve
in the last minute of the test was considered as VO2peak.
Ventilatory threshold 1 - VT1
To determine
VT1, we opted for the graphic inspection of the behavior of ventilatory
equivalents - VE/VO2 and VE/VCO2. VT1 was defined as the
point on the curve at which there was an increase in the VE/VO2
curve without the concomitant increase in VE/VCO2 [16]. The analysis
of VT1 was performed independently by two experienced evaluators, and then the
evaluators' agreement in each test was verified. In case of disagreement, a third
evaluator was consulted.
Cardiorespiratory Optimal Point (COP)
COP was defined
as the lowest value on the VE/VO2 curve during exercise, as
described by Ramos et al. [9]. In addition to the absolute value of
VE/VO2, the VO2 value (in mL.kg-1.min-1,
in L/min, and as a percentage in relation to the peak), the load (w), and the
time of effort (min:s)
referring to the moment of identification of the COP.
Statistical procedures
The results were
described as median (minimum value-maximum value). Given the sample size of the
study subgroups, we chose to use a non-parametric statistical procedure for
comparisons between subgroups. Thus, the Mann-Whitney test was applied
considering the level of statistical significance of 5%. Analyzes were performed
using the Statistical Package for Social Sciences (SPSS 20.0) (Armonk, NY:
International Business Machines Corporation).
Results
The groups of
individuals with amputation (N = 6) and without amputation (N = 10) were
comparable in terms of age, total body mass, Body Mass Index, and weekly
frequency of physical exercise (Table II) and statistically different regarding
the time of physical exercise practice.
Table II - Demographic,
anthropometric and physical exercise characteristics of the study subgroups
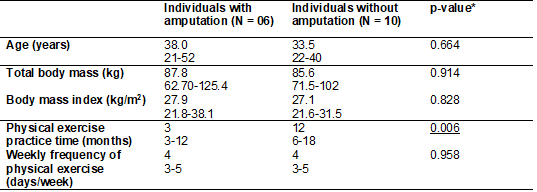
Data presented as
average (minimum value – maximum value); *Mann-Whitney test; statistical
significance when p-value < 0.05
The results
regarding exercise cardiorespiratory capacity are shown in Table III. At the
end of the exercise, the groups presented similar total time and total effort
load (p = 0.386 and p = 0.785, respectively). When analyzing the VO2peak, we
noticed a higher median value among individuals without amputation, both in
absolute and relative to body mass analysis. All study participants, regardless
of the group, reported peripheral fatigue (upper limbs) as a reason for effort
interruption.
The absolute
value of COP, time, and load at the time of occurrence did not differ between
groups (p = 0.786; p = 0.212 and p = 0.240, respectively), but individuals with
amputation presented this point at a higher percentage of VO2peak (p
= 0.007) and in a lower relative and absolute VO2 (p = 0.004 and p =
0.009, respectively). In both groups, COP preceded the occurrence of VT1.
VT1 was
identified in all participants in the amputee group, while in the non-amputated
group, in 70%. There was no difference between the groups about time and load
at the time of reaching VT1 (p = 0.253 and p = 0.170, respectively) and
percentage of VO2peak (p = 0.568). However, amputees had lower
relative and absolute VO2 at this time (p = 0.046 and p = 0.032,
respectively).
Table III - Variables
related to the cardiopulmonary exercise test of the study subgroups
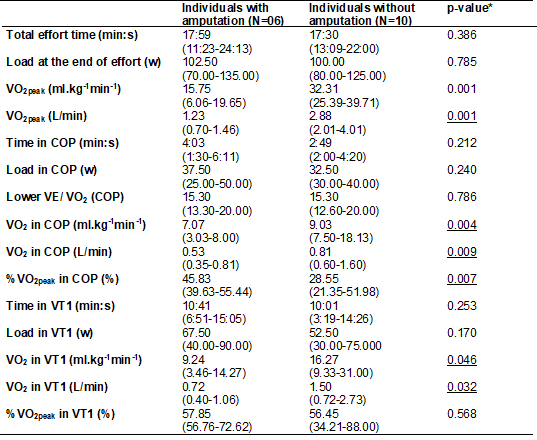
COP = Cardiorespiratory Optimal Point; VT1 = Ventilatory threshold 1; *Mann-Whitney test; statistical significance = 5%.
Data presented as (minimum value – maximum value);
*Mann-Whitney test; statistical significance when p-value < 0.05
Discussion
The present
study aimed to test the hypothesis that individuals with unilateral lower limb
amputation have lower cardiorespiratory fitness at different effort intensities
compared to individuals without amputation. The main findings were that the
group with amputation had lower VO2peak for the same effort intensity when
compared to the group without amputation, as well as the VO2 at submaximal
effort intensities, that is, in COP and VT1. However, the amputated group
reached COP and VT1 in percentage values of VO2peak similar to the group without amputation.
