Rev Bras Fisiol Exerc 2021;20(6):618-32
doi: 10.33233/rbfex.v20i6.4943
ORIGINAL ARTICLE
Risk behaviors
for relative energy deficiency in sport in young high-performance Brazilian
rhythmic gymnasts
Comportamentos de risco para deficiência
de energia relativa no esporte em jovens ginastas rítmicas brasileiras de alto
rendimento
Igor Leite Marques1, Vinícius Oliveira Menezes1,
Raquel de Jesus Silva1, Marcia Regina Aversani
Lourenço1, João Henrique Gomes2, Renata Rebello Mendes1
1Universidade Federal de Sergipe,
Aracaju, SE, Brazil
2Universidade do Norte do Paraná
(UNOPAR), Londrina, PR, Brazil
Received: September
29, 2021; Accepted: October
29, 2021.
Correspondence: Renata Rebello Mendes, Universidade
Federal de Sergipe, Departamento de Nutrição (DNUT), Av. Marechal Rondon, s/n -
Jardim Rosa Elze, 49100-000 São Cristóvão SE
Igor Leite Marques:
igorlmarquesufs@gmail.com
Vinícius Oliveira
Menezes: vinimamute1999@gmail.com
Raquel de Jesus Silva:
raqueljs@live.com
Marcia Regina Aversani Lourenço: marcia.aversanilourenco@gmail.com
João Henrique Gomes:
profjhgomes@gmail.com
Renata Rebello Mendes:
remendes@academico.ufs.br
Abstract
Introduction:
Rhythmic gymnastics is an aesthetic sport, whose rules encourage long line and
lean biotype, exposing gymnasts to the risk of relative energy deficiency in
sport (RED-S). Objective: To analyze risk behaviors for RED-S in
high-performance Brazilian gymnasts from pre-infant, infant and juvenile
categories, with national and international prominence. Methods: 36
Brazilian athletes (10 pre-infant, 9 infant and 17 juveniles) were evaluated
for body composition, sexual maturation and risk of eating disorders. The
investigation of training volume, menstrual cycles, monitoring of bone mineral
density and laboratory tests, occurrence of stress fracture, specialized
nutritional monitoring and consumption of food supplements, was carried out
through a questionnaire adapted by Ackerman. Results: The gymnasts had a
weekly training volume of 27.32 hours, % of fat mass of 12.1 ± 2.8, with infant
having the lowest adiposity. As for sexual maturation, 66.1% were in the
pubescent phase, and no athlete reached the post-pubescent phase. The frequency
of risk of eating disorders was 55.6%, being the most affected juveniles
(70.6%). Only 47.1% of the juveniles had menarche. Only 36.1% have access to a
sports nutritionist, while 16.7% evaluated bone mineral density at least once
in their career, and 52.8% regularly perform laboratory tests. Stress fracture
was reported by 22.2% of the gymnasts, 44.4% in the juveniles. Food
supplementation was found in 36.1% of the gymnasts, especially vitamins C and
D, and proteins. Conclusion: Risk behaviors were found for RED-S in
young Brazilian rhythmic gymnasts with high performance, with emphasis for
eating disorders, especially in the juvenile category.
Keywords:
relative energy deficiency in sport; feeding behavior; gymnastic; adolescent.
Resumo
Introdução: A ginástica rítmica é uma modalidade
esportiva estética, cujas regras encorajam biotipo longilíneo e magro, expondo
ginastas ao risco de deficiência energética relativa no esporte (RED-S). Objetivo:
Analisar comportamentos de risco para RED-S em ginastas brasileiras de alto
rendimento de categorias pré-infantil, infantil e
juvenil, com destaque nacional e internacional. Métodos: 36 atletas
brasileiras (10 pré-infantis, 9 infantis e 17
juvenis) foram avaliadas quanto à composição corporal, maturação sexual e risco
de transtornos alimentares. A investigação de volume de treinamento, ciclos
menstruais, monitoramento de densidade mineral óssea e de exames laboratoriais,
ocorrência de fratura por estresse, acompanhamento nutricional especializado e
consumo de suplementos alimentares realizou-se por questionário de Ackerman
adaptado. Resultados: As ginastas apresentaram volume de treinamento
semanal de 27,32 horas, % de massa gorda de 12,1 ± 2,8, sendo as infantis as de
menor adiposidade. Quanto à maturação sexual, 66,1% encontravam-se na fase
púbere, e nenhuma atleta chegou à fase pós-púbere. A frequência de risco de
transtornos alimentares foi de 55,6%, sendo as juvenis mais afetadas (70,6%).
Apenas 47,1% das juvenis apresentaram menarca. Somente 36,1% têm acesso a
nutricionista esportivo, enquanto 16,7% avaliaram a densidade mineral óssea ao
menos uma vez na carreira, e 52,8% realizam exames laboratoriais regularmente.
Foi relatada fratura por estresse por 22,2% das ginastas, sendo 44,4% nas
juvenis. Encontrou-se suplementação alimentar em 36,1% das ginastas, com
destaque para vitaminas C e D e proteínas. Conclusão: Foram encontrados
comportamentos de risco para RED-S em jovens ginastas rítmicas brasileiras de
alto rendimento, com destaque para transtornos alimentares, especialmente na
categoria juvenil.
Palavras-chave: deficiência energética relativa no
esporte; comportamento alimentar; ginástica; adolescência.
