Rev Bras Fisiol Exerc 2022;2193):163-71
doi: 10.33233/rbfex.v21i3.5154
ORIGINAL ARTICLE
Elevation training mask in respiratory muscle strength and
thoracoabdominal expansion in athletics practitioners
Máscara de treinamento
elevado na força muscular respiratória e expansibilidade toracoabdominal
em praticantes de atletismo
Scarlatt Jordanna
Pereira Silva1, Yanca Carollynne
Souza Moraes1, Hosana Thaynara de Pádua1,
Victor Hugo de Sousa Utida1, Erikson Custódio Alcântara1,
Marco Antonio Basso Filho1, Marcos Rassi Fernandes2, Luciana Carvalho Silveira2
1Pontifícia Universidade Católica de
Goiás, Goiânia, GO, Brazil
2Faculdade de Medicina da Universidade
Federal de Goiás, Goiânia, GO, Brazil
Received on: April 21, 2022; Accepted on: August 30, 2022.
Correspondence: Hosana Thaynara
de Pádua, Rua 235, 15 Setor Leste Universitário 74605-050 Goiânia GO
Scarlatt Jordanna
Pereira Silva: scarlattjps@gmail.com
Yanca Carollynne
Souza Moraes: yanca7moraes@gmail.com
Hosana Thaynara de Pádua: hosanapadua@gmail.com
Victor
Hugo de Sousa Utida: v.utida@gmail.com
Erikson
Custódio Alcântara: eriksonalcantara@hotmail.com
Marco Antonio Basso Filho: mbassofilho@gmail.com
Marcos Rassi Fernandes: marcosombro@ufg.br
Luciana
Carvalho Silveira: lucianacsilveira@yahoo.com.br
Abstract
Introduction: Exposure to moderate or high altitudes promotes
physiological changes in all systems of the human body, mainly cardiovascular
and respiratory. The elevation training mask (ETM) was developed with the
function of simulating respiratory conditions at moderate and high altitudes. Objectives:
The objectives of this study were to evaluate the effects of ETM on respiratory
muscle strength and lung expansion in athletics practitioners. Methods:
This is a prospective and longitudinal study. The sample was non-probabilistic,
composed of athletics practitioners. The individuals were divided into an
Intervention Group (IG) that used ETM (LiveUP Sports)
and a Control Group (CG) that did not use it. Study outcomes were maximal
inspiratory pressure and maximal expiratory pressure, lung expansion by
axillary, xiphoid, and abdominal cirtometry. Results:
The peripheral oxygen saturation (SpO2) decresased
in the pre- and post-intervention of both groups. The CG showed higher values in
the variables xiphoid cirtometry, abdominal cirtometry, MIP and MEP. Different GI results, significant
only in xiphoid and abdominal cirtometries. Conclusion:
The high training mask does not improve the thoracoabdominal expansion and the
strength of the ventilatory muscles of athletics practitioners.
Keywords: muscle strength; resistance training, athletes;
exercise.
Resumo
Introdução: Exposição a altitudes moderadas ou
elevadas promove alterações fisiológicas em todos os sistemas do corpo humano,
principalmente cardiovascular e respiratório. A máscara de treinamento elevado
(MTE) foi desenvolvida com a função de simular condições respiratórias em
moderadas e grandes altitudes. Objetivos: O objetivo deste estudo foi
avaliar os efeitos do uso da MTE na força muscular respiratória e na
expansibilidade tóracoabdominal em praticantes de
atletismo. Métodos: Trata-se de um de um estudo prospectivo e
longitudinal. A amostra foi não probabilística composta por praticantes de
atletismo. Os indivíduos foram divididos em Grupo Intervenção (GI) que utilizou a
MTE e Grupo Controle (GC) que não a utilizou. Os desfechos do estudo foram pressão
inspiratória máxima e pressão expiratória máxima, expansibilidade toracoabdominal pela cirtometria axilar, xifoidiana e
abdominal. Resultados: Houve redução da saturação periférica de oxigênio
(SpO2) no pré e pós-intervenção de ambos
os grupos. O GC apresentou maiores valores nas variáveis cirtometria xifóide, cirtometria abdominal, PImáx
e PEmáx. Resultados GI diferentes,
significativos apenas nas cirtometrias xifóide e
abdominal. Conclusão: A máscara de treinamento elevado não melhora a
expansão toracoabdominal e a força dos músculos
ventilatórios de praticantes de atletismo.
Palavras-chave: força muscular; treinamento de força;
atletas; exercício físico.