The VO2max
is the variable that best represents the aerobic capacity of an individual,
with higher values being associated with a lower risk of fatal and non-fatal
cardiovascular events [6,7]. In the present study, in the two investigated
groups, none of the participants reached VO2max. This may be related
to the type of ergometer used, which, among other factors, influences the
maximum metabolic response [17,18]. Particularly about the cycle ergometer for
upper limbs, it is known that 1) it mobilizes a smaller amount of muscle groups
when compared to other ergometers such as the treadmill and the ergometric bicycle;
and 2) the gestures of movement are less familiar than the gestures in the
ergometers mentioned above, in addition to not being muscle groups commonly
used in daily activities, a fact that can facilitate the interruption of the
test due to peripheral muscle fatigue. All study participants reported upper
limb fatigue as the main cause for cessation of exertion. These factors, taken
together, may have contributed to achieving VO2peak instead of VO2max.
Regarding VO2peak,
it was observed that individuals with amputation had a median value
approximately 50% lower than individuals without amputation, reflecting lower
integrity of the respiratory, circulatory, and muscle systems, determinants of
cardiorespiratory fitness [16]. This difference was noticed both in the
absolute analysis, in L/min, and in the body mass (mL.kg-1.min-1). To achieve
the same intensity at the end of the effort, amputees probably resorted to a
higher percentage of contribution of the glycolytic anaerobic system for the
generation of ATP since the aerobic system did not rise as much as the
non-amputee group. It is known that variables such as age, level of daily
physical activity, and body size influence VO2max [8]. Even if
amputees practiced physical exercises recreationally on average three times a
week, it is believed that in their daily lives, due to the lower mobility
commonly caused by the removal of the limb, these individuals have a lower
energy expenditure, leading to lower fitness cardiorespiratory when compared
with congeners without amputation. Recently, a study including the
participation of 72 individuals with lower-limb amputations – mostly men, with
amputation at the transtibial level, and with a mean age of 53.6 years – showed
that 61% of the participants did not have enough physical activity daily to be
classified as sufficiently active, and 33% was classified as sedentary [3].
Considering the
submaximal effort intensities, this study considered the following moments: 1)
COP and 2) VT1. COP was first described in 2012 by a team of Brazilian
researchers [9], following the assessment of healthy men and women on a
treadmill. The authors noted that COP was achieved, on average, at 44% of VO2max
and before VT1. In professional soccer players, the COP was reached between
48.4% and 57% of the VO2max, this variation being related to the position on
the field – particularly the goalkeepers reached the COP in a higher percentage
of the VO2max and a lower VO2max [10]. In the present
study, amputees achieved COP in a higher % of VO2peak compared to
non-amputates (median amputees’ group = 45.83; non-amputates = 28.55), with
values like those described by Ramos et al. [9], which averaged 44%.
However, even if there was a difference, the two groups reached the COP in a %
of the VO2peak close to what is reported in the literature, that is,
between 30 and 50% [9].
COP values lower
than 22, assessed through the effort performed on a cycle ergometer for lower
limbs by healthy individuals and with chronic diseases, were associated with a
lower risk of mortality [19]. Taking this value alone as a reference, we could
suggest amputees would have a good clinical prognosis (median COP = 15.30;
lowest value = 13.3; highest value = 20.0). However, this result must be
interpreted with caution considering the following issues: 1) metabolic
adjustments during physical effort are dependent, among others, on the
ergometer and the exercise protocol. Therefore, there may be differences
between the COP obtained in efforts performed with the upper and lower limbs,
reflecting the number of mobilized muscle groups and differences in fiber types
[8] and 2) the group had low VO2peak, which is indicative of low
cardiorespiratory fitness. Ramos and Araújo [19] evaluated maximal
cardiorespiratory capacity on a cycle ergometer for lower limbs in 3331 adults
with and without chronic diseases. Through the combination of COP [stratified
at < 22 (low), 22-30 (medium) and > 30 (high)] and VO2max
[stratified at < 15.75 (low); 15.76-30 (medium) and > 30 (high)
ml.kg-1min-1] it was found through the analysis of the Kaplan-Meier survival
curve, that regardless of the COP classification (low, medium or high), when in
the presence of a low VO2max, the risk of death is greater (the
higher the COP and the lower the VO2max, the greater the mortality).