Introduction
Rhythmic
gymnastics (RG) is a sport modality of body movements that requires a
combination of beauty, thinness, and elegance of classical ballet, associated
with strength and physical fitness. Although the competition exercises last
between 90 and 150 seconds, in the individual and group events, respectively,
the training sessions are strenuous, consisting of warm-up, ballet, physical
preparation, and series training, which can vary according to the periodization
phase [1].
In
the competitive context, body weight is considered a relevant requirement for
good performance in acrobatic modalities, as “smaller” athletes seem to gain
biomechanical advantages [2]. Additionally, as it is also an aesthetic
modality, the rules of RG indirectly encourage a long biotype and low
adiposity. Thus, body shape has been reported to be relevant to satisfy judges
and the public, and body weight can be an eliminatory parameter in an elite
gymnast selection [3].
The
search for the thin biotype makes athletes more susceptible to dietary patterns
characterized by an imbalance between energy intake and physical exercise. This
increases the risk of adopting health and performance risk behaviors, including
eating disorders (ED) [4].
For
many years, ED was considered a pillar of the female athlete triad (FAT),
together with menstrual dysfunction and impaired bone health [5]. Recently, low
energy availability (LEA) was included as a causal factor of FAT, which may or
may not be due to ED. Currently, ED continues to be used as diagnostic criteria
for FAT and Relative Energy Deficiency in Sport (RED-S) [6].
The
term RED-S is considered an expansion of FAT, as it includes other clinical
outcomes resulting from LEA, such as the reduced metabolic rate at rest, decreases
in immunity and protein synthesis capacity, damage to cardiovascular health, as
well as gastrointestinal, hematological, psychological, growth, and development
changes [7].
Thus,
the assessment of behaviors related to health care of high-performance rhythmic
gymnasts is essential to promote strategies for the prevention and treatment of
RED-S [8]. This study aimed to describe risk behaviors for the development of
RED-S in young athletes with national and international prominence in Brazilian
rhythmic gymnastics.
Methods
Experimental
design
This
is a descriptive and exploratory research. Data were collected during the Primeiro Estágio de Treinamento de Ginástica Rítmica do Brasil (First Stage of
Rhythmic Gymnastics Training in Brazil), which lasted one week. In the first
visit, athletes, coaches, and guardians were informed about all the procedures
inherent to the study and, after clarification, they signed the Free and
Informed Consent Term (TCLE). On the second visit, an anthropometric assessment
was performed. On the third visit, the athletes answered the questionnaire to
characterize the variables of interest and performed a self-assessment of
sexual maturation. At the last visit, the athletes responded to tests to assess
the risk of eating disorders.
Participants
Thirty-six
high-performance Brazilian rhythmic gymnastics athletes were evaluated, with an
average age of 12 ± 1.9 years, who participated in the Primeiro
Estágio de Treinamento de Ginástica Rítmica do Brasil (First Stage of Rhythmic Gymnastics Training in
Brazil), an event organized by the Brazilian Gymnastics Confederation, held at
Aracaju/SE. To this end, Brazilian gymnasts were invited from the pre-infant (9
to 10 years old), infant (11 to 12 years old) and juvenile (13 to 15 years old)
categories, medalists in national and international championships in 2019, in
general or with apparatus tests, as well as the gymnasts who represented the
South American champion groups, configuring themselves as the elite practicing
the sport in Brazil. As exclusion criteria, hormonal contraceptives use was
adopted.
Body composition
To
characterize the body composition, anthropometry was performed, with collection
of body weight, height and skinfolds. Weight and height were measured on an
analog scale with a coupled stadiometer (Toledo®) with a precision scale of 100
g and 1.0 cm, respectively. To estimate the percentage of body fat (%FM), the
triceps and subscapular skinfolds were measured with a scientific adipometer (Sanny®), with 0.1 mm
precision, according to the standards determined by the International Society
for Advancement of Kinanthropometry (2001). The
measurements were taken three times by the same examiner, not consecutively,
considering the mean of the values, which was then applied to the equation of
Slaughter et al. (1992) [9] and classified according to Lohman (1992)
[10].
Eating disorders
For
the risk assessment for eating disorders, the Eating Attitudes Test (EAT-26) in
its validated version for females [11] and the Bulimic Investigatory Test
Edinburgh (BITE) were adopted. The EAT is a questionnaire consisting of 26
questions, evaluated on a Likert scale with 6 response options (from “always”
to “never”), divided into three factors: a) diet – related to pathological
refusal to high-content foods caloric and concern with physical appearance; b)
bulimia and preoccupation with food: refers to episodes of binge eating,
followed by purgative behaviors to lose/control body weight and; c) oral
self-control: reflects self-control concerning food and assesses the
environmental and social forces that stimulate food intake. The BITE is a
validated questionnaire to identify individuals with binge eating and assess
cognitive and behavioral aspects related to nervous bulimia [12].
Sexual
maturation
Sexual
maturation was self-assessed using a board that assesses the development of
breasts and pubic hair, according to criteria proposed by Tanner [13], with
stage 1 corresponding to the prepubertal phase, stages 2, 3, and 4
characterizing the pubertal period, and stage 5, the post-pubertal phase. In
cases where athletes have marked different stages for each secondary sexual
character (breasts and pubic hair), the smallest stage was considered,
according to Tanner [13].
