Rev Bras Fisiol Exerc 2021;20(5):562-73
doi: 10.33233/rbfex.v20i5.4877
REVIEW
Acute inflammatory responses to flexibility training:
a systematic review
Respostas
inflamatórias agudas ao treinamento de flexibilidade: uma revisão sistemática
Carlos
José Nogueira1,2,3, Andrea Dos Santos Garcia3, Isabelle
Vasconcellos de Souza1, Antônio Carlos Leal Cortez1,3,4,
Gilmar Weber Senna1,3,5, Paula Paraguassu Brandão3, Estélio Henrique Martin Dantas1,3
1Universidade Federal do Estado do Rio de
Janeiro (UNIRIO), Rio de Janeiro, RJ, Brazil
2Força Aérea Brasileira (FAB), Escola
Preparatória de Cadetes do Ar (EPCAR), Barbacena, MG, Brazil
3Universidade Tiradentes (UNIT), Aracaju,
SE, Brazil
4Centro Universitário Santo Agostinho
(UNIFSA), Teresina, PI, Brazil
5Universidade Católica de Petrópolis,
Petrópolis, RJ, Brazil
Received:
August 10, 2021; Accepted: September
30, 2021.
Correspondence: Carlos José Nogueira, Universidade Federal do Estado do Rio
de Janeiro (UNIRIO), Laboratório de Biociências da Motricidade Humana (LABIMH),
Rua Dr. Xavier Sigaud, 290 / Sala 301, Praia
Vermelha, Rio de Janeiro RJ
Andrea dos Santos Garcia: andrea-sgarcia@hotmail.com
Isabelle Vasconcelos de Souza: isav2206@gmail.com
Antônio Carlos Leal Cortez: antoniocarloscortez@hotmail.com
Gilmar Weber Senna: gilmar.senna@ucp.br
Paula Paraguassu Brandão: pb.paula@yahoo.com.br
Estélio Henrique Martin Dantas:
estelio@pesquisador.cnpq.br
Abstract
Objective: The aim of the study was to
systematically assess the scientific evidence available on the effectiveness
and safety of flexibility training at different intensities in terms of acute
inflammatory responses in adult men. Methods: A search was conducted in
the Medline/PubMed, Cochrane Library, Web of Science and Scopus databases and a
manual search in the reference lists of relevant studies. The research question
and strategy used were based on the PICO model. Included were studies involving
adults aged between 18 and 45 years, published in English, Spanish and
Portuguese, with no restriction for year of publication. Results: A
total of 1014 articles were initially recovered. After duplicates were
eliminated, 655 references were analyzed by title and abstract, 16 of which
were included for reading in their entirety. After this stage, 13 references
were excluded. At the end, three studies were considered eligible. Conclusion:
The evidence available suggests that stretching exercises maximum in
combination with non-habitual eccentric exercise or applied alone, are
associated with a possible acute inflammatory response. Based on the evidence
and the quality of the articles included in this review, the results should be
interpreted with caution. Future research with better methodological quality
involving the variables studied may better explain the results obtained to
date.
Keywords: exercises; muscle stretching exercises; flexibility; inflammation.
Resumo
Objetivo: O objetivo do estudo foi avaliar
sistematicamente as evidências científicas disponíveis sobre a eficácia e
segurança do treinamento de flexibilidade em diferentes intensidades sobre as
respostas inflamatórias agudas em homens adultos. Métodos: Foi realizada
uma busca nas bases de dados Medline/PubMed, Cochrane
Library, Web of Science e Scopus e uma busca manual
nas listas de referências de estudos relevantes. A questão de pesquisa e a
estratégia utilizadas foram baseadas no modelo PICO. Foram incluídos estudos
envolvendo adultos com idade entre 18 e 45 anos, publicados nos idiomas inglês,
espanhol e português, sem restrição de ano de publicação. Resultados: Um
total de 1.014 artigos foram recuperados inicialmente. Após a eliminação das
duplicatas, foram analisadas 655 referências por título e resumo, das quais 16
foram incluídas para leitura na íntegra. Após essa etapa, 13 referências foram
excluídas. Ao final, 3 estudos foram considerados elegíveis. Conclusão:
As evidências disponíveis sugerem que exercícios de alongamento máximo em
combinação com exercícios excêntricos não habituais ou aplicados isoladamente
estão associados a uma possível resposta inflamatória aguda. Com base nas
evidências e na qualidade dos artigos incluídos nesta revisão, os resultados
devem ser interpretados com cautela. Pesquisas futuras com melhor qualidade
metodológica envolvendo as variáveis estudadas podem explicar melhor os
resultados obtidos até o momento.