Another approach
that highlights the lower cardiorespiratory fitness in amputees is related to
VT1. VT1 represents the moment of effort when the transition from aerobic to
anaerobic metabolism begins. From this moment on, exercise ceases to be almost
exclusively aerobic and starts to have an increase in the contribution of
anaerobic mechanisms in the energy production process [8]. Progressive efforts
performed above VT1 are associated with decreased effort tolerance [20].
In the present
study, as much as amputees have reached VT1 in a percentage of VO2peak within
the expected range for the healthy population, that is, 50-60% [21] and similar to the non-amputee group, this percentage does not
match a good cardiorespiratory fitness to the group given the VO2
value at the time of VT1 (almost 50% lower than the non-amputee group). It can
be suggested that although amputees have low cardiorespiratory fitness, it
seems that they have a similar tolerance to non-amputates about the onset of
the metabolism transition.
The present
study has as a limitation the small sample size, which may limit the inference
of the findings. However, as far as the authors are aware, this is the first
approach involving the assessment of exercise-cardiorespiratory fitness in
individuals with lower-limb amputations at different intensities. Specifically,
this is the first investigation of COP in this population: a variable that
reflects the efficiency of the integration between the cardiovascular and
respiratory systems and with good applicability in populations that present
functional limitations that prevent reaching maximum effort [9].
Whereas lower
limb amputation is related to less participation in physical activities for reasons
ranging from lack of accessibility, materials (prostheses and orthotics) and
emotional issues such as problems with self-esteem, self-image,
self-confidence, and motivation [22], knowledge of the cardiorespiratory
fitness of individuals with amputation becomes necessary and relevant in the
context of rehabilitation. The use of VO2peak, VT1, and COP as a
basis for exercise prescription allows stimuli to be effectively individualized
according to demands and physiological conditions, a fact that will favor the
occurrence of more consistent chronic adaptations.
As future
perspectives, studies are expected to be carried out involving, among others:
1) larger sample size to increase the power of inferences; 2) the population of
women since metabolic responses differ according to sex; 3) the creation of
cut-off points for COP classification involving a cycle ergometer for upper
limbs.
Conclusion
Individuals with
unilateral lower limb amputation have lower cardiorespiratory fitness at
different effort intensities when compared to individuals without amputation.
Conflict of interests
All authors declare no
conflict of interest.
Contribution of each
author
Conception and research
design: Costa RMR, Vigário PS, Mainenti
MRM; Data collection: Costa RMR, Castro PMLA; Data analysis and interpretation:
Vigário PS, Mainenti MRM,
Santos MA; Statistical analysis: Vigário PS, Mainenti MRM; Funding: Vigário
PS; Writing of the manuscript: Costa RMR, Vigário PS,
Mainenti MRM, Castro PMLA; Critical review of the
manuscript for important intellectual content: Lopes AJ, Santos MA.
Financing source
This study was
partially funded by the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior - Brasil (CAPES,
Coordination for the Improvement of Higher Education Personnel) - Funding Code
001, by the Fundação de Amparo à Pesquisa
do Estado do Rio de Janeiro (FAPERJ, Foundation for Research Support of the
State of Rio de Janeiro) (public notice E-26/203.256/2017) and by the Conselho Nacional de Desenvolvimento
Científico e Tecnológico (CNPq, National Council for Scientific and Technological
Development). The authors also thank the Brazilian Paralympic Academy, of the
Brazilian Paralympic Committee (BPA/BPC), for its scientific support.
References
- Esfandiari E, Yavari A, Karimi A, Masoumi
M, Soroush M, Saeedi H. Long-term symptoms
and function after war-related lower limb amputation: A national
cross-sectional study. Acta Orthop Traumatol Turc 2018;52(5):348–51. doi: 10.1016/j.aott.2017.04.00 [Crossref]
- Rimmer JH, Schiller W, Chen MD. Effects of disability-associated low energy expenditure deconditioning syndrome. Exerc Sport Sci Rev 2012;40(1):22-9. doi: 10.1097/JES.0b013e31823b8b82 [Crossref]
- Langford J, Dillon MP, Granger CL, Barr C. Physical activity participation amongst individuals with lower limb amputation. Disabil Rehabil 2019;41(9):1063–70. doi: 10.1080/09638288.2017.1422031 [Crossref]
- Mok A, Khaw KT, Luben R, Wareham N,
Brage S. Physical activity trajectories and mortality: population
based cohort study. BMJ 2019;365:l2323. doi: /10.1136/bmj.l2323 [Crossref]
- Mundell BF, Luetmer MT, Kremers HM, Visscher S, Hoppe KM, Kaufman KR. The risk of major cardiovascular events for adults with transfemoral amputation. J Neuroeng Rehabil 2018;15(1):58. doi: 10.1186/s12984-018-0400-0 [Crossref]
- Khan H, Kunutsor S, Rauramaa R, Savonen K, Kalogeropoulos AP, Georgiopoulou VV, et al. Cardiorespiratory fitness and risk of heart failure: A population-based follow-up study. Eur J Heart Fail 2014;16(2):180-8. doi: 10.1111/ejhf.37 [Crossref]
- Kunutsor SK, Kurl S, Khan H, Zaccardi F, Laukkanen JA. Associations of cardiovascular and all-cause mortality events with oxygen uptake at ventilatory threshold. Int J Cardiol 2017;1(236):444-50. doi: 10.1016/j.ijcard.2017.01.156 [Crossref]
- American Thoracic Society; American College of Chest
Physicians. ATS/ACCP Statement on cardiopulmonary exercise testing. Am J Respir
Crit Care Med 2003;167(2):211-77. doi: 10.1164/rccm.167.2.211 [Crossref] Erratum in: Am J Respir Crit Care Med 2003 May
15;1451-2.