Risk factors for
RED-S
The
evaluation of training volume, menstrual cycles, monitoring of bone mineral
density (BMD) through Dual-energy X-ray Absorptiometry (DEXA), regular
laboratory tests (LT), history of stress fracture (SF), monitoring by a sports
nutritionist, as well as the consumption of food supplements, was performed
using a questionnaire adapted from Ackerman et al. [6].
Statistical
analysis
The
collected data were submitted to descriptive statistics, presented as mean and
standard deviation. For the normality test, the Kolmogorov-Smirnov test was
used. Analysis of Variance (ANOVA) was used, and the significance adopted was p
≤ 0.05. All statistical procedures were performed using SPSS (Statistical
Package for the Social Sciences) software, version 21.0.
Ethical aspects
This
study followed the guidelines and norms that monitor research with human beings
(Law 196/96) and was approved by the local Ethics Committee (opinion
3.121.613). After informing the athletes and their guardians of the risks and
testing procedures, the guardians signed an informed consent form.
Results
Table
I shows that there were statistical differences in variables such as age, body
weight, height, BMI, fat mass, and lean mass, with juvenile athletes being the
heaviest, tallest, with higher values of BMI, fat mass, and lean mass in kg,
while infants were the gymnasts with the highest percentage of lean body mass.
Table I - Descriptive
statistics (mean ± standard deviation) regarding age, training routine, body
composition, and risk test scores for eating disorders among young
high-performance Brazilian rhythmic gymnasts, according to categories
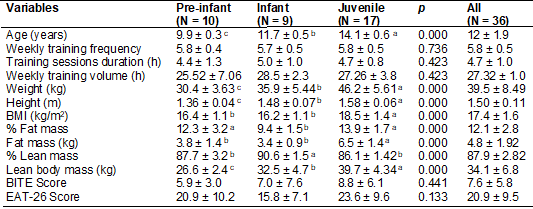
Values
with different letters indicate means with a significant difference (p <
0.05); Statistical differences were determined by one-way ANOVA followed by
Tukey's test
Figures
1 to 5 demonstrate the frequencies found in the studied population concerning
the variables of interest. The association between duration and frequency of
the most cited training sessions in all categories evaluated (figure 1)
culminated in an average volume of 27.3 hours per week.
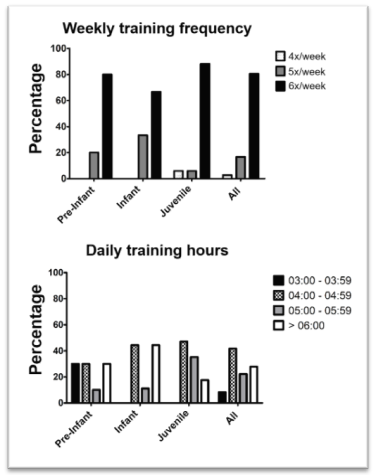
Figure 1 - Weekly
frequency and duration of training sessions of the evaluated rhythmic gymnasts,
according to the categories
Regarding
the EAT-26, most gymnasts showed risk behaviors for the development of ED, with
the juvenile and pre-infant categories being the most affected. The figure also
shows that the risk of bulimia was lower than the results obtained by the
EAT-26, with a higher frequency among infant gymnasts (Figure 2).

Figure 2 - Risk
of eating disorders according to the EAT-26 and BITE instruments, in the
evaluated rhythmic gymnasts, according to the categories
As
shown in Figure 3, most gymnasts evaluated are in their pubescent stage. When
stratifying the results into categories, most pre-infants and infants are in
the pre-pubescent phase, and the pubescent phase is unanimous among the
juveniles. There was no self-assessed athlete in the postpubertal
phase. No athlete in the pre-infant and infant categories had menarche, and a
minority of juveniles had menarche. In addition, among the 17 youth gymnasts,
12 (70.6%) athletes were 14 years old, 3 (17.6%) were 15 years old, and 2
(11.8%) were 13 years old.

Figure 3 - Sexual
maturation and presence of menarche in the evaluated rhythmic gymnasts,
according to the categories
Figure
4 shows that a minority of gymnasts have access to specialized nutritional care
in the sports area, with this behavior being similar
in all categories. About 45% of athletes do not undergo laboratory tests
regularly. Figure 4 also shows that few gymnasts performed DEXA at least once
in their sports career, with a history of stress fractures, especially those in
the infants' category.
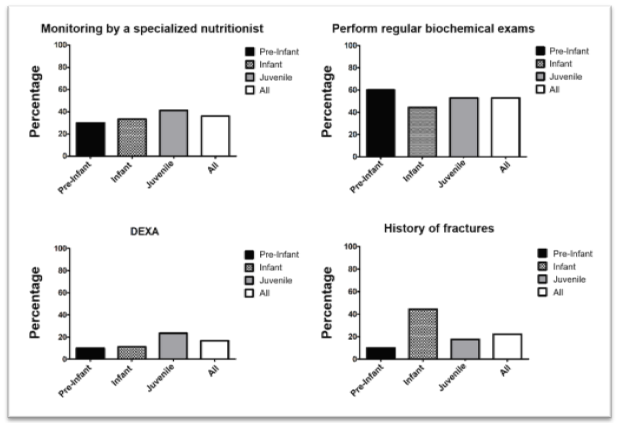
Figure 4 - Monitoring
by a sports nutritionist, history of stress fractures, the performance of
laboratory biochemical tests, and DEXA by rhythmic gymnasts evaluated,
according to the categories
Figure
5 shows that most gymnasts had a low fat-mass percentage, especially in the
infants' category.