Palavras-chave: exercícios; exercícios de alongamento
muscular; flexibilidade; inflamação.
Introduction
Flexibility
training is considered a form of physical activity used by athletes, patients
in rehabilitation and individuals engaged in physical activities [1]. Control
of flexible training intensities enables differentiating between submaximal
(stretching) and maximal (flexibilizing) exercises,
which is essential to good physical planning and preparation [2,3].
Movement in
submaximal stretching occurs within the normal joint range, slightly sustained,
without pain or discomfort; in stretching exercises maximum, the muscle is
stretched to the point of discomfort, a little before the pain threshold [4,5].
According to Behm et al. [6], four main stretching exercises
techniques can be applied: static, dynamic, ballistic, and proprioceptive
neuromuscular facilitation (PNF). The static technique involves a continuous
controlled movement for the range of final motion of a single or multiple
joints actively contracting the agonist muscles (active static) or using
external forces such as gravity, a partner or stretching aids (passive static).
In the final position, the individual maintains the muscle in a stretched
position for a certain time [6].
The magnitude of
the moment of force (or torque) that will be applied to a joint or set of joints
during flexibility training is characterized as intensity, while the number of
sets and time are the dimensions of volume [7]. Special importance should be
attributed to training intensity, since a small moment of force may result in a
viscoelastic response of the locomotor apparatus with little or no gain in
range of motion. However, applying excessive force may compromise the tissue,
resulting in inflammation or even injury [7,8].
An experiment
with adult male mice reported high neutrophil levels after passive stretching
exercises maximum protocol, exhibiting an acute inflammatory response, given
that activated neutrophils secrete proinflammatory cytokines such as
interleukin 1 beta (IL-1b),
tumor necrosis factor alpha (TNF-α) and interleukin 6 (IL-6) [9]. This
inflammatory response to training plays an essential role in energy metabolism,
skeletal muscle repair and remodeling, and anabolic/catabolic response, and may
respond differently according to exercise type, intensity, volume, and recovery
between the exercise phases [10].
Thus, different
substrates of the inflammatory response are produced and secreted, such as
cytokines, which belong to a group of regulatory glycoproteins produced by
leukocytes and tissues such as the skeletal muscles [11] and are responsible
for the interconnections between immunological cells as a response to infection
or tissue damage, with possible proinflammatory and anti-inflammatory activity
[12,13].
Evidences on
the inflammatory responses caused by flexibility training are scarce in the
literature. This hampers a better understanding of the physiological mechanisms
of adaptation resulting from alterations in this methodological training
variable and the monitoring of adaptive responses to establish a balance
between the overload applied and recovery [14].
Thus,
investigating the inflammation resulting from flexibility training may
complement the information presented by traditional tissue injury markers
already evident in the literature, such as creatine kinase (CK) or
delayed-onset muscle soreness (DOMS) [15].
Therefore, the
aim of the present review was to systematically assess and summarize the
scientific evidence available regarding the effectiveness and safety of
flexibility training at different intensities (maximal and submaximal) on acute
inflammatory responses in adult men.
Methods
The systematic
search in the literature was conducted in line with the guidelines of the
PRISMA Statement reports for systematic reviews and meta-analysis [16] and the
Cochrane Handbook for Systematic Reviews of Interventions [17]. The current
review was registered at the International Prospective Register of Systematic
Reviews (PROSPERO), under protocol number 42020165515, and entitled “Acute
inflammatory responses to stretching”.
Search strategy
A search was
conducted in the following electronic databases: Medical Literature Analysis
and Retrieval System Online (Medline, via PubMed), Cochrane Library, Web of
Science and Scopus. The search strategies created and used for the databases
are presented in Table I. A manual search was carried out in the reference
lists of the relevant studies to identify eligible articles not found in the
electronic search. The searches were performed in June 2020 and update in July
2021.