- Ramos PS, Ricardo DR, Araújo CGS. Cardiorespiratory optimal point: A submaximal variable of the Cardiopulmonary Exercise Testing. Arq Bras Cardiol 2012;99(5):988-96. doi: /10.1371/journal.pone.0104932 [Crossref]
- Silva CGS, Castro CLB, Franca JF, Bottino A, Myers J, Araújo CGS. Ponto ótimo cardiorrespiratório em futebolistas profissionais: uma nova variável submáxima do exercício. Int J Cardiovasc Sci 2018;31(4):323-32. doi: 10.5935/2359-4802.20180030 [Crossref]
- IBGE.
Censo demográfico: 2010: características gerais da população, religião e
pessoas com deficiência [Internet]. Rio de Janeiro, 2012. [cited
2021 Sept 29]. Available from:
https://biblioteca.ibge.gov.br/visualizacao/periodicos/94/cd_2010_religiao_deficiencia.pdf
- Matsudo S, Araújo T, Matsudo V, Andrade D, Andrade E, Oliveira LC, et al. Questionário internacional de atividade física (IPAQ): estudo de validade e reprodutibilidade no Brasil. Rev Bras Ativ Fís Saúde 2012;6(2):5-18. doi: 10.12820/rbafs.v.6n2p5-18 [Crossref]
- Yazbek PJ, Carvalho RT, Sabbag LMS, Battistella LR. Ergoespirometria. Teste de Esforço Cardiopulmonar, Metodologia e Interpretação. Arq Bras Cardiol 1998;71(5):719-24. doi: 10.1590/s0066-782x1998001100014 [Crossref]
- Campos
LFCC. Comparação entre métodos para mensuração da potência aeróbia em atletas
tetraplégicos [Dissertação]. São Paulo: Faculdade de Educação Física da
UNICAMP; 2013.
- ACSM.
Diretrizes do ACSM para os testes de esforço e sua prescrição. 10 ed. Rio de
Janeiro: Guanabara Koogan; 2018.
- Wasserman K. The anaerobic threshold measurement to evaluate exercise performance. Am Rev Respir Dis;129(2 Pt 2):S35-40. doi: /10.1164/arrd.1984.129.2P2.S35 [Crossref]
- Miranda EF, Malaguti C, Corso SD. Peripheral muscle dysfunction in COPD: lower limbs versus upper limbs. J Bras Pneumol 2011;37(3):380-8. doi: 10.1590/s1806-37132011000300016 [Crossref]
- Wasserman K, Hansen J, Sue DY, Casaburi
R, Whipp B. Principles of exercise testing and
interpretation. 3 ed. Baltimore: Lippincott, Williams & Wilkins; 1999.
- Ramos PS, Araújo CGS. Cardiorespiratory optimal point during exercise testing as a predictor of all-cause mortality. Rev Port Cardiol 2017;36(4):261-9. doi: 10.1016/j.repce.2016.09.011 [Crossref]
- Sullivan MJL, Bishop SR, Pivik J. The Pain catastrophizing scale: development and validation. Psychol Assess 1995;4(7):524-32. doi: /10.1037/1040-3590.7.4.524 [Crossref]
- Roca J, Whipp BJ, Agustí AGN, Anderson SD, Casaburi R, Cotes JE, et al. Clinical exercise testing with reference to lung diseases: Indications, standardization and interpretation strategies. Eur Respir J 1997;10(11):2662-89. doi: 10.1183/09031936.97.10112662 [Crossref]
- Miller MJ, Jones J, Anderson CB, Christiansen CL. Factors influencing participation in physical activity after dysvascular amputation: a qualitative meta-synthesis. Disabil Rehabil 2019;41(26):3141-50. doi: 10.1080/09638288.2018.1492031 [Crossref]