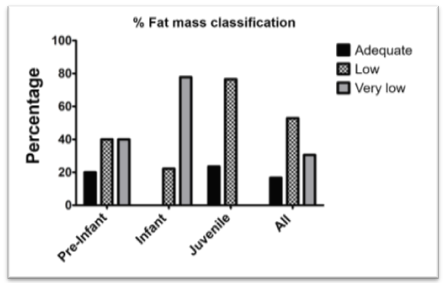
Figure 5 -
Classification of the fat mass of the evaluated rhythmic gymnasts, according to
the categories
Table
II shows the consumption of food supplements, with the juvenile group being the
largest consumer, with emphasis on vitamin C, vitamin D, and proteins.
Table II - Frequency
of consumption of nutritional supplements and products mentioned by gymnasts
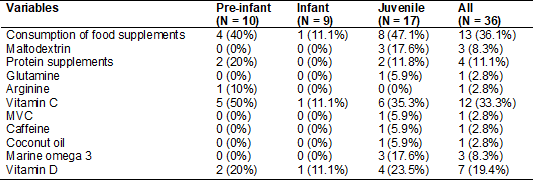
MVC
= Multivitamin and Mineral Complexes
Discussion
The
main findings of the present study show that the elite rhythmic gymnasts
evaluated had a high training volume and low adiposity, with child athletes
being the thinnest. Most gymnasts evaluated were in the pubescent stage, with
pre-infants predominantly categorized as pre-pubescent and juveniles as
pubescent. High risk for ED was found in most athletes, with juvenile and
pre-infant categories being the most affected. Menarche was only identified in
juvenile athletes, although most athletes in this category have not yet had
their first menstruation. Most gymnasts do not have access to specialized
nutritional care in the sports field and do not perform exams considered
essential for assessing bone mineral density. Stress fractures were mentioned
in all categories, especially those in the children's category. Most gymnasts
do not consume nutritional supplements. According to our searches, to date,
this is the first national and international study that analyzes behaviors for
RED-S in elite young rhythmic gymnasts, stratified by categories.
The
high volume of training, associated with low adiposity, and the high risk of
eating disorders, has been associated with low energy availability (LEA), the
latter being the main etiological factor of RED-S. As a consequence, athletes
in LEA can present damage in the hypothalamic-pituitary-gonadal axis,
culminating in hypoestrogenism, amenorrhea, alterations in sexual maturation,
and even damage to cardiac health [6].
LEA
and eating disorders have also been correlated with less release of leptin,
insulin, and triiodothyronine (T3), and a greater synthesis of cortisol and
parathormone, with these hormonal changes being able to reduce osteoblast
activity, culminating in bone demineralization and greater risk of stress
fractures. Thus, the International Olympic Committee advises that athletes
exposed to the risk of RED-S perform bone mineral density assessment, through
DEXA, every one or two years and that the assessment of biochemical exams be
performed every six months [7], thus as the Australian Institute of Sport (AIS)
states that such athletes must be accompanied by a specialist nutritionist
[14].
The
International Society of Sports Nutrition (ISSN) [15] reports that athletes
undergoing high-volume training often face difficulties consuming enough food
to meet their caloric needs, especially carbohydrates, for reasons related to
gastrointestinal discomfort during training and induced hunger suppression by
intense exercise. Thus, the ISSN suggests that, in these cases, the use of
carbohydrate supplements during training is convenient to prevent low energy
availability and RED-S.
Thus,
it is possible to infer that the findings of our study point to important signs
for the development of RED-S in the evaluated gymnasts, which, in addition to
the aforementioned outcomes, can also promote immunological, hematological,
psychological, and performance damage [7].
The
findings' stratification of the present study, according to age groups, also
brought important observations to light. Regarding anthropometric data, the
difference in body weight between the three groups may be associated with
changes in height, which is expected; however, the higher BMI of the juveniles
may be related to the gymnasts' transition to different stages of pubertal
development, since in this category all athletes were in the pubertal stage.
Gonçalves et al. [16] state there is an increase in body mass as the
pre-pubertal individual moves to the pubescent and post-pubescent stages. As
for body composition, it is believed that the higher percentage of body fat in
pre-infants, concerning children, is related to the process of energy
repletion, characteristic of the pre-pubertal phase, and so necessary for
future development (pubertal spurt) [17]. The lower percentage of fat mass
found in children's gymnasts can also be linked to the stage of sexual
maturation, since practically half of the group is pubescent, and according to Fidencio et al. [18], this is the stage in which the
spurt usually occurs, favoring the reduction of fat mass. And the greater
adiposity found in juveniles, compared to children, may also be related to
biological maturation [19]. In Gemelli, Farias, and Spritzer [20], the
occurrence of menarche was associated with body fat gain.
The
training volume found in the present study was about 27.3 hours, varying
between 24 and 30 hours per week. Batista et al. [21] reported a volume
of 36 hours/week in athletes from the Brazilian and Portuguese teams of RG,
data that are consistent with the results of the present study.
In
aesthetic modalities, the combination of intense training and pressure to
achieve weight and performance goals can lead athletes to develop risky dietary
patterns [21], as well as RED-S [6,7]. The term eating disorder refers to
severe disturbances in eating behavior and body image, among which are nervous
anorexia and nervous bulimia. The EAT was proposed as an objective and
self-report measure of the symptoms of nervous anorexia, thus being more
sensitive to the indication of the presence of symptoms common to this type of
disorder and has been one of the most used instruments in research related to
ED due to its validity and reliability [22].