The
following descriptors were selected in the Descritores
em Ciências da Saúde (DeCS) and Medical Subject
Headings (MeSH) databases: homens
(men), adulto (adult), exercícios
de alongamento muscular (muscle stretching
exercises), amplitude de movimento articular (joint
range of motion), inflamação (inflammation), citocinas (cytokines), biomarcadores
(biomarkers), as described and presented along with the search strategy used in
Medline via Pubmed and adapted to other databases
(Chart 1).
Chart 1 - Strategies
used for electronic searches
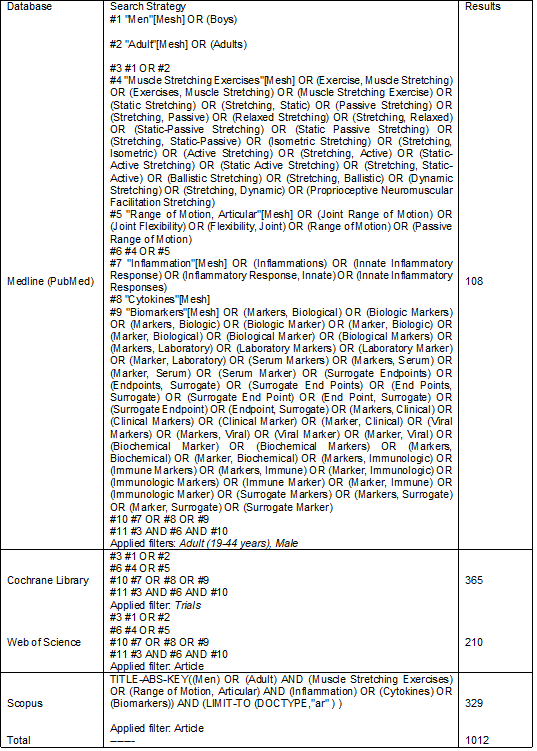
Source: Author 2020
Research question
The research
question and strategy used in this study were based on the Population,
Intervention, Comparison, Outcome (PICO) model, commonly applied in
evidence-based practice and recommended for systematic reviews [18].
Thus, adult men,
trained or not in flexibility, were used as the “Population”; for Intervention,
studies involving different intensities of flexibility training were
considered, for Control, the “not applicable” criterion was adopted; and
“Outcomes” were the primary and secondary outcomes of acute inflammatory
responses caused by flexibility training exercises. Thus, the final PICO
question was “Does flexibility training at different intensities increases the
acute inflammatory response in adult men?
Eligibility criteria
Included were
studies involving adults aged between 18 and 45 years and complete articles
published in English, Spanish and Portuguese. There was no restriction for year
of publication.
With respect to
study designs, given the limited number of studies published to date and that
the aim of this review was to map knowledge, randomized and non-randomized
(quasi-experimental) clinical studies were included.
The following
exclusion criteria were established: studies other than randomized, quasi-randomized
or experimental clinical trials, studies involving older adults, children,
individuals with disabilities, limitations, or chronic diseases; studies with
high-performance athletes and those using animal models.
Study selection
The study
selection process was performed by two independent reviewers, with disagreement
resolved by a third reviewer. The articles were selected in two stages. In the
first stage, titles and abstracts of the references identified in the search
were assessed and the potentially eligible studies were pre-selected. In the
second stage, the entire text of the pre-selected studies was evaluated to
confirm eligibility. The selection process was conducted using the Rayyan
platform (https://rayyan.qcri.org) [19]. The entire inclusion and exclusion
process was in accordance with the PRISMA FLOW stages, illustrated in Figure 1.
Studies included
After the
selection process, the following studies were included: one randomized clinical
trial [20] and two quasi-experimental non-randomized studies [8,21].
Data extraction
Standardized
electronic forms were used for this stage. The reviewers independently
extracted data related to the morphological characteristics of the studies, interventions and results. The differences were resolved by
consensus. The following data were initially collected: authors, year of
publication, type of study, sample (number of participants), methods,
intervention protocol and control group (if applicable), outcomes assessed,
results and conclusions.
