Rev Bras
Fisiol Exerc. 2023;22:e225312
ORIGINAL ARTICLE
Prevalence of medial tibial stress syndrome in university
students
Prevalência
da síndrome de estresse tibial medial em estudantes universitários
Pablo Ursini Abreu1, Thainá Santos
da Cunha1, Leandro dos Santos2, Valério Garrone Barauna1
1Universidade Federal do Espírito Santo,
Vitória, ES, Brazil
2Universidade Federal Rural de
Pernambuco, Serra Talhada, PE, Brazil
Received: October 5, 2022; Accepted: January 12, 2023.
Correspondence: Valério Garrone Barauna, barauna2@gmail.com
Abreu PU, Cunha TS, Santos L, Barauna
VG. Prevalence of medial tibial stress syndrome in
university students. Rev Bras Fisiol Exerc. 2023;22:e225312. doi: 10.33233/rbfex.v22i1.5312
Abstract
Introduction: Medial Tibial Stress
Syndrome can be defined as pain along the posteromedial edge of the tibia that occurs
during exercise. Its incidence can reach 35% in military and athletes. Objective:
The study aimed to show the prevalence of the syndrome in students of Physical education
and Physical therapy courses at UFES. Methods:
A cross-sectional study was
carried out on 141 students. All students answered a questionnaire
about personal
data, level of physical activity and clinical history of the syndrome.
A physical
exam was performed for those who presented with compatible clinical
history. If positive, it would be suggestive that the student had the
syndrome. Results:
Our results demonstrate no significant differences between the prevalence of syndrome
between courses, gender and the volume of physical activity between groups with
and without the syndrome. The the most reported activity by the positive group was
weight training. Conclusion: We conclude that possibly extrinsic factors
such as volume and type of physical activity are not linked to the emergence of
medial tibial stress syndrome.
Keywords: medial tibial stress syndrome; exercise;
pain; physical therapy specialty; physical education and training.
Resumo
Introdução: A Síndrome do estresse tibial medial pode
ser definida como dor ao longo da borda posteromedial
da tíbia que ocorre durante o exercício, sua incidência pode chegar a 35% em militares
e atletas. Objetivo: Mostrar a prevalência da síndrome do estresse tibial
medial nos estudantes dos cursos de Educação Física e Fisioterapia da Universidade
Federal do Espírito Santo, e as características de gênero, tipo e volume de atividade
física e o curso matriculado dos alunos acometidos pela síndrome. Métodos:
Trata-se de um estudo transversal, no qual foram incluídos um total de 141 estudantes,
todos responderam um questionário com perguntas sobre dados pessoais, nível de atividade
física e história clínica da síndrome. Naqueles que apresentaram história clínica
compatível foi realizado um exame físico, caso fosse positivo o participante era
diagnosticado com a síndrome. Resultados: Não houve diferenças significativas
entre a prevalência de síndrome entre os cursos, entre sexos, e nem correlação com
o volume de atividade física praticado. A atividade mais relatada pelos indivíduos
com a síndrome foi a musculação. Conclusão: Os fatores extrínsecos como volume
e tipo de atividade física não estão associados a síndrome do estresse tibial medial.
Palavras-chave: síndrome do estresse tibial medial; exercício
físico; dor; especialidade de fisioterapia; educação física e treinamento.
Introduction
Medial Tibial Stress Syndrome (MTSS)
can be defined as pain along the posteromedial border of the tibia that occurs during
physical exercise. For its confirmation, the presence of pain in an extension of
at least 5 cm in this region is necessary. This is one of the most common
overuse injuries in sports orthopedics, with an incidence of between 4 and 35% in
military populations and athletes [1].
Although its etiology is unknown, there
are several theories about its cause, including periostitis caused by muscles, local
bone lesions due to overload, and fasciitis [2]. About its incidence, we can mention
increased internal and external rotation of the hip, high body mass index, and decreased
calf perimetry, in addition to being more prevalent in females [3,4]. Thus, the
understanding of MTSS is limited, and the elaboration of interventions for its treatment
or prevention is reduced [5].
The association between sports practice
and MTSS incidence is a subject that has been extensively studied in the literature.
Although there is still no absolute evidence about the characteristics of physical
activity and the incidence of MTSS, it is believed that it is more common in activities
with repetitive effort and impact, such as running or jumping [7]. A study by Yates
et al. [1] observed that running was reported as the activity causing pain
in 66% of individuals. A study carried out in 2018 with Physical Education (PE)
students showed an incidence of MTSS ranging from 0-12% and a prevalence of 5-15%.