In the present study, the investigation
using the EAT-26 demonstrated that 55.6% of rhythmic gymnasts presented risk
behavior for eating disorders. A prevalence between 10 and 25% of eating
disorders in athletes has been found, which are considered higher than the
prevalence in non-athletes [23]. However, studies carried out with athletes in
aesthetic modalities show even higher frequencies, on average 40%, which is
similar to our results [24].
Martínez
et al. [4] found a score of 8.73 ± 6.94 and the presence of disorder in
two, in a total of 33 gymnasts. Stofeles Cecon et al. [25] found a positive correlation
between the percentage of fat mass and body dissatisfaction, indicating that
individuals with higher percentages of fat may be more susceptible to the
development of ED. In our study, the athletes who were at higher risk were
those who had higher adiposity in a modality that requires thinness, which
could indicate an association between body image dissatisfaction and the onset
of eating disorders. However, a limitation of the present study was the lack of
self-perceived image assessment and body satisfaction.
Athletes
in aesthetic sports are more likely to develop characteristic behaviors of low
energy availability (LEA), as they seek to maintain a body composition that
meets the standards required by the sport [21]. Although we have not evaluated
the total energy intake and the energy expenditure added by the training of the
gymnasts evaluated in this study, which we consider a limitation, a high
frequency of athletes classified as having a very low percentage of fat mass
was observed, and thinness has been correlated with LEA [26].
It is
known that the two main outcomes of RED-S are impairment of menstrual function
and bone health [5]. Although genetic factors are the main determinants of
puberty onset, nutritional, health, and psychological status may be involved in
the process. Additionally, a high level of physical exercise can promote
pubertal development delay [27]. The age at which menarche occurs varies
considerably between countries; in Brazil, studies carried out between 2010 and
2014 showed a mean age of 12.2 years [20]. Camargo [28] found the presence of
menarche in only 26% of its sample of 132 Brazilian athletes from RG, with an
average of 13.2 years. Adolescents with marked thinness and thinness had a mean
of 13.53 years and 13.39 years, respectively [29]. In our study, no athlete
from the infantile category had menarche, and only 47.1% of the juvenile
athletes had the first cycle, which may indicate a delay in pubertal
development, indicating menstrual impairment [7].
As
for bone health, our study found that, although very young, practically a
quarter of the athletes have already had stress fractures and almost half of
the juvenile gymnasts. It is noteworthy that these fractures are less common in
children and adolescents when compared to adults [30]. Additionally, it has
been shown that only less than one-fifth of rhythmic gymnasts have undergone
bone mineral density assessment by DEXA, although this is a test suggested by
the International Olympic Committee [7] and the Australian Institute of Sport
[14] for screening for high-performance athletes, to diagnose RED-S early.
Concerning
aesthetic modalities, in which eating disorders and RED-S are more prevalent,
in addition to the investigation of the two main outcomes (menstrual and bone
damage), it is essential to investigate other clinical possibilities, such as
the follow-up of RED-S-related biomarkers, such as leptin, T3 and free
thyroxine (T4l), estradiol, testosterone, cortisol, and lipid profile and blood
count [31]. For this purpose, the Australian Institute of Sports [14]
determines that the interdisciplinary team must be composed of at least one
doctor, a sports nutritionist, and a psychologist, this being called the
“central multidisciplinary team”. However, in the present study, only 36.1% of
the evaluated rhythmic gymnasts are accompanied by a sports nutritionist, and
practically half of those evaluated are not regularly submitted to laboratory
tests.
About
food supplementation, there was an average consumption of 36.1%, highlighting a
higher frequency of consumption of vitamin C, followed by vitamin D and
proteins, while only 8.3% reported consuming carbohydrates (maltodextrin). This
result differs from the study by Jovanov et al.
[32], in which consumption of supplements was seen by 82.2% of 348 athletes and
a tendency by younger athletes (15-16 years) to use carbohydrates,
beta-alanine, glutamine, vitamins, and mineral complexes. It is necessary to
highlight that the average duration of the gymnasts' training sessions
evaluated in this study was 4.7 hours, and, according to the International
Society of Sports Nutrition (ISSN) [15], athletes engaged in prolonged training
sessions can benefit by supplementing carbohydrates in solutions with
concentrations between 6 and 8% of this nutrient, also because in this dilution
the digestion and absorption of carbohydrate would be facilitated. It is
noteworthy that better gastric emptying can be considered an advantage in an
acrobatic modality, in which there are many jumps and aerial activities.
Vitamin
C (ascorbic acid) was the most used supplement by athletes, and its use in
sports is associated with increased antioxidant capacity and reduced excessive
production of reactive oxygen species during and immediately after exercise.
However, the results are still controversial, since in some studies no positive
effects on markers of performance or recovery after exercise were observed
[33]; while, others suggest that 400 mg supplementation can act in the
reduction of late-onset muscle pain and recovery of maximum contractile
function [34]. It is noteworthy that vitamin C supplementation can be
considered a positive factor in the prevention of RED-S, provided that it is
guided by a sports nutritionist, since iron deficiency is a crucial factor in
the hematological outcomes of RED-S [35] and vitamin C is a determining factor
in increasing iron bioavailability [36].