Assessment of the methodological quality of the
studies included
The
methodological quality and/or risk of bias of the studies were independently
assessed by two reviewers using the appropriate tools for each study design, as
follows: randomized clinical trial - Cochrane risk of bias [22], non-randomized
or quasi-experimental clinical trials - ROBINS-I [23]. The assessment of risk
of bias of randomized clinical trials is summarized in Figure 2 and of
non-randomized or quasi-experimental trials in Table II.
Results
Search results
The search
produced 1014 studies. After duplicates were eliminated, 655 references were
analyzed by title and abstract, resulting in 16 inclusions (according to the
PICO question) for reading in their entirety. After this stage, 13 references
were excluded (different populations, interventions and/or outcomes). At the
end, three studies were considered eligible and analyzed. The flowchart of the
study selection process is presented in Figure 1, and Table I summarizes the
characteristics of these studies.
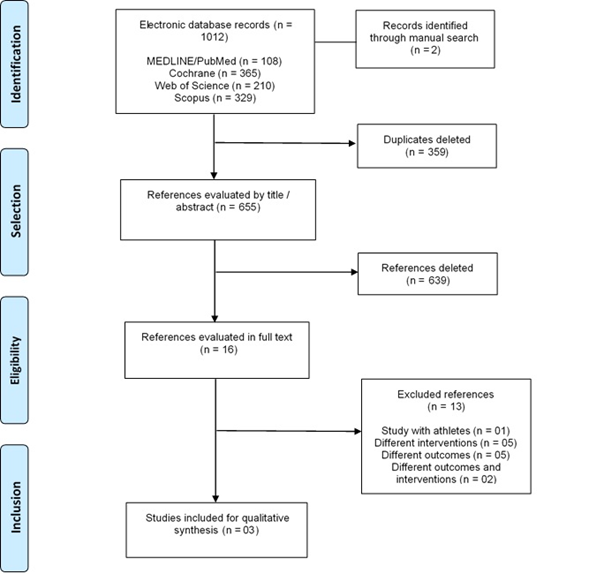
Adapted from Page et
al. [16]
Figure 1 - Flowchart
of the study selection process (PRISMA Flow)
Study results
Since only one
randomized clinical trial was eligible for review [20], we were unable to
conduct a quantitative summary between the studies. Thus, a narrative approach
was more appropriate.
The qualitative
summary obtained for the acute inflammatory responses are presented in Table I.
Table I – Characteristics
of the studies included
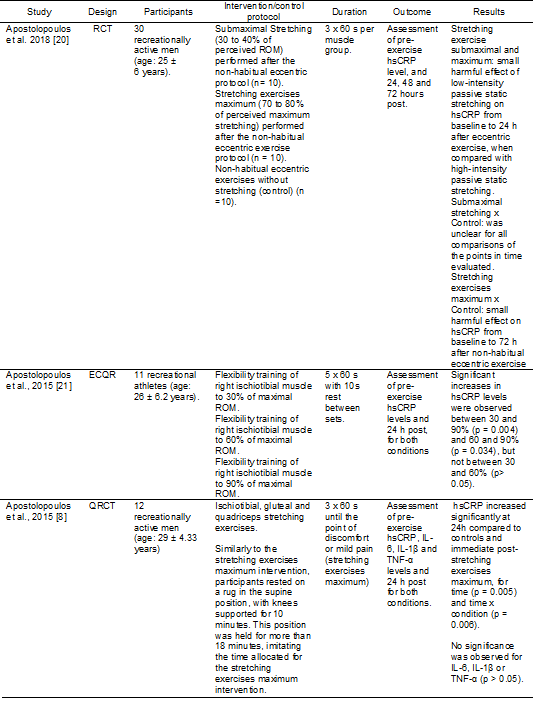
RCT = Randomized
clinical trial; QRCT = Quasi-randomized clinical trial; hsCRP
= high-sensitivity C-reactive protein; ROM: Maximal range of motion; IL-6 =
Interleukin 6; IL-1b = Interleukin 1 beta; TNF-α = Tumor necrosis factor alfa
Risk of bias assessment
In general,
considering the Cochrane tool, the randomized clinical trial showed high risk
of bias and unclear risk in three domains, and low risk of bias only in the
random sequence generation domain, as shown in Figure 2. The quasi-experimental
studies according to the ROBINS-I tool exhibited a serious and critical risk of
bias in most of the domains assessed, and only one study showed low risk of
bias in the incomplete outcome data domain since data were missing, as
illustrated in Chart 2.