The authors attributed these results to the high load of practical classes in this
course, as well as the high level of sports practice among PE students [6].
Taking into account the ease of recruiting
and obtaining data, our study was carried out with university students. We investigated
the prevalence of MTSS in Physical Education and Physiotherapy students at the Universidade Federal do Espírito Santo
(UFES). The objective of our study was to investigate the prevalence of MTSS among
students of PE and Physical Therapy courses, to observe the behavior of intrinsic
and extrinsic factors that are associated with MTSS, and to describe the characteristics
of the practice of physical exercise between these two groups of students that may
explain this prevalence of MTSS.
Methods
Study design
An analytical cross-sectional study
was carried out, in which the objects of study were students from the Universidade Federal do Espírito Santo
(UFES) in the PE and Physiotherapy courses, regardless of the period. In this population,
we studied the presence of MTSS, as well as other intrinsic and extrinsic factors.
Scenery
The interviews took place near the UFES
campuses, with Physiotherapy students interviewed at the Health Sciences Center
and Physical Education students at the Physical Education and Sports Center, both
located in Vitória, ES. Approaches took place from 04/01/2020 to 08/31/2020. Data
collection and physical examination were performed in a single meeting.
Participants
A total of 141 students were included
in the study, of which 68 were from the Physical Therapy course and 73 from the
PE course. As an exclusion criterion, any sign of other pain-causing lesions that
could be confused with MTSS, such as paresthesia, edema and fracture history, was
defined. This study was approved by the Human Research Ethics Committee of the Universidade Federal do Espírito Santo
(3,367,411). All participants were informed about the study protocol and signed
an informed consent form accepting to participate in the study.
Questionnaire
Students included in the study answered
an anamnesis that addressed questions about gender, age, education, lower limb dominance,
participation in physical activity, presence of MTSS, and impact of MTSS on their
physical activities.
Physical exam
The physical examination to confirm
the diagnosis of MTSS consisted of palpation of the region of the posteromedial
border of the tibia (with the participant sitting with double flexion of 90 degrees)
and considered positive when the referred pain was in an extension greater than
or equal to 5 cm (Figure 1) [8].

Figure 1- Physical examination
Variables
The main variable investigated was the
presence of MTSS. Secondly, the types and volume of activity practiced. It was expected
that participants considered positive for MTSS would practice activities of higher
impact and would have a greater volume of exercises. Participants who tested positive
in the previously explained physical examination or had a previous medical diagnosis
were considered to have MTSS.
Statistical analysis
Data are presented as mean ± standard
deviation or as frequency and percentage. For statistical analyses, Student's t-test
was used for continuous variables and Fisher's exact test for contingency data.
A statistically significant difference was considered when p < 0.05.
Results
Table I shows the general characteristics
of the study participants. Among the 141 students included in the study, according
to the diagnostic criteria adopted, 18 students had MTSS, which is equivalent to
a 12.8% prevalence.
Table I - Characteristics of the participants
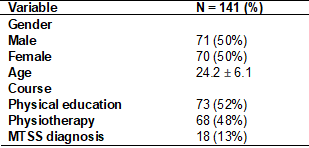
Table II demonstrates the extrinsic/intrinsic
factors comparison according to the student's course. The difference between the
students number by gender between courses reflects this
behavior in reality, in which the number of women who attend Physiotherapy is higher
than that of men, and the opposite is seen in the Physical education course. When
analyzing the weekly exercise volume, Physiotherapy students practiced half the
volume of PE students per week on average (3.4 ± 3.5 vs. 6.8 ± 6.1 h/week, p <
0.01). The weekly volume was calculated using information acquired during the application
of the evaluation form, and the result comes from the multiplication of the weekly
frequency x duration time. The two most cited activities in the two courses were
bodybuilding and running, with bodybuilding cited 25 (48%) times by Physiotherapy
students and 30 (29%) times by PE students, and running 6 (11%) times by Physiotherapy
students and 16 (15%) times by PE students. The activities practiced were counted
cumulatively, and the same student could practice more than one type of physical
exercise, so the sum of the number of activities is greater than the total number
of students. The percentage of practice of activities was calculated by the total
number of activities mentioned.