In
the present study, some gymnasts also mentioned the intake of vitamin D
supplements. Low serum vitamin D concentrations have been associated with an
increased risk of fractures [37]. Vitamin D can be obtained from diet and sun
exposure. However, this exposure is highly variable depending on environmental
factors, skin pigmentation, clothing, and the use of sunscreen. Therefore,
obtaining it from diet or supplements may be necessary [34]. According to
Mountjoy et al. [7], athletes with bone damage due to RED-S, or at risk
for it, may benefit from a daily intake of 1500 to 2000 IU of vitamin D until
serum concentration of 25-hydroxy vitamin D between 38-50 ug/day.
About
protein supplementation, it is known that whey protein, the most mentioned
protein supplement by the participants in this study, has some relevant
qualities, especially concerning digestion speed and leucine concentration
[38]. However, the use of this supplement should be evaluated by a sports
nutritionist, as the sum of proteins ingested via food and supplement must be
considered since high-protein diets can be associated with a reduction in pH,
which in healthy and non-athletes, is easily reversed through buffers such as
bicarbonate. However, in high-performance athletes, metabolic acidosis has been
the subject of great debate, as carnosine and bicarbonate are not always
sufficient to control the drop in pH generated by exercise [39], and protein
excess could contribute even more for this ergolytic
situation.
Additionally,
acidosis has been associated with the use of bone alkaline reserves for
tamponade, which would incur less bone mineralization, which could be an
aggravating factor in aesthetic modalities where the risk of RED-S is greater.
It is noteworthy that, although less frequently, caffeine was cited by the
rhythm gymnasts evaluated, and its consumption has been associated with a
reduction in BMD and increased risk of fracture, mainly due to the adverse
effects on calcium balance, increasing its excretion or decreasing its
absorption [40]. Its use without professional monitoring can generate a
potential risk to the bone health of the rhythmic gymnasts evaluated in this
study, especially when we associate this practice with other detected risk
factors, such as low frequency of monitoring of bone mineral density by DEXA,
low frequency of menarche in juvenile athletes, very low concentrations of fat
mass, low frequency of laboratory tests, high training volume, and especially,
high frequency of eating disorders.
The
present study contributes to a better understanding of the risk factors for the
development of RED-S in RG athletes stratified by categories, little explored
in previous research. Brazilian rhythmic gymnastics is a modality on the rise
in Brazil, with the Brazilian team having recently qualified for the Olympic
Games in Tokyo. Therefore, our findings can contribute to the development and
implementation of effective strategies to guide actions for the prevention
and/or treatment of eating disorders and RED-S by inter or transdisciplinary
teams.
Conclusion
The
study showed a high prevalence of eating disorders associated with high
training volume, low adiposity, reduced bone mineral density monitoring,
presence of training-related fractures, low frequency of follow-up by a sports
nutritionist, and irregular laboratory tests in young high-performance
Brazilian gymnasts in the pre-infant, infant and juvenile categories. And in
the juvenile category, a delay in pubertal development was found. Such factors
are related to a higher risk of relative energy deficiency in sport.
We would like to
thank the athletes who participated in the study, as well as the Organizing
Committee of the First Stage of Rhythmic Gymnastics Training in Brazil and the
Brazilian Gymnastics Confederation, for collaborating with the study.
Acknowledgements
Potential
conflict of interest
No
conflicts of interest were reported.
Financing source
There were no external funding sources for this study.
Conception
and design of the research: Marques IL, Mendes
RR; Obtaining data: Marques IL, Menezes VO, Silva RJ; Data analysis
and interpretation: Marques IL, Menezes VO, Silva RJ, Mendes RR; Statistical
analysis: Gomes JH; Obtaining financing: Marques IL; Manuscript writing:
Marques IL, Mendes RR; Critical review of the manuscript for important
intellectual content: Mendes RR.
References
- Gram MCD, Bø K. High level rhythmic gymnasts and urinary
incontinence: Prevalence, risk factors, and influence on performance. Scand J Med Sci Sport 2019;00:1-7.
doi: 10.1111/sms.13548 [Crossref]
- Wasserfurth P, Palmowski J, Hahn A, Krüger K. Reasons for and consequences of low energy availability in female and male athletes: social environment, adaptations, and prevention. Sport Med Open 2020;6(1):44. doi: 10.1186/s40798-020-00275-6 [Crossref]
- San Mauro Martín I. Aspectos nutricionales, antropométricos y psicológicos en gimnasia rítmica. Nutr Hosp 2016;33(4). doi: 10.20960/nh.383 [Crossref]
- Martínez-Rodríguez A, Reche-García C, Martínez-Fernández MDC, Martínez-Sanz JM. Assessment of nutritional-dietary status, body composition, eating behavior, and perceived image in rhythmic gymnastics athletes. Nutr Hosp 2020;37(6):1217-25. doi: 10.20960/nh.03141 [Crossref]
- Brook EM, Tenforde AS, Broad EM, Matzkin EG, Yang HY, Collins JE, et al. Low energy availability, menstrual dysfunction, and impaired bone health: A survey of elite para athletes. Scand J Med Sci Sports 2019;29(5):678-85. doi: 10.1111/sms.13385 [Crossref]
- Ackerman KE, Holtzman B, Cooper KM, Flynn EF, Bruinvels G, Tenforde AS, et al. Low energy availability surrogates correlate with health and performance consequences of Relative Energy Deficiency in Sport. Br J Sports Med 2019;53(10):628-33. doi: 10.1136/bjsports-2017-098958 [Crossref]
- Mountjoy M, Sundgot-Borgen JK, Burke LM, Ackerman KE, Blauwet C, Constantini N, et al. IOC consensus statement on relative energy deficiency in sport (RED-S): 2018 update. Br J Sports Med 2018;52(11):687-97. doi: 10.1136/bjsports-2018-099193 [Crossref]
- Moraes LCL, Moraes e Silva M, Rinaldi IPB, Rojo JR, Gomes
LDC. Ginástica rítmica: perfil sobre a produção científica em periódicos da
América Latina, Caribe e Países Ibéricos. Pensar Mov
[Internet] 2019 [cited 2020 Nov 19];17(1):e33546.