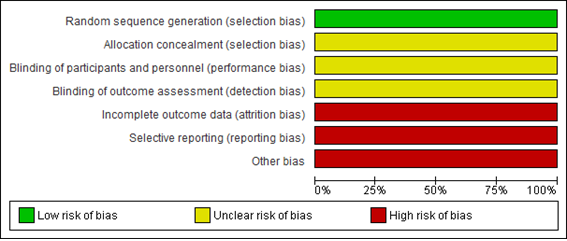
Figure 2 – Risk of bias of the
randomized clinical trial Apostolopoulos et al. 2018
[20], using the Cochrane Risk of Bias table
Chart 2 – Summary of the risk of bias
of non-randomized comparative studies, using the ROBINS-I tool

Green ( + ) = low risk of bias; Yellow ( - ) = moderate risk of
bias; Red (X) = serious risk of bias; Wine-colored ( ! ) = critical risk of
bias
Domains:
D1: Bias related to
confounding factors;
D2: Bias related to
participant selection;
D3: Bias related to
intervention classification;
D4: Bias related to
deviations from intended interventions;
D5: Bias related to
missing data;
D6: Bias related to
outcome assessment;
D7: Selection bias in
the report of results
Assessment certainty of evidence
We were unable
to assess certainty of evidence for the outcome of interest of the present
review, given that only one study (randomized clinical trial) evaluated the
effect magnitude.
Discussion
The evidence of
three clinical trials with available data whose primary and secondary outcomes
were the inflammatory effects caused by flexibility training at different
intensities: one randomized clinical trial [20] and two quasi-experimental
clinical trials [8,21].
Considering the
results of the randomized clinical trial for the outcome analyzed [20], there
was a small harmful effect of submaximal stretching at the hsCRP
concentrations assessed from baseline to 24 hours after eccentric exercise when
compared to stretching exercises maximum. The effects of submaximal stretching
compared to controls were unclear for all the comparisons at the assessment
times of hsCRP levels. However, there was a small
harmful effect of stretching exercises maximum compared to controls on hsCRP from baseline to 72h after non-habitual eccentric
exercise.
According to the
results of this randomized clinical trial [20], stretching exercises maximum
may have caused a slight inflammation, demonstrated by the increase in hsCRP concentrations after non-habitual eccentric exercise,
with statistically higher hsCRP values at 24 h versus
72 h (p = 0.012).
In one of the
quasi-experimental clinical trials, static flexibility training at different
maximal ROM (30, 60 and 90%) in the right ischiotibial
muscle promoted significant increases in hsCRP levels
between 30 and 90% (p = 0.004) and 60 and 90% (p = 0.034), but not between 30
and 60% (p > 0.05), revealing that increases in the percentage of maximal
ROM (intensity) are associated with a rise in hsCRP
levels, causing possible systemic inflammation [21].
In the second
quasi-experimental study, Apostolopoulos et al.
[8] observed that stretching exercises maximum with three 60-second sets of
static insistence to the point of discomfort or mild pain caused an acute
inflammatory response sustained by the significant increase in hsCRP at 24h compared to the control condition and
immediate post-stretching, for time (p = 0.005) and time x condition (p =
0.006). However, no significant increases were observed for inflammatory
markers IL-6, IL-1b or
an-α.
Comparing the
results of the studies included in this review showed that passive stretching
exercises maximum is associated with a likely increase in acute inflammatory
response. Thus, stretching exercises maximum promoted higher concentrations of hsCRP, as clearly demonstrated in the quasi-experimental
studies, in which flexibility training was applied alone, without resistance
exercise.
