Rev Bras Fisiol Exerc. 2023;22:e225373
doi: 10.33233/rbfex.v22i1.5373
REVIEW
Hormonal changes in strength training during the
menstrual cycle: a systematic review
Alterações
hormonais no treinamento de força durante o ciclo menstrual: revisão
sistemática
Vitória
Aparecida da Silva Pereira1, Andreza Alamon
Trindade1, Michel Oliveira da Silva2, André Dias de
Oliveira Fernandes1, Juliana Brandão Pinto de Castro2,
Rodrigo Gomes de Souza Vale2,3, Rogério Santos de Aguiar3
1Universidade Estácio de Sá, Petrópolis,
RJ, Brazil
2Universidade do Estado do Rio de
Janeiro, RJ, Brazil
3Universidade Estácio de Sá, Cabo Frio,
RJ, Brazil
Received: January 23, 2023; Accepted: May 20, 2023.
Correspondence: Rogério Santos de Aguiar, rogghi@gmail.com
How to cite
Pereira VAS,
Trindade AA, Silva MO, Fernandes ADO, Castro JBP, Vale RGS, Aguiar RS. Hormonal changes in strength training during the menstrual cycle: a
systematic review. Rev Bras Fisiol Exerc. 2023;22:e225373. doi: 10.33233/rbfex.v22i1.5373
Abstract
Introduction: During the
menstrual cycle, women are exposed to continual variations in serum
concentrations of various female sex steroid hormones. The fluctuations of the
main female hormones (estrogen, progesterone, follicle stimulating hormone and
luteinizing hormone) are essential for regulating ovulatory cycle patterns. In
this sense, it is speculated that strength training can stimulate the signaling
pathways of essential hormones to regulate the patterns in the different phases
of the ovulatory cycle. Objective: To analyze hormonal changes and
strength performance in different phases of the menstrual cycle in women
experienced in strength training. Methods: A systematic review was
carried out following the PRISMA recommendations. The terms “Strength Training”,
“Resistance Exercise” and “Menstrual Cycle” were searched in Medline (PubMed),
Virtual Health Library, and ScienceDirect databases. We included experimental
studies that evaluated hormonal changes during the menstrual cycle in strength
training in women trained in resistance exercise. Results: From a total
of 592 documents, six studies met the inclusion criteria. Interventions in the
included studies ranged from 2 to 140 days. The protocols demonstrated that the
intervention with strength training changes progesterone, testosterone,
estradiol, and ammonia in the follicular and luteal phases. Conclusion:
The studies investigated in this review demonstrated that strength training
induced hormonal and strength increases, in the follicular phase of the
menstrual cycle, in women experienced in strength training.
Keywords: strength training; resistance
exercises; menstrual cycle.
Resumo
Introdução: Durante o ciclo menstrual, as mulheres
são expostas a variações contínuas nas concentrações séricas de diversos
hormônios esteroides sexuais femininos. As flutuações dos principais hormônios
femininos (estrogênio, progesterona, hormônio folículo estimulante e hormônio
luteinizante) são essenciais para regular os padrões do ciclo ovulatório. Neste sentido, especula-se que o treinamento de
força pode estimular as vias de sinalização dos hormônios essenciais para
regular os padrões nas diferentes fases do ciclo ovulatório.
Objetivo: Analisar as alterações hormonais e o desempenho da força nas
diferentes fases no ciclo menstrual em mulheres experientes submetidas ao
treinamento de força. Métodos: Foi realizada uma revisão sistemática
seguindo as recomendações do PRISMA. Foram pesquisados, nas bases de dados
Medline (PubMed), Biblioteca Virtual em Saúde e ScienceDirect, os termos “Strength
Training”, “Resistance Exercise”
e “Menstrual Cycle”. Foram incluídos estudos
experimentais que avaliaram as alterações hormonais durante o ciclo menstrual
no treinamento de força em mulheres treinadas no exercício resistido. Resultados:
De um total de 592 documentos, seis estudos preencheram os critérios de
inclusão. As intervenções dos estudos incluídos variaram de 2 a 140 dias. Os
protocolos demonstraram que a intervenção com o treinamento de força
proporcionou alteração nos hormônios progesterona, testosterona, estradiol e
amônia nas fases folicular e lútea. Conclusão: Os estudos investigados
nesta revisão demostraram que o treinamento de foça induziu aumentos hormonais
e da força, na fase folicular do ciclo menstrual, em mulheres experientes em
treinamento de força.