Introduction
Exposure to moderate (1300 to 2400 m) or high
altitudes (above 2500 m) promotes physiological changes in all human body
systems, mainly cardiovascular and respiratory. This occurs due to the decrease
in barometric pressure in these places where the levels of partial pressure of
oxygen (PpO2) are reduced, causing low supply and decreased
consumption, as well as drops in central and peripheral saturation [1,2].
Exercises performed at these high altitudes lead to a
reduction in PpO2, temperature, and air density, making marathon
runners less resistant to high-speed movements. Under these conditions,
high-performance athletes lose minimal aerobic power performance during races.
The organism undergoes changes to adapt to the environment when practicing
specific training at simulated altitudes [3].
The elevation training mask (ETM) was developed to
simulate respiratory conditions at moderate and high altitudes [4]. It has
already been used by Mixed Martial Arts, running, cycling, and bodybuilding
athletes, as it is a simple piece of equipment with few contraindications. Its
use is indicated in individuals with high cardiovascular performance [5].
There is a divergence in the literature about the
effect of ETM and the results of respiratory variables with its use [4,6,7].
Thus, this study aimed to evaluate the effect of ETM on respiratory muscle
strength and thoracoabdominal expansion in athletics practitioners.
Methods
Type of study
It is a prospective and longitudinal study carried out
in a public sports center located in a city in the central region of Brazil,
held from September to November 2019, composed of a non-probabilistic sample of
athletics practitioners.
Inclusion criteria
Individuals aged between 13 and 24 years; enrolled in
running training sessions who delivered physical fitness exams; training
frequency of at least twice a week; athletics practice for more than three
months; signing of the Free and Informed Consent Term, being signed by the
legal guardian when under 18 years of age.
Exclusion criteria
Individuals with a training time of fewer than three months were excluded; subjects who did not attend or had a frequency < 85% and who did not submit the cardiological physical fitness exams.
Data collect
All athletes
underwent 2 assessments (pre and post-intervention), consisting of
personal data, vital signs, axillary, xiphoid and umbilical 3-point
cirtometry and manovacuometry. Vital signs: heart rate, respiratory
rate and systemic blood pressure were collected in all training
sessions before and after the end by the sama examiner in the reserved
space next to the running track, Athlete remained seated at rest for 3
minutes before checking in a chair with back support.
The individuals were divided into Intervention Group
(IG) that used the ETM (LiveUP Sports) and Control
Group (CG) that did not use it. Twelve training sessions were held twice a week
for 45 consecutive days.
Of the 12 sessions, the first three were performed at
914 m, from the fourth to the sixth session at 1829 m, from the seventh to the
ninth at 2743 m, and from the tenth to twelfth at 3658 m. The training lasted
one hour.
In the first session, the IG underwent an adaptation process, in which he used the mask at rest for 10 minutes to adapt to the instrument. The training of the two groups was identical, following the planning of the team of runners. For the safety of the research participants and possible cases of intolerance or adverse effect of the ETM use during training, a rescuer with oxygen support and a defibrillator were made available at the scheduled training times.
Used tools
The instruments used were: Ventcare
analog manovacuometer to measure respiratory muscle
strength; Milward body measuring tape 150 cm to perform cirtometry;
Nonin model GO2 Achieve pulse oximeter to manage and
monitor oxygen saturation; premium aneroid sphygmomanometer; and 3M Littmann® Classic II stethoscope to measure blood pressure.
Manovacuometry was
used to assess respiratory muscle strength through measurements of maximal
inspiratory pressure (MIP) and maximal expiratory pressure (MEP). To perform
the MIP, an expiration was requested to the residual volume and, after
placement of the nasal clip, an inspiration with maximum force. The performance
of the MEP started with inspiration until the total lung capacity and, after
placing the nasal clip, an expiration with maximum force. Three measurements of
each measure were performed, adopting the highest value.
The cirtometry was performed
with the athletes standing and the examiner in front of them. The thoracic
perimeters were measured in three regions of the chest: (1) axillary perimeter,
with the measuring tape passing through the axillary cavities at the level of
the third rib; (2) xiphoid perimeter, passing the tape over the xiphoid process
at the level of the seventh costal cartilage; (3) umbilical perimeter, passing
over the umbilicus. First, the athletes take a deep inspiration and exhale all
the inspired air, and then follow the measurements of maximum inspiration at
the level of total lung capacity and maximum expiration at the level of
residual volume in the three cited regions, with three measurements in each and
eligibility of the best numerical variation.