Table II – Comparison of extrinsic/intrinsic
factors according to course
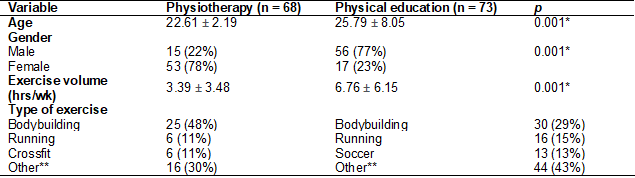
Other** (Pilates, jumping, basketball,
functional training, footvolley, dance, cycling, wrestling, rowing, archery, swimming,
surfing, triathlon, bodyboarding, gymnastics, handball, volleyball, and yoga); Hrs/wk – hours per week. The variables
Age and volume of exercise were analyzed by Student's t-test. The gender and type
of exercise variables were evaluated using Fisher's exact test
Table III shows the extrinsic/intrinsic
factors according to the MTSS diagnosis. There was no significant difference for
any of the factors analyzed between people with or without MTSS. The total volume
was calculated with information on a weekly frequency, duration, and practice time
over time.
Table III - Comparison of characteristics
according to diagnosis
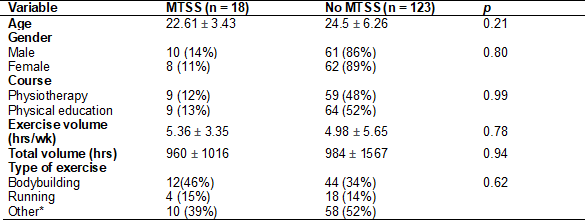
Other*: MTSS (pilates,
basketball, functional training, crossfit, dance, soccer,
gymnastics, and fight); no MTSS – basketball, cycling, crossfit,
wrestling, rowing, dancing, archery, swimming, surfing, triathlon, bodyboarding,
handball, volleyball, and yoga); hrs/wk – hours per week. The variables age, exercise volume, and
total volume were analyzed by Student's t-test. The variables gender, course, and
type of exercise were evaluated using Fisher's exact test
Regarding the participants diagnosed
by physical examination, the activities most reported as causing MTSS symptoms by
the participants were bodybuilding (n = 7; 50%), running (n = 4; 28%), gymnastics
(n = 1; 7%), Crossfit (n = 1; 7%), and basketball (n =
1; 7%). Of these participants, 4 (28%) felt MTSS symptoms unilaterally while exercising,
while another 10 (71%) felt them bilaterally. When asked about the intensity of
pain during exercise, 3 (21%) reported it as being very weak, 6 (43%) as moderate,
4 (29%) as strong, and 1 (7%) as very strong. Regarding the interference of pain
in carrying out physical activities, 2 participants (14%) reported that the MTSS
interferes a little, 4 (29%) a lot, 5 (36%) reasonably, and 3 (21%) said that MTSS
is disabling for physical activities.
Discussion
Our study included 141 students from
the Physical Therapy and Physical Education courses at UFES. No difference was observed
in the prevalence of MTSS between courses. In addition, we also did not observe
any difference in the prevalence of MTSS according to gender, type, or volume of
physical activity practiced.
The incidence and prevalence of MTSS
vary among different populations. In our study, a total prevalence of 12.8% was
found among all students included, 50% of each course. There was no difference in
the prevalence of MTSS between physical education (13%) and physiotherapy (12%)
courses.
Female gender is considered an intrinsic
factor for MTSS. Some studies have already found higher incidences in females, one
of which was carried out with recruits in Australia, in which women had an incidence
of 52.9%, compared to 28.2% among men (RR: 2.03) [9]. In the present study, women
had a prevalence of 11% against 14% in men, which is contrary to what is available
in the literature [1,4,11].
Data, such as volume and type of activity,
were also analyzed to look for a possible cause of this disagreement, but no relevant
correlation was found. Because of this, we assume that the possible explanation
for this event has not been investigated by our study. Despite Physical Education
students having incidences of up to 15% in other studies and being physically more
active than physiotherapy students, the incidence between the two courses did not
show significant differences, even with Physical Education students reporting practicing
approximately twice the volume of activities weekly (6.77 x 3.39, h/week, p <
0.01).
In addition, despite the incidence reaching
up to 20% in runners, in our study, the activity cited as the main cause of pain
was bodybuilding. However, we observed that this may have happened because the students
used this term (bodybuilding) in general, not differentiating between strength and
aerobic exercises, such as running on a treadmill, which we supposed to be the activity
that causes pain in these individuals [6,9]. The volume of weekly hours of physical
activity was not different between the groups with and without MTSS. This data was
also not different in a study carried out with naval recruits [1].
Our results may have possible errors
due to the greater flexibility of the sample, with students from different periods
included, which may influence the time spent performing physical activities. Because
the data were collected through interviews, it can be considered a bias since many
answers depend on the participants' memory.