Palavras-chave: treinamento de força; exercícios de
resistência; ciclo menstrual.
Introduction
The menstrual cycle is a complex
process involving cell replication and growth under the influence of hormones,
growth factors, neurotransmitters, and regulatory molecules [1]. It is repeated
at regular intervals of 21 to 36 days, with an average of 28 days and consists
of a phenomenon essentially linked to the reproductive life of women [2].
The physiology of the menstrual
cycle depends on the balance between the pituitary-ovaries hypothalamus axis.
Thus, the menstrual cycle requires the secretion of gonadotropin-releasing
hormone (GnRH) by the hypothalamus in a critical range of amplitude and frequency
[3]. During menstrual cycle, estrogen and progesterone are responsible for
changes that occur in the endometrium, uterine cervix, and vagina, in addition
to feedback regulation of secretion of the follicle stimulating hormone (FSH)
and luteinizing hormone (LH) by the anterior pituitary [4].
The MC is composed of four phases.
The follicular phase of the menstrual cycle lasts from 10 to 20 days and ends
with ovulation; the luteal phase lasts for 14 days; and menstrual, from four to
seven days [5]. During this period, ovarian hormones (estrogen and
progesterone) undergo changes in their concentrations, thus demarcating the
phases of menstrual cycle [1]. These phases are known as follicular phase and
luteal phase, which are separated by ovulatory period [6].
The follicular phase begins on the
first day of the menstrual cycle and ends at the end of the ovulatory period,
being characterized by a gradual increase in follicle stimulating hormone
(FSH), low progesterone levels and an estrogen peak near the ovulatory phase
[1]. The luteal phase begins at the end of the ovulatory phase and lasts until
the next menstrual flow, presenting an increase in the concentration of both
estrogen and progesterone [7].
During the menstrual cycle, the
hormones estrogen and progesterone are two primary sex hormones that fluctuate
in three distinct hormonal environments: the early follicular phase
characterized by low concentrations of estrogen and progesterone, the late
follicular phase (or peri-ovulatory) characterized by high concentrations of
estrogen and low progesterone, and the luteal phase, in which high levels of
estrogen and progesterone are present [8].
Chidi-Ogbolu
& Baar [9] demonstrated that women practicing
strength training (ST) in menstrual cycle can stimulate the signaling pathways
induced by hormones such as estrogens and androgens, which are groups of
endogenous sex hormones produced by women and men [10].
Knowles et al. [11] reported
the increase in estrogen during the late follicular phase in ST performance, as
there is increased strength in the follicular phase and declines in the middle
phase of luteum. However, estrogen becomes more abundant after an acute ST
session, generating an increase of 65-95 minutes in the luteal phase compared
to the follicular phase [12]. Then estradiol remains up to 21% higher than
resting levels within 24 hours after training [13].
Rechichi et
al. [8] point out that estrogen has a greater strengthening effect on
skeletal muscle, although the basic mechanism is not clearly known. Variations
during the menstrual phase may be a consequence of changes because of ST on
metabolism, which are again attributed to fluctuations observed in the
concentrations of ovarian hormones [14].
The difficulties around the day of
the test that coincide with hormonal fluctuations and evaluation hormones to
ensure that the correct phase is being examined may be some of the reasons for
the development of few investigations on ST and menstrual cycle [15]. Thus, the
aim of this systematic review was to analyze hormonal changes and strength
performance in different phases of the menstrual cycle in experienced women
submitted to ST.
Methods
This systematic review followed the
recommendations of the Preferred Reporting Items for Systematic reviews and
Meta-Analyses (PRISMA) [16] recommendations and was registered in the
International Prospective Register of Systematic Reviews (PROSPERO), with the
number CRD42020091506.
Eligibility criteria
Table I shows the PICOS strategy
used to delimit inclusion criteria. We excluded studies were excluded with
sedentary women who used some contraceptive method, who had already gone
through menopause or who performed any other type of training.