The force
generated by the acute stretch (mechanical stimulus) causes an excessive
overload of the contractile elements of the skeletal muscle, exceeding their
usual demands and inducing tissue damage [24]. Structurally, there is a
myofilament disarrangement in the sarcomeres, damage to the sarcolemma, loss of
fiber integrity and the subsequent leakage of muscle proteins into the blood
[25]. This functional change causes a reduction or loss of muscle strength and
is responsible for triggering an acute response [24].
The application
of this overload causes microtraumas of varying degrees in the striated
skeletal muscle tissue, connective tissue and bone
tissue. These microtraumas, considered as temporary and repairable damage,
result in an acute inflammatory response, instrumented by numerous specific
chemical mediators such as C-reactive protein (CRP) and the pro-inflammatory
cytokines IL-1b,
IL-6 and TNF-α, derivatives of the injured tissues [13,26,27,28,29]. The extent
of the inflammatory response is determined by the degree of muscle damage, the
magnitude of inflammation, and the lesion-specific interaction between the
invading inflammatory cells and the injured muscle [24,28].
Considering
intensity as an important parameter of flexibility training [26], evidence
indicates that the magnitude of force applied to the muscle during stretching
is a catalyst for tissue damage and inflammation [28,30,31] as observed in animals studies [9,32] and according to the results
presented in this review.
About the
applicability and quality of the evidence, the studies included in the present
review revealed high and critical risk of bias in assessment of the randomized
clinical and quasi-experimental trials [8,20,21], respectively.
However, the
findings of the present review need to be interpreted considering the following
limitations: few studies were eligible, with only one randomized controlled
trial and two quasi-experimental studies; the different study designs,
experimental protocols and controls, measures of results and incomplete data in
some of the studies hampered an additional quantitative synthesis; the
conclusions were based on relatively low-quality data and consequent high risk
of bias; and important methodological questions, such as the lack of allocation
concealment, group comparison at baseline of the participants and assessor
blinding, limited the strength of the study conclusions.
Conclusion
The evidence
available in randomized and non-randomized trials suggests that stretching
exercises maximum, in combination with non-habitual eccentric exercise, or
applied alone, is associated with an acute inflammatory response. However, the
estimates of these results are very low, which precludes definitive
conclusions. The limitations inherent to the design and methodological quality
(high or critical risk of bias) of the studies significantly reduced the
reliability of all the results presented. Thus, new studies with better
methodological quality, involving the variables studied, may better elucidate
the results obtained to date.
Conflict of interest
No conflict of interest
with relevant potential
Financing source
There were no external
sources of funding for this study.
Authors’ contributions
Conception and design
of the research: Nogueira CJ, Senna GW, Dantas EHM;
Data collection: Nogueira CJ, Brandão PP, Souza IV,
Garcia, AS; Analysis and data interpretation: Nogueira CJ, Cortez ACL, Brandão PP, Souza IV, Garcia, AS; Statistical analysis: Not
applicable; Obtaining financing: Not applicable; Writing of the manuscript:
Nogueira CJ, Dantas EHM; Critical review of the
manuscript: Senna GW, Cortez ACL; Final revision of the manuscript: Nogueira
CJ, Brandão PP, Dantas EHM
Academic link
This study is linked to
the thesis of doctoral student Nogueira CJ, from the Stricto
Sensu Post-Graduation Program in Nursing and
Bioscience, Universidade Federal do Estado do Rio de
Janeiro (UNIRIO), Rio de Janeiro, Brazil.