Available from: https://revistas.ucr.ac.cr/index.php/pem/article/view/33546
- Slaughter MH,
Lohman TG, Boileau RA, Horswill CA, Stillman RJ, Van
Loan MD, et al. Skinfold equations for estimation of body fatness in children
and youth. Hum Biol [Internet].1988 [cited 2020 Nov 19];60(5):709-23. Available from: http://www.ncbi.nlm.nih.gov/pubmed/3224965
- Lohman TG.
Advances in body composition assessment. Champaign IL: Human Kinetics
Publishers; 1992.
- Bighetti F. Tradução e validação do Eating Attitudes Test (EAT-26) em
adolescentes do sexo feminino na cidade de Ribeirão Preto - SP [Internet].
[Ribeirão Preto]: Universidade de São Paulo; 2003. [cited
2020 Nov 20]. Available from:
http://www.teses.usp.br/teses/disponiveis/22/22133/tde-12042004-234230/
- Henderson M, Freeman CP. A self-rating scale for bulimia. The “BITE”. Br J Psychiatry 1987;150:18-24. doi: 10.1192/bjp.150.1.18 [Crossref]
- Tanner JM.
Growth at adolescence. With a general consideration of the effects and
environmental factors upon growth and maturation from birth to maturity. 2 ed.
Vol. 28, Oxford: Blackwell Scientific; 1962.
325 p.
- Wells KR, Jeacocke NA, Appaneal R, Smith HD, Vlahovich N, Burke LM, et al. The Australian Institute of Sport (AIS) and National Eating Disorders Collaboration (NEDC) position statement on disordered eating in high performance sport. Br J Sports Med 2020;54(21):1247–58. doi: 10.1136/bjsports-2019-101813 [Crossref]
- Kerksick CM, Wilborn CD, Roberts MD, Smith-Ryan A, Kleiner SM, Jäger R, et al. ISSN exercise & sports nutrition review update: Research & recommendations. J Int Soc Sports Nutr 2018;15(1):38. doi: 10.1186/s12970-018-0242-y [Crossref]
- Gonçalves LGC,
Aquino RLQT, Filho HT, Puggina EF. Caracterização do perfil de jovens
jogadores de futebol: uma análise das habilidades técnicas e variáveis
antropométricas. Motricidade
2016;12(2):27. doi: 10.6063/motricidade.6718 [Crossref]
- Takahashi LAR,
Santos Figueiredo FW, Benedet
J, Vasconcelos FAG, Adami F. Influence of sexual
maturation status on the relationship between body adiposity indicators and
age: a cross-sectional study. BMC
Res Notes 2019;12(1):61. doi: 10.1186/s13104-019-4095-5 [Crossref]
- Fidencio J, Gonçalves FM, Czarnobay SA, Campos VM. Associação entre estado
nutricional, horas de consumo de tela e de atividade física em adolescentes.
Revista Brasileira de Obesidade, Nutrição e Emagrecimento [Internet]. 2018 [cited 2020 Nov 12];12(72):535-41.
Available from: https://dialnet.unirioja.es/servlet/articulo?codigo=6985681
- Chung S. Growth and puberty in obese children and implications of body composition. J Obes Metab Syndr 2017;26(4):243–50. doi: 10.7570/jomes.2017.26.4.243 [Crossref]
- Gemelli IFB,
Farias ES, Spritzer PM. Association of body composition and age at menarche in
girls and adolescents in the Brazilian Legal Amazon. J Pediatr
(Rio J) 2020;96(2):240-6. doi: 10.1016/j.jped.2018.10.012 [Crossref]
- Batista A, Garganta R, Ávila-Carvalho L. Morphological characteristics
and biological maturation of brazilian and portuguese gymnasts. Int J Morphol
[Internet]. junho de 2019;37(2):561-7.