Table I - PICOS strategy

Search strategy
A search without filters was
performed in Medline (via PubMed), Virtual Health Library (VHL) and
ScienceDirect databases, in October 2022, using the terms "Strength
Training", "Resistance Exercise" and "Menstrual
Cycle". These descriptors were combined using the logical operators [OR]
(between synonyms) and [AND] (between the terms). After the references were
extracted using the search terms, they were exported to a shared EndNote X8
library. Two independent evaluators completed the research, the removal of
duplicates, the analysis of titles and abstracts and the screening of the
complete articles. Any divergences in the analysis were forwarded to a third
evaluator. Then, the studies were read to verify the articles that met the
eligibility criteria of the present study.
Bias analysis
The The Risk Of Bias In Non-randomized Studies (ROBINS-I)
tool was used to assess the risk of bias in the studies included in this review
[17]. The studies were classified as "selection bias",
"performance bias", "detection bias", "monitoring
bias", "report bias", "bias due to lack of data" and
"bias" in the selection of reported results, with the answers
"yes", "probably yes", "probably no", and
"no". Two independent and experienced evaluators analyzed the risk of
bias in the included studies. The disagreements were resolved by a third
evaluator.
Data collection process
The following data were extracted
from the selected studies: country, number of participants in each group, age,
body mass, height, and duration of the menstrual cycle (Table I), intervention
protocol, muscles tested, methodologies, tests used and training load for data
analysis (Table II and III), and hormone analysis (Tables VI).
Results
In total, 594 studies were found
following the proposed research methodology (Medline = 43; VHL = 65;
ScienceDirect = 484). After the use of the selection criteria, six articles
were included in this review (Figure 1).
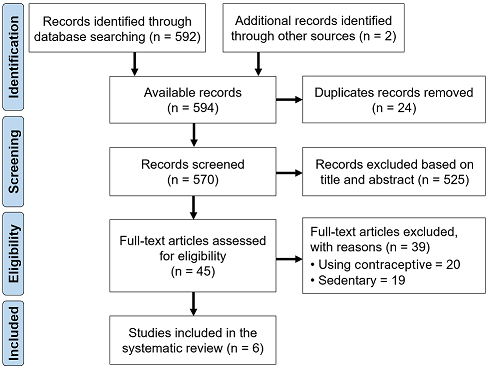
Figure 1 - PRISMA flowchart of the study
selection process
Table II presents the
characteristics of the studies, study countries and sample characteristics of
the studies included in this review. When analyzing the six studies in Table
II, we observed a population of 81 trained women (mean age: 26.3 ± 2.39 years;
body mass: 62.11 ± 2.14 kg; height: 164.5 ± 3.96 m).
Table II - Descriptive characteristics
of the studies included in this review
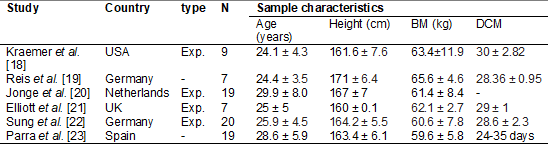
USA = United States of America; UK
= United Kingdom; Exp = Experimental; BM = Body Mass; DMC = Duration of the
menstrual cycle
Table III shows the methodological
characteristics and the results related to the resting conditions in the
imposition of the maximum load, in six of the studies, including intervention
days, the exercises evaluated, the maximal repetition test, training protocol,
interval between sets, and training load.