Pulse oximetry was performed with the oximeter in contact with the skin of the index fingers of each athlete, waiting for a 2-minute interval with the device and recording the value at the end of this time. For the blood pressure measurement, the athletes were placed in a sitting position, with both feet flat on the floor and their backs straight, supported on the back of the chair.
Independent outomes/variables
The study outcomes were: MIP and MEP, thoracoabdominal expansion by axillary, xiphoid, and abdominal cirtometry. The independent variables were: age group (< 18/18 to 25 years); sex (male/female); sport modality (endurance/sprinter); training time (< 24 months/ > 24 months); exercise frequency (x/week); heart rate (HR/bpm), respiratory rate (RR/ipm); systolic blood pressure (SBP/mmHg); diastolic blood pressure (DBP/mmHg) and peripheral oxygen saturation (SpO2/%).
Data analysis
Data were analyzed using the Statistical Package of Social Sciences (SPSS 23.0). The demographic profile and vital signs characterization of the athletes in the IG and CG were performed using absolute and relative frequency for qualitative variables, while mean and standard deviation for quantitative variables. The homogeneity of the athletes' profiles in both groups was verified using Pearson's chi-square tests. Data normality was verified using the Shapiro-Wilk test. The t-student test was used to compare the means between the groups studied, while the t-paired test was used for the analysis before and after in the two groups.
Ethical aspects
The work was approved by the Ethics and Research
Committee of the Pontifícia Universidade
Católica de Goiás under
number 3,626,289.
Results
The initial sample consisted of 20 athletes. However,
four individuals were excluded from the research due to lack of assiduity in
training, two from the CG and two from the GI. Therefore, 16 participating
athletes remained.
Table I demonstrates the profile characterization of
the athletes in the study and the homogeneity between the variables analyzed.
Table I - Profile characterization of athletes in the
control and intervention groups (n = 16)
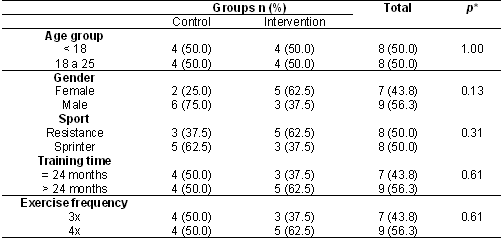
*Pearson's chi-square; n = absolute frequency; % =
relative frequency
Table II characterizes the mean vital signs in the
control and intervention groups, after the 12 training sessions, with no
statistically significant differences between the groups.
Table II - Characterization of vital signs in the control
and intervention groups after the training sessions (n = 16)

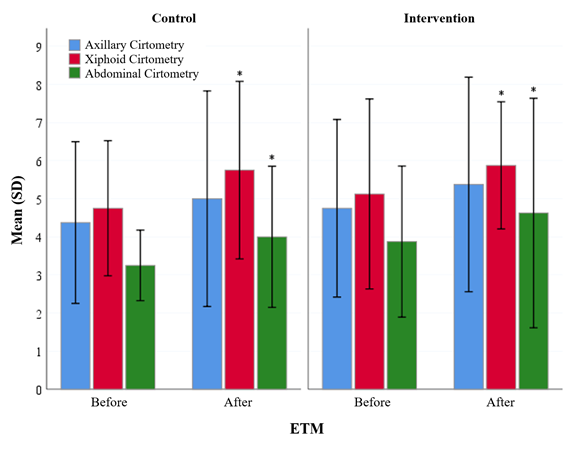
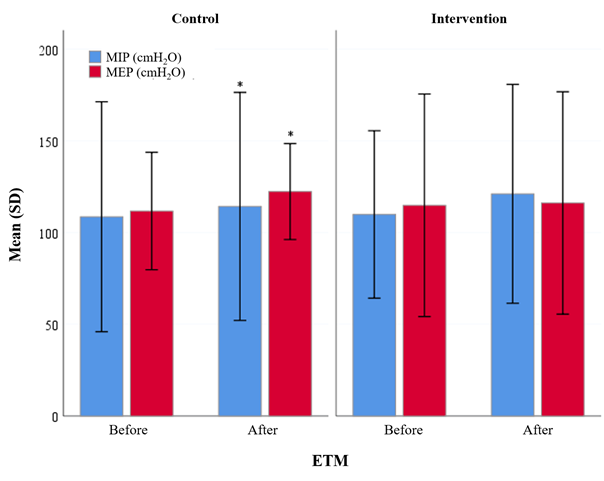
The evaluation of cirtometry
and manovacuometry in the CG and IG before and after
the twelve training sessions showed statistically significant differences in
the CG, both in xiphoid and abdominal cirtometry and
in MIP and MEP. In the IG, only in the xiphoid and abdominal cirtometry (Table III). (Figures 1 and 2).