References
- Garber CE, Blissmer B,
Deschenes MR, Franklin BA, Lamonte MJ, Lee IM, et al. Quantity and quality of
exercise for developing and maintaining cardiorespiratory, musculoskeletal, and
neuromotor fitness in apparently healthy adults. Med Sci Sports Exerc 2011;43(7):1334-59. doi: 10.1249/MSS.0b013e318213fefb [Crossref]
- Dantas EHM, Daoud R, Trott A, Nodari Júnior RJ, Conceição MCSC. Flexibility: components, proprioceptive mechanisms and methods. Biomed Hum Kinet 2011;(3):39-43. doi: 10.2478/v10101-011-0009-2 [Crossref]
- Dantas EHM, Conceição MCSC. Flexibility: myths and facts. J Phys Education 2017;86(4):279-83. doi: 10.37310/ref.v86i4.470 [Crossref]
- Nogueira CJ, Galdino AS, Cortez ACL, Vasconcelos Souza I, Mello DB, Senna GW, et al. Effects of flexibility training with different volumes and intensities on the vertical jump performance of adult women. J Phys Educ Sport (JPES) 2019;19(3):1680-85. doi: 10.7752/jpes.2019.03244 [Crossref]
- Nogueira CJ, Galdino LAS, Vale RGS, Mello DB, Dantas EHM. Acute effect of the proprioceptive neuromuscular facilitation method on vertical jump performance. Biomed Hum Kinet 2012;(2):1-4. doi: 10.2478/v10101-010-0001-2 [Crossref]
- Behm DG, Blazevich AJ, Kay AD, McHugh M. Acute effects of muscle stretching on physical performance, range of motion, and injury incidence in healthy active individuals: a systematic review. Appl Physiol Nutr Metab 2016;41(1):1-11. doi: 10.1139/apnm-2015-0235 [Crossref]
- Jacobs CA, Sciascia AD. Factors That influence the efficacy of stretching programs for patients with hypomobility. sports health: a multidisciplinary approach 2011; 3(6):520-23. doi: 10.1177/1941738111415233 [Crossref]
- Apostolopoulos NC, Metsios GS, Taunton J, Koutedakis Y, Wyon M. Acute inflammation response to stretching: a randomised trial. Ita J Sports Reh Po 2015; 2(4): 368-81. doi: 10.17385/ItaJSRP.015.3008 [Crossref]
- Pizza FX, Koh TJ, McGregor SJ, Brooks SV. Muscle inflammatory cells after passive stretches, isometric contractions, and lengthening contractions. J Appl Physiol 2002; 92(5):1873-78. doi: 10.1152/japplphysiol.01055.2001 [Crossref]
- Rossi FE, Gerosa-Neto J, Zanchi NE, Cholewa JM, Lira FS. Impact of short and moderate rest intervals on the acute immunometabolic response to exhaustive strength exercise. J Strength Cond Res 2016;30(6):1563-9. doi: /10.1519/JSC.0000000000001189 [Crossref]
- Peake JM, Della Gatta P,
Suzuki K, Nieman DC. Cytokine expression and secretion by skeletal muscle
cells: regulatory mechanisms and exercise effects. Exerc
Immunol Ver [Internet]. 2015 [cited 2021 Oct 27];(21):8-25.
Available from: http://www.ncbi.nlm.nih.gov/pubmed/25826432
- Ferreira VS, Muller BC, Achour Junior A. Acute effects of static versus dynamic stretching on the vertical jump performance of soccer players. Motriz: J Phys Ed 2013; 19(2):450-459. doi: 10.1590/S1980-65742013000200022 [Crossref]
- Silva FOC, Macedo DV. Physical exercise, inflammatory process and adaptive condition: an overview. Rev Bras Cineantropom Desempenho Hum 2011;13(4):320-8. doi: 10.5007/1980-0037.2011v13n4p320 [Crossref]
- Antunes
Neto JMF, Almeida EJP, Campos MF. Análise de marcadores celulares e bioquímicos
sanguíneos para determinação de parâmetros de monitoramento do treinamento de
praticantes de musculação. RBPFEX [Internet]. 2017 [cited 2021 Oct
27];11(70):778-83. Available from:
http://www.rbpfex.com.br/index.php/rbpfex/article/view/1266
- Brenner IK, Natale VM, Vasiliou P, Moldoveanu AI, Shek PN, Shephard RJ. Impact of three different types of exercise on components of the inflammatory response. Eur J Appl Physiol Occup Physiol 1999;80(5):452-60. doi: 10.1007/s004210050617 [Crossref]
- Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ 2021;372(71). doi: 10.1136/bmj.n71 [Crossref]
- Higgins JPT, Thomas J, Chandler J, Cumpston
M, Li T, Page MJ, et al. Cochrane Handbook for Systematic Reviews of
Interventions version 6.0 (updated July 2019). [Internet]. Cochrane, 2019.