Table III - Methods and results of the
studies included in this review
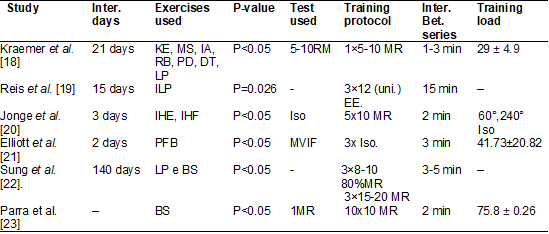
Inter = intervention; LP = Leg
press; BS = back squat; KE = Knee extension; MS = Military Squat; IA = Inclined
abdominal; LR = Low rowing; PD = Pulldown; DT = Direct thread; PFB = Pulled
from behind; IHF = isokinetic hip flexion; IHE = Isokinetic hip extension; MR =
Maximum repetition; MVIF = Maximum voluntary isometric force; ISO = Isometry;
Inter = interval; bet = between; ILP = Isometric leg press
Table IV – Result of hormone variation
pre, during and post ST during the follicular phase
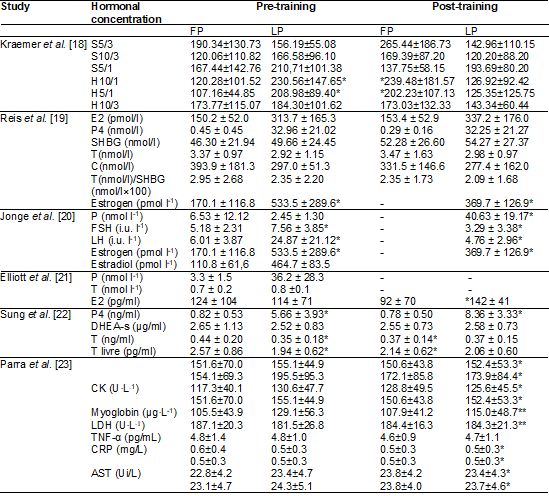
FP = follicular phase; LP = luteal
phase; S = Strength; HC = Hormonal concentration; H = Hypertrophy; 5/3 = 5
maxims repetitions/3 minutes of rest; 10/3 = 10 maxims repetitions/3 minutes of
rest; 5/1 = 5 maxims repetitions /1 minute rest; E2 = Estradiol; P4 =
Progesterone; SHBG = Sex hormone binding globulin; T = Testosterone; C =
Cortisol; FSH = Follicle stimulating hormone; P = Progesterone; FSH = Follicle
stimulating hormone; LH = Luteinizing hormone; DHEA-s = Dihydrotestosterone
sulfate; CK = creatine kinase; LDH = lactate dehydrogenase; IL-6 =
interleukin-6; TNF-α = tumor necrosis factor; CR = C-reactive protein;
AST= aspartate aminotransferase; ALT = alanine aminotransferase; *; ** (p
< 0.05)
TheTable V
presents the risk of bias in the studies through the ROBINS-I tool. Of the six
studies, two studies were considered to have moderate risk [18,21] two were
considered to have a critical risk of bias [19,22] and the other studies were
considered to have a low risk of bias [20,23].
Table V – Risk analysis of bias by the
tool ROBINS-1

P = Probably; 1 = Selection bias; 2
= Performance bias; 3 = Detection bias; 4 = Monitoring bias; 5 = Reporting
bias; 6 = Bias due to lack of data; 7 = Bias in the selection of reported
results
Discussion
This systematic review aimed to
analyze the main findings of hormonal changes and strength performance in
different phases of the menstrual cycle in experienced women undergoing ST. The
six studies included different research questions, measured different hormonal
changes and strength performance at different stages of the menstrual cycle,
and often reported varying results in the homonyms analyzed and increased
muscle strength. From the six included studies (Table II), two did not present
the training load and hormonal analyses [18,22], while the other four presented
the training load and hormonal analyses [19,20,21,23].
Analysis of the studies [18,19,20,21,22,23]
show either that the practice of ST with exercise protocols performed from 2 to
140 days caused a significant increase in estradiol, progesterone,
testosterone, dihydrotestosterone sulfate, cortisol, and ammonia hormones, and
blood markers of muscle damage and inflammation: creatine kinase. myoglobin,
lactate dehydrogenase, interleukin-6, TNF-α, and C-reactive protein.
However, the findings of these
experimental studies should be interpreted with caution as they were classified
as uncertain risk of bias (Table V). Regarding interventions, two studies used
ST isokinetic devices [18,20], two used dynamometers [21,22], and two used free
weights with bars and washers [19,24]. In all studies there were hormonal
variations after the intervention during the different phases of the menstrual
cycle.
In addition, two of these studies
[19,22] reported hormonal analyses before and after training during the
follicular and luteal phase, while two studies [20,21] described hormonal
analyses in follicular phase, medium and late without informing whether it was
pre- or post-test. One study [23] presented the results of the hormonal
analyses of pre-training in the middle of training and immediately after
training in the times of 5 minutes, 120 minutes, 24 and 48 hours. Moreover, two
of these studies did not present the maximum repetition (MR) tests used in the
exercises [19,22] and the other four [18,20,21,23] described the MR tests used
in the protocols.
In this sense, Kraemer et al.