Table III - Evaluation of cirtometry
and manovacuometry in the control and intervention
groups before and after training (n = 16)
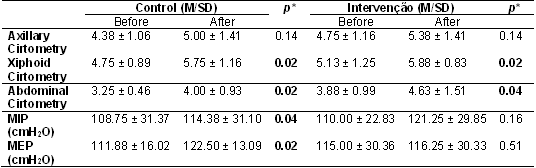
*Paired t-test; M = mean; SD = standard deviation
*p = 0.05
Figure 1 - Initial cirtometry
values and after conclusion of the 12 training sessions in the control and
intervention groups
*p = 0.05
Figure 2 - Initial manovacuometry
values and after conclusion of the 12 training sessions in the control and
intervention groups
Discussion
The results of this study report no differences
between the groups regarding the use of ETM in athletics practitioners.
Specific training based on the physiology of the sport itself can already be
decisive in the differences found in both cirtometry
and manovacuometry, and not only due to the use of
ETM.
Divergent and scarce are the studies that evaluated
the use effects of this ETM instrument, and this study becomes essential
regarding the analysis of the variable thoracoabdominal expansion by cirtometry [8].
Kwitschal et
al. [9] reported a difference only in MIP after the ETM usage, suggesting a
considerable improvement in the inspiratory muscles within eight weeks. In this
study, in the assessment of basal cirtometry before
and after using the mask, there was no difference, although the group showed an
improvement, which may be associated with a small sample. The authors suggest
that the increase in inspiratory resistance offered by the mask triggers an
improvement only in thoracic mobility, requiring additional studies with a
larger sample and longer use of the ETM.
Sellers et al. [10] evaluated the effectiveness
of ETM on the physical fitness of reserve officers, and the results showed no
significant aerobic and anaerobic adaptations. This was because the ETM was
used only during the maximum and submaximal capacity tests, with a small sample
and evaluation in a short period. It had no effect in training simulating
altitude, despite differing from the variables studied in the present study.
The authors suggest the need to incorporate training with greater scientific
evidence with the use of ETM.
Elmarakby et
al. [11] found no significant differences between the groups of athletes
when assessing respiratory muscle strength, endurance, and aerobic capacity at
a 12-week interval when comparing the ETM to two respiratory training devices,
which corroborates our findings. The authors suggest that the device should be
used to minimize respiratory fatigue and improve exercise performance,
maximizing its positive effects in high-intensity training.
Munhoz et
al. [12] found that thoracoabdominal expansion and pulmonary function did
not exceed the normal range expected by the athletes' high aerobic capacity, confirming
our results by proving that the ETM did not produce significant effects on the
aforementioned outcome. The lack of data regarding the interval and duration of
this study suggests the need to carry out additional studies between these
variables and the use of ETM.
On the other hand, Hartz and Moreno [9] showed that
thoracic mobility and muscle strength in handball athletes in inspiratory
muscle training were shown to be at better levels in 12 weeks, which confronts
our findings of the ETM not producing the desired effects. Thus, comparing the
presented study, it can be understood that the training time is a determining
factor for the divergent results between the studies.
Our study had the sample size and a short time
interval as limitations, which may have interfered with the outcomes studied,
generating a possibility of type II error. Other points to be highlighted would
be the non-randomization of athletes in the study groups, without randomness in
their allocation, as well as possible selection bias in the choice of
participating athletes. On the other hand, the presence of a control group
allowed the comparison of the data obtained to expand the scientific knowledge
of the topic addressed.
Conclusion
The ETM use did not change the thoracoabdominal
expansion and respiratory muscle strength in athletes practicing athletics.
Academic affiliation
This article represents the Course Conclusion Paper by
Scarlatt Jordanna Pereira
Silva, supervised by Professor Luciana Carvalho Silveira at Pontificia Universidade Católica de Goiás in Goiânia.
Potential conflict of interest
No potential conflicts of interest relevant to this
article have been reported.
Financing source
There were no external funding sources for this study.