[cited 2021 Oct 27]. Available from: http://www.training.cochrane.org/handbook
- Santos CMDC, Pimenta CADM, Nobre MRC.The PICO strategy for the research question construction and evidence search. Rev Lat Am Enfermagem 2007;15(3):508-11. doi: 10.1590/S0104-11692007000300023 [Crossref]
- Ouzzani M, Hammady H, Fedorowicz Z, Elmagarmid A. Rayyan: A web and mobile app for systematic
reviews. Systematic Reviews 2016;5(1):210. doi: 10.1186/s13643-016-0384-4 [Crossref]
- Apostolopoulos NC, Lahart IM, Plyley MJ, Taunton J, Nevill AM, Koutedakis Y, et al. The effects of different passive static stretching intensities on recovery from unaccustomed eccentric exercise - a randomized controlled trial. Appl Physiol Nutr Metab 2018;43(8):806-15. doi: 10.1139/apnm-2017-0841 [Crossref]
- Apostolopoulos NC, Metsios GS, Nevill AM, Koutedakis Y. Stretch intensity vs. inflammation: a dose-dependent association? IJKSS 2015;3(1):1-6. doi: 10.7575/aiac.ijkss.v.3n.1p.27 [Crossref]
- Whiting P, Savović J, Higgins JPT, Caldwell DM, Reeves BC, Shea B, et al. ROBIS: A new tool to assess risk of bias in systematic reviews was developed. J Clin Epidemiol 2016;(69):225-34. doi: 10.1016/j.jclinepi.2015.06.005 [Crossref]
- Sterne JA, Hernán MA, Reeves BC, Savović J, Berkman ND, Viswanathan M, et al. ROBINS-I: A tool for assessing risk of bias in non-randomised studies of interventions. BMJ (Online) 2016;355:i4919. doi: 10.1136/bmj.i4919 [Crossref]
- Peake JM, Neubauer O, Della Gatta PA, Nosaka K. Muscle damage and inflammation during recovery from exercise. J Appl Physiol 2017:122(3),559-70. doi: 10.1152/japplphysiol.00971.2016 [Crossref]
- Urso ML. Anti-inflammatory interventions and skeletal muscle injury: benefit or detriment? J Appl Physiol 2013;115(6):920-8. doi: 10.1152/japplphysiol.00036.2013 [Crossref]
- Apostolopoulos NC.
Stretching intensity and the inflammatory response - a paradigm shift. Switzerland: Springer Natures;
2018.
- Rocha
AL, Pinto AP, Kohama EB, Pauli JR, De Moura LP,
Cintra DE, et al. The proinflammatory effects of chronic excessive
exercise. Cytokine 2019;119:57-61. doi: 10.1016/j.cyto.2019.02.016 [Crossref]
- Silva
VF, Braga JC, Santos KM, Oliveira GL, Oliveira TAP, Teixeira AM, et al. Pain,
inflammation and performance can predict the ideal moment to apply new
overload. J Sport Sci [Internet]. 2021 [cited 2021 Oct 27];14(1):32-41.
Available from: https://sportscience.ba/pdf/br27.pdf
- Pedersen BK. The physiology of optimizing health with a focus on exercise as medicine. Annu Rev Physiol 2019;81:607-27. https://doi.org/10.1146/annurev-physiol-020518-114339 [Crossref]
- Antunes BM, Inoue DS, Lira FS, Rossi FE, Rosa-Neto JC. Imunometabolismo e exercício físico: uma nova fronteira do conhecimento. Motricidade 2017;13(1):85-98. https://doi.org/10.6063/motricidade.7941 [Crossref]
- Bessa AL, Oliveira VN, Agostini GG, Oliveira RJS, Oliveira ACS, White GE, et al. Exercise intensity and recovery: biomarkers of injury, inflammation, and oxidative stress. J Strength Cond Res 2016;30:311-9. https://doi.org/10.1519/JSC.0b013e31828f1ee9 [Crossref]
- Berrueta L, Muskaj I, Olenich S, Butler T, Badger GJ, Colas RA, et al. Stretching impacts inflammation resolution in connective tissue. J Cell Physiol 2016;231(7):1621-27. https://doi.org/10.1002/jcp.25263 [Crossref]