[18], Reis et al. [19], Jonge et al. [20], Sung et
al. [22], and Parra [23] analyzed estrogen, progesterone, creatine kinase,
and ammonia in women during menstrual cycle using an isokinetic dynamometer.
The researchers reported that, after the ST intervention with MRI protocols,
there was a significant increase in estrogen and progesterone levels during
follicular phase for luteal phase (P < 0.05) and luteal phase (P < 0.01).
Estrogen is a hormone with
purported anabolic function, while progesterone has been linked to catabolic
pathways [24]. Given these differences in hormonal functions, it is speculated
that skeletal muscle performance may vary with changes in hormone production
during the different phases of the menstrual cycle.
The current
literature framework does not provide clear answers on this topic. However, Fridén et al. [25] reported an 11% increase in
quadriceps and maximum voluntary isometric handgrip strength in the period of
ovulation that coincided with follicular phase.
Similarly, Bambaeichi
et al. [26] reported that isometric strength performance peaked during
ovulation in follicular phase. These results suggest an association with
ovarian hormones that have a notable influence on protein metabolism during ST
[27]. According to Oosthuyse and Bosch [28], the most
frequent increases in muscle protein synthesis are related to the increase in
training frequency. which favors the gain of muscle mass at rest during
follicular phase.
Haines et al. [29]
highlighted that mRNA protein synthesis ER as well as cyclic expression of skeletal
muscle mRNA D1 appear to be associated with activation and proliferation of
skeletal satellite cells during follicular phase compared to luteal phase after
an acute ST session [30,31].
However, other studies have not
supported these findings as no changes in muscle strength have been found in
the different phases of the menstrual cycle [28]. Gür
[32] and Sterne [33] reported not having found differences in muscle torque in
the concentric and eccentric stages between the menstrual, follicular, and
luteal phases. The ambiguous evidence in the findings may be due to the use of
different methods to estimate the phases of the menstrual cycle and the use of
different muscle strength performance tests. A possible limitation of this
evidence is that most studies have measured peak muscle strength values.
However, in the practical context, the expression of maximum force rarely
occurs, especially if we consider that the ST is commonly performed with
submaximal loads (for example, 60 to 80% of 1MR).
This systematic review has some
limitations that should be highlighted. First, measurements of female sex
hormones were not performed to confirm the duration of the cycle from the
beginning to the end of each phase. Second, none of the studies in this review
reported whether participants measured hormone levels on the day of the test.
It should be shown, given in more detail the three phases of a regular
menstrual cycle. Thus, the chances of showing a relationship between hormone
concentrations and muscle function would be increased. However, despite the
limitations mentioned, the findings provided by the studies may contribute to
elucidate hormonal changes and strength performance at different stages of the
menstrual cycle in experienced women undergoing ST.
Conclusion
The studies analyzed in the present
systematic review showed that ST can cause hormonal increases and improvements
in muscle strength performance during the follicular phase compared to the
luteal phase. It is suggested that the anabolic effects of ST are reduced in
women with menstrual disorders. More studies will be needed to demonstrate the
acute and long-term effects on skeletal muscle on hormonal responses to ST at
different stages of the menstrual cycle.
Conflict of interest
No potential conflicts of interest
for this article were reported.
Funding source
There were no external sources of
funding for this study.
Academic link
This study is linked to the final
work of Pereira AS and Trindade AA of the Physical Education Course at Universidade Estácio de Sá (Petrópolis, RJ, Brazil).
Author’s contribution
Research conception and
design: Pereira AS and Trindade AA, Aguiar RS; Data
analysis and interpretation: Aguiar RS, Castro JBP, Silva MO, Fernandes
ADO; Writing of the manuscript: Pereira AS and Trindade AA, Castro JBP; Critical
review of the manuscript for important intellectual content: Castro JBP,
Vale RGS, Aguiar RS
References
- Freitas LG. Menstrual cycle: evaluation of
alterations. [Tese]. Belo
Horizonte: Federal University of
Minas Gerais; 2016. 104f.
- Giordano
MG, Giordano MV, Giordano LA, Giordano SMA. In: Giordano MG
ed. Gynecological and reproductive endocrinology. Rio de Janeiro: Rubio;
2009;39-47.