Authors' contribution
Research conception and design: Silva SJP, Silveira LC, Utida VHS, Alcântara EC, Filho MAB; Obtaining data: Silva SJP,
Silveira LC; Data analysis and interpretation: Silva SJP, Silveira LC, Pádua HT, Filho MAB, Fernandes MR; Writing of the
manuscript: Silva SJP, Moraes YCS, Pádua HT,
Filho MAB, Silveira LC; Critical review of the manuscript for important
intellectual content: Fernandes MR
References
- Neder JA, Andreoni S, Lerario MC, Nery LE. Reference
values for lung function tests. II. Maximal respiratory pressures and voluntary
ventilation. Braz J Med Biol Res 1999;32(6):719-27. doi: 10.1590/S0100-879X1999000600007 [Crossref]
- Granja KSB, Neves RHS, Calles ACDN. Resposta fisiológica sobre o efeito da
altitude no exercício: uma revisão. Ciências Biológicas e da Saúde [Internet].
2016 [cited 2022 Aug
30];3(3):71-80. Available from:
https://periodicos.set.edu.br/fitsbiosaude/article/view/3259
- Araújo RC. Efeitos da
exposição à altitude no desempenho físico. Revista Digital-Buenos Aires
[Internet]. 2009 [cited 2022 Aug
30];13(129). Available from:
https://efdeportes.com/efd129/efeitos-da-exposicao-a-altitude-no-desempenho-fisico.htm#:~:text=Exposições%20prolongadas%20à%20altitude%20proporcionam,e%20maior%20concentração%20de%20hemoglobina
- Porcari JP, Probst L,
Forrester K, Dobertein S, Foster C, Cress M.L,
Schmidt K. Effect of wearing the elevation training mask on aerobic capacity,
lung function, and hematological variables. Journal of Sports Science and
Medicine [Internet]. 2016 [cited 2022 Aug 30];15(2):379-86. Available from:
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4879455/pdf/jssm-15-379.pdf
- Vargas Pinilla OC. Exercise and training at altitudes: physiological effects and protocols. Rev Cienc Salud 2014;12(1):111-26. doi: 10.12804/revsalud12.1.2014.07 [Crossref]
- Biggs NC, England BS, Turcotte NJ, Cook MR, Williams AL. Effects of
simulated altitude on maximal oxygen up take and inspiratory fitness. Int J Exerc Sci [Internet]. 2017 [cited 2022 Aug
30];10(1):127-36. Available from: https://pubmed.ncbi.nlm.nih.gov/28479953/
- Shen SC, Nacgalon Y, Randall DR, Zeltzer NN, Belafsky PC. High elevation training mask as a respiratory muscle strength training tool for dysphagia. Acta Oto-Laryncologica 2019;1-5. doi: 10.1080/00016489.2019.1605196 [Crossref]
- Hartz CS, Moreno MA. Efeitos
do treinamento muscular inspiratório em atletas de handebol [Internet]. VI
Congresso de Ciência do Desporto. Dez 2015. [cited
2022 Aug 30]. Available from:
https://www.fef.unicamp.br/fef/sites/uploads/fef_inscricao/ccd2015/paper-1443664339.pdf
- Kwitschall GS, Sartor
AV, Paula KM, Waltrick RP, Bahr
AC, Waltrick T. Influência do training mask sobre os parâmetros cardiorrespiratórios em
praticantes de exercícios aeróbicos. Revista Brasileira de Prescrição e
Fisiologia do Exercício [Internet]. 2019 [cited 2022 Aug 30];14(90):250-63. Available from:
http://www.rbpfex.com.br/index.php/rbpfex/article/view/1998
- 10.Sellers JH, Monaghan TP, Schnaiter JA, Jacobson BH, Pope ZK. Efficacy of a ventilatory training mask to improve anaerobic and aerobic capacity in reserve officers training corps cadets. J Strength Cond Res 2016;30(4):1155-60. doi: 10.1519/JSC.0000000000001184 [Crossref]
- Elmarakby A, Siniscarco M, Simpson B, Nunno-Evans M. Comparative study of two different respiratory training devices on lung function, respiratory muscle strength and endurance, and aerobic capacity in division III athletes. Crit Rev Phys Rehabil Med 2021:21-43. doi: 10.1615/CritRevPhysRehabilMed.2021040613 [Crossref]
- Munhoz GM, Mazzoti M, Santos ALD, Gimenes C, Manzano RM. Avaliação da função pulmonar e expansibilidade torácica em atletas de futsal. Revista Inspirar [Internet]. 2012 [cited 2022 Aug 30];4(20):1-5. Available from: https://www.inspirar.com.br/wp-content/uploads/2012/11/avaliacao-funcao-pulmonar-artigo-239.pdf