Conclusion
We conclude that possibly extrinsic
factors such as volume and type of physical activity are not linked to the emergence
of SETM in the studied population, because when comparing students with and without
SETM there was no statistical difference. However, there is still a small number
of studies that address this topic, more studies are needed to realize the role
of these factors in SETM. Our study demonstrated that students of Physical education
and Physiotherapy courses are a good population to look for when one wants to carry
out studies with people with SETM, due to its significant prevalence and the level
of Physical activity of this population, it also shows that bodybuilders can be
a potential population for conducting intervention studies.
Academic affiliation
This article represents a course completion
work by undergraduate students of the Physiotherapy course, Pablo Ursini Abreu and Thainá Santos da
Cunha, supervised by the professor and doctor Valério
Garrone Baraúna, at the Federal
University of Espírito Santo, Vitória, ES, and co-supervised
by Postdoctoral Leandro dos Santos, professor at the Federal Rural University of
Pernambuco, PE.
Conflict of interests
We report that there was no financial,
personal or political conflict of interest for any of the authors and the institution
that contributed financial support.
Financing
The project was financially supported
by the CNPq
Authors’ contributions
Conception and design of
the research: Cunha TS, Abreu PU and Barauna VG; Obtaining data: Cunha TS and Abreu PU; Data
analysis and interpretation: Cunha TS, Abreu PU, Santos L; Statistical analysis:
Barauna VG. Obtaining funding: Abreu PU, Santos
L. Writing of the manuscript: Cunha TS, Abreu PU; Critical review of the
manuscript for important intellectual content: Santos L, Barauna VG.
References
- Yates B, White S. The incidence and risk factors in the
development of medial tibial stress syndrome among naval recruits. Am J Sports Med.
2004;32(3):772-80. doi: 10.1177/0095399703258776 [Crossref]
- Reshef N, R
Guelich D. Medial tibial stress syndrome. Clinics in Sports
Medicine. 2012;31(2):273-90. doi: 10.1016/j.csm.2011.09.008 [Crossref]
- Reinking FM, Austin MT, Richter RR, Krieger MM. Medial
tibial stress syndrome in active individuals: a systematic review and meta-analysis
of risk factors. Sports Health . 2016;9(3). doi: 10.1177/1941738116673299 [Crossref]
- Newman P, Witchalls J, Waddington G, Adams R. Risk factors associated with medial tibial stress syndrome in runners: a systematic review and meta-analysis. Open Access J Sports Med. 2013;13(4):229-41. doi: 10.2147/OAJSM.S39331 [Crossref]
- White M. Medial tibial stress syndrome: diagnosis, treatment and outcome assessment (PhD Academy Award). British Journal of Sports Medicine. 2018;52(18):1213-14. doi: 10.1136/bjsports-2017-098907 [Crossref]
- Bliekendaal S, Moen M, Fokker Y, H Stubbe J, Twisk J, Verhagen E. Incidence and risk factors of medial tibial stress syndrome: a prospective study in physical education teacher education students. BMJ Open Sport Exerc Med. 2018;4(1):1-7. doi: 10.1136/bmjsem-2018-000421 [Crossref]
- Moen MH, Tol JL, Weir A, SteunebrinkM, Winter TC. Medial tibial stress syndrome: a critical review. Sports Med. 2012;39(7):523-46. doi: 10.2165/00007256-200939070-00002 [Crossref]
- Winters M, Bakkers EWP, Moen MH, Barten CC, Teeuwen R, Weir A. Medial tibial stress syndrome can be diagnosed reliably using history and physical examination. Br J Sports Med. 2017;52(19):1267-72. doi: 10.1136/bjsports-2016-097037 [Crossref]
- Lopes AD, Hespanhol Júnior LC, S Yeung S, Costa LOP. What are the main running-related musculoskeletal injuries? Sports Med. 2012;42(10):891-905. doi: 10.1007/BF03262301 [Crossref]
- Verrelst R, Clercq D, Willems TM, Roosen P, Witrouw E. Contralateral risk factors associated with exertional medial tibial pain in women. Med Sci Sports Exerc. 2014;46(8):1546-53. doi: 10.1249/MSS.0000000000000280 [Crossref]
- Bennet J, F Reinking M, Pluemer B, Pentel A, Seaton M, Killian C. Factors contributing to the development of medial tibial stress syndrome in high school runners. J Orthop Sports Phys Ther. 2001;31(09):504-10. doi: 10.2519/jospt.2001.31.9.504 [Crossref]