- Cunha
MP, Magatão M, Silva DF, Queiroga MR, Silva MP, Paludo AC. Effect of the menstrual cycle on exercise performance:
a quick review of the literature. Brazilian Journal of Prescription and
Exercise Physiology [Internet]. 2021 [cited 2023 Jun 21];15(96):194-202.
Available from:
http://www.rbpfex.com.br/index.php/rbpfex/article/view/2351#:~:text=Cinco%20artigos%20apresentaram%20efeito%20do,a%20fase%20folicular%20vs%20luteal
- Constanzo LS. Fisiologia. Rio de Janeiro:
Elsevier; 2014. p.702-810.
- Pallavi LC, Urbano JDS,
Shivaprakash G. Evaluation of musculoskeletal strength and fatigue levels
during different phases of the menstrual cycle in young adults. J Clin Diagn Res. 2017;11(2):11-3. doi: 10.7860/JCDR/2017/24316.94088 [Crossref]
- Kraemer WJ, Radames
NA. Hormonal responses and adaptations to resistance exercise and training.
Sports Med. 2005;35(4):339-61. doi: 10.2165/00007256-200535040-00004 [Crossref]
- Bandyopadhyay A, Dalui R. Endurance capacity and cardiorespiratory responses in sedentary females during different phases of menstrual cycle. Kathmandu University Medical Journal. 2014.10:25-29. doi: 10.3126/KUMJ.V10I4.10990 [Crossref]
- Rechichi C, Dawson B, Goodman C. Athletic performance and the oral contraceptive. Int J Sports Physiol Perform. 2009;4(2):151-62. doi: 10.1123/ijspp.4.2.151 [Crossref]
- Chidi-Ogbolu N, Baar K. Effect of estrogen on musculoskeletal performance and injury risk. Front Physiol. 2019;(9):1-11. doi: 10.3389/fphys.2018.01834 [Crossref]
- Julian R, Hecksteden AF, Fullagar HH, Meyer T. The effects of menstrual cycle phase on physical performance in female soccer players. PloS One. 2017;(12):0173951. doi: 10.1371/journal.pone.0173951 [Crossref]
- Knowles OE, Aisbett B, Main LC, Drinkwater EJ, Orellana L, Lamon S. Resistance training and skeletal muscle protein metabolism in eumenorrheic females: implications for researchers and practitioners. Sports Med. 2019;49(11):1637-50. doi: 10.1007/s40279-019-01132-7 [Crossref]
- Sakamaki-Sunaga M, Min S, Kamemoto K, Okamoto T. Effects of menstrual phase-dependent resistance training frequency on muscular hypertrophy and strength. J Strength Cond Res. 2016;30(6):1727-34. doi: 10.1519/jsc.0000000000001250 [Crossref]
- Kraemer WJ, Ratamess NA.
Hormonal responses and adaptations to resistance exercise and training. Sports
Med. 2005;35(4):339-61. doi: 10.2165/00007256-200535040-00004 [Crossref]
- Mihm M, Gangooly S, Muttukrishna S. The normal menstrual cycle in women. Anim Reprod Sci. 2011;124(3-4):229-36. doi: 10.1016/j.anireprosci.2010.08.030 [Crossref]
- Nakamura Y, Aizawa K, Imai T, Kono I, Mesaki N. Hormonal responses to resistance exercise during different menstrual cycle states. Med Sci Sports Exerc. 2011;43(6):967-73. doi: 10.1249/MSS.0b013e3182019774 [Crossref]
- Liberati A, Altman DG, Tetzlaff J, Mulrow C, Gøtzsche PC, Ioannidis JPA, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: explanation and elaboration. BMJ 2009;339-b2700. doi: 10.1371/journal.pmed.1000100 [Crossref]
- Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ 2021;(372). doi: 10.1136/bmj.n71 [Crossref]
- Kreamer WJ, Fleck SJ, Dziados JE, Harman EA, Marchitelli LJ, Gordon SE, et al. Changes in hormonal concentrations after different heavy-resistance exercise protocols in women. J Appl Physiol. 1993;75(2):594-604. doi: 10.1152/jappl.1993.75.2.594 [Crossref]
- Reis E, Frick U, Schmidtbleicher D. Frequency variations of strength training sessions triggered by the phases of the menstrual cycle. Int J Sports Med. 1995;16(8):545-50. doi: 10.1055/s-2007-973052 [Crossref]
- Jonge XAK, Boot JCRL,
Thom JM, Ruell PA, Thompson MW. The influence of the
menstrual cycle phase on the contractile characteristics of skeletal muscle in
humans. J Physiol. 2001;530(1):161-6. doi: 10.1111/j.1469-7793.2001.0161m.x [Crossref]
- Elliott KJ, Cable NT, Reilly T, Diver MJ. Effect of menstrual cycle phase on the concentration of bioavailable 17-β o estradiol and testosterone and muscle strength. Clin Sci. 2003;(105):663-9. doi: 10.1042/CS20020360 [Crossref]
- Sung E, Han A, Hinrichs T, Vorgerd
M, Manchado C, Platen P. Effects of follicular versus
luteal phase-based strength training in young women. Springerplus.