http://doi.org/10.4067/S0717-95022019000200561 [Crossref]
- Spivak-Lavi Z, Peleg O, Tzischinsky O, Stein D, Latzer Y. Differences in the factor structure of the Eating Attitude Test-26 (EAT-26) in different cultures in Israel: Jews, Muslims, and Christians. Nutrients 2021;13(6):1899. doi: 10.3390/nu13061899 [Crossref]
- Petisco-Rodríguez C, Sánchez-Sánchez LC, Fernández-García R, Sánchez-Sánchez J, García-Montes JM. Disordered eating attitudes, anxiety, self-esteem and perfectionism in young athletes and non-athletes. Int J Environ Res Public Health 2020;17(18):6754. doi: 10.3390/ijerph17186754 [Crossref]
- Fortes L, Almeida S, Ferreira M. Influência da ansiedade nos comportamentos de risco para os transtornos alimentares em ginastas. Rev Bras Atividade Física Saúde 2013;18(5). doi: 10.12820/rbafs.v.18n5p546 [Crossref]
- Stofeles Cecon R,
Castro Franceschini SC, Gouveia Peluzio MC, Miranda Hermsdorff HH, Priore SE. Anthropometric
profile, body composition and body image perception of adolescents with
positive screening for eating disorders. Rev Chil Nutr 2017;44(4):337-40. doi: 10.4067/s0717-75182017000400337 [Crossref]
- Sim A, Burns SF. Review: questionnaires as measures for low energy availability (LEA) and relative energy deficiency in sport (RED-S) in athletes. J Eat Disord 2021;9(1):41. doi: 10.1186/s40337-021-00396-7 [Crossref]
- Campos CG, Carlos FM, Muniz LA, Bila
WC, Damasceno VO, Romano MCC, et al. Atividade física na adolescência e
maturidade sexual: uma revisão sistemática. Cienc Saude Colet [Internet]. 2021 [cited May 2021];26(5):1823–32.
Available from:
http://www.scielo.br/scielo.php?script=sci_arttext&pid=S1413-81232021000501823&tlng=pt
- Camargo CTA, Gomez-Campos RA, Cossio-Bolaños MA, Barbeta VJDO, Arruda M, Guerra-Junior G. Growth and body composition in Brazilian female rhythmic gymnastics athletes. J Sports Sci 2014;32(19):1790-6. doi: 10.1080/02640414.2014.926381 [Crossref]
- Barros BS, Kuschnir MCMC, Bloch KV, Silva TLN. ERICA: age at menarche and its association with nutritional status. J Pediatr (Rio J) 2019;95(1):106-11. doi: 10.1016/j.jped.2017.12.004 [Crossref]
- Prado MP, Abussamra A, Mendes M,
Medeiros BC, Longo CH, Alberto L. Fraturas por estresse do pé e tornozelo na
criança. Assoc Bras Med e Cir do Tornozelo e Pé 2012;6:2-9. Available from: https://jfootankle.com/ABTPe/article/view/603
- Elliott-Sale KJ,
Tenforde AS, Parziale AL,
Holtzman B, Ackerman KE. Endocrine effects of relative energy deficiency in
sport. Int J Sport Nutr Exerc
Metab 2018;28(4):335-49. doi: 10.1123/ijsnem.2018-0127 [Crossref]
- Jovanov P, Đorđić V, Obradović B, Barak O, Pezo L, Marić A, et al. Prevalence, knowledge and attitudes towards using sports supplements among young athletes. J Int Soc Sports Nutr 2019;16(1):27. doi: 10.1186/s12970-019-0294-7 [Crossref]
- Oliveira DCX,
Rosa FT, Simões-Ambrósio L, Jordao
AA, Deminice R. Antioxidant vitamin supplementation
prevents oxidative stress but does not enhance performance in young football
athletes. Nutrition 2019;63/64:29-35. doi: 10.1016/j.nut.2019.01.007 [Crossref]
- Heaton LE, Davis
JK, Rawson ES, Nuccio RP, Witard OC, Stein KW, et al. Selected
in-season nutritional strategies to enhance recovery for team sport athletes: a
practical overview. Sports Med [Internet]. 2017;47(11):2201-18. Available from:
http://www.ncbi.nlm.nih.gov/pubmed/28702900
- Williams NI, Statuta SM, Austin A. Female athlete triad: future directions for energy availability and eating disorder research and practice. Clin Sports Med 2017;36(4):671-86. doi: 10.1007/s40279-017-0759-2 [Crossref]
- Lynch S, Pfeiffer CM, Georgieff MK, Brittenham G, Fairweather-Tait S, Hurrell RF, et al. Biomarkers of Nutrition for Development (BOND) Iron Review. J Nutr 2018;148(suppl1):1001S-1067S. doi: 10.1093/jn/nxx036 [Crossref]
- Krahenbühl T, Borges JH, Barros-Filho AA,
Guerra-Junior G, Gonçalves EM. Assessment of bone mineral density in young female
handball players. Brazilian J Kinanthropometry Hum
Perform 2018;20(1):102-13. doi: 10.5007/1980-0037.2018v20n1p102 [Crossref]
- Jäger R, Kerksick CM, Campbell BI, Cribb PJ, Wells SD, Skwiat TM, et al. International Society of Sports Nutrition Position Stand: protein and exercise. J Int Soc Sports Nutr 2017;14(1):20. doi: 10.1186/s12970-017-0177-8 [Crossref]
- Huerta Ojeda Á, Tapia Cerda C, Poblete Salvatierra MF, Barahona-Fuentes G, Jorquera Aguilera C. Effects of beta-alanine supplementation on physical performance in aerobic-anaerobic transition zones: a systematic review and meta-analysis. Nutrients 2020;12(9):2490. doi: 10.3390/nu12092490 [Crossref]
- Chau Y-P, Au PCM, Li GHY, Sing C-W, Cheng VKF, Tan KCB, et al. Serum metabolome of coffee consumption and its association with bone mineral density: The Hong Kong Osteoporosis Study. J Clin Endocrinol Metab 2020;105(3):e619-27. doi: 10.1210/clinem/dgz210 [Crossref]