2014;(3):668. doi: 10.1186/2193-1801-3-668 [Crossref]
- Parra NR, Moreno LB, Rael B, Magallanes VMA, Cupeiro R, Díaz AE, et al. Influence of menstrual cycle on blood markers of muscle injury and inflammation after exaúcteres exercises. Int J Environ Res Saudi Publica. 2020;17(5)1618. doi: 10.3390/ijerph17051618 [Crossref]
- Hornum M, Cooper DM, Brasel JA, Bueno A, Sietsema KE. Exercise-induced changes in circulating growth factors with cyclic variation in plasma estradiol in women. J Appl Physiol. 1997;82(6):1946-51. doi: 10.1152/jappl.1997.82.6.1946 [Crossref]
- Fridén C,
Hirschberg A, Saartok T. Muscle Strength and
Endurance Do Not Significantly Vary Across 3 Phases of the Menstrual Cycle in
Moderately Active Premenopausal Women. Clin J Sport Med. 2003;13:238-241. doi: 10.1097/00042752-200307000-00007 [Crossref]
- Bambaeichi E,
Reilly T, Cable NT, Giacomini M. The isolated and combined effects of menstrual
cycle phase and time-of-day on muscle strength of eumenorrheic females. Chronobiol Int. 2004;21(4-5):645-60. doi: 10.1081/cbi-120039206 [Crossref]
- Davis HC, Hackney AC. Sex hormonesMihm
M, Gangooly S, Muttukrishna
S. The normal menstrual cycle in women. Anim Reprod Sci. 2011;124(3):229-36. doi: 10.1016/j.anireprosci.2010.08 [Crossref]
- Oosthuyse T, Bosch AN. The effect of the menstrual cycle on exercise metabolism. Sports Med. 2010;40(3):207-27. doi: 10.2165/11317090-000000000-00000 [Crossref]
- Haines M, Mckinley-barnard
SK, Andre TL, Gann JJ, Hwang PS, Willoughby DS. Skeletal muscle estrogen
receptor activation in response to eccentric exercise up-regulates
myogenic-related gene expression independent of difering
serum estradiol levels occurring during the human menstrual cycle. J Sports Sci
Med [Internet]. 2018 [cited 2023 Jun 21];17(1):31-9. Available from:
https://pubmed.ncbi.nlm.nih.gov/29535576/
- Jabbour HN, Kelly RW, Fraser HM, Critchley HO. Endocrine regulation of menstruation. Endocr Rev. 2016;27(1):17-46. doi: 10.1210/ er.2004-0021 [Crossref]
- Kadi F, Schjerling P, Andersen LL, Charifi N, Madsen JL, Christensen LR, Andersen JL. The effects of heavy resistance training and detraining on satellite cells in human skeletal muscles. J Physiol. 2004;558(3):1005-12. doi: 10.1113/jphysiol.2004.065904 [Crossref]
- Gür H. Concentric and eccentric isokinetic measurements in knee muscles during the menstrual cycle: a special reference to reciprocal moment ratios. Arch Phys Med Rehabil. 1997;78:501-05. doi: 10.1016/s0003-9993(97)90164-7 [Crossref]
- Sterne JA, Hernán MA, Reeves BC, Savović J, Berkman ND, Viswanathan M, et al. ROBINS-I: a tool for assessing risk of bias in non-randomized studies of interventions. BMJ. 2016;(355):i4919. doi: 10.1136/bmj.i4919 [Crossref]
