Rev Bras
Fisiol Exerc. 2023;22:e225384
REVIEW
Effects of exercise on individuals with chronic kidney disease: an
evidence gap map
Efeitos do exercício
em indivíduos com doenças renais crônicas: um mapa de evidências
Leticia Gimenes dos Santos
de Moura¹, Thatiane Lopes Valentim Di Paschoale
Ostolin1
1Universidade Federal de São Paulo,
Santos, São Paulo, Brazil
Received: January 11, 2023; Accepted: February 20, 2023.
Correspondence: Thatiane Lopes Valentim Di Paschoale Ostolin, thatiane.ostolin@unifesp.br
Como citar
Moura LGS, Ostolin TLVP. Effects of exercise on individuals with
chronic kidney disease: an evidence gap map. Rev Bras Fisiol
Exerc. 2023;22:e225384. doi:
10.33233/rbfex.v22i1.5384
Abstract
Introduction: Despite compromised exercise capacity and quality of
life, patients with chronic kidney disease (CKD) are extremely inactive. Thus,
exercise plays an essential role in disease management and has been strongly
recommended, regardless of disease severity. Mapping the main evidence about
this topic allows an evidence-based practice. Objective: To summarize
the effects of exercise-based interventions prescribed for patients with CKD by
producing an evidence gap map. Methods: After a comprehensive search in
electronic databases, the eligible studies were analyzed by two reviewers. The
data was extracted and plotted into a matrix linking interventions and
outcomes. The narrative synthesis included only the findings of the studies
published in the last five years. The confidence level was assessed as
recommended. Results: In total, 75 reviews published between 2005 and
2022 were included in the map, but only 50 were described in the narrative
synthesis. We found 179 associations, especially positive, based on the
analysis of plotting 20 interventions categorized into seven groups and 27
outcomes categorized into 13 groups. Negative, potentially negative, and
adverse effects were not reported, which indicates that exercise is safe for
patients with CKD. Conclusion: The mapped evidence was mainly high
confidence level, corroborating the role of prescribing exercise for patients
with CKD as a safe and positively effective intervention for multiple outcomes
with highlights for physical fitness, clinical outcomes, quality of life and
wellbeing.
Keywords: kidney diseases; exercise; evidence-based practice.
Resumo
Introdução: A despeito do comprometimento da
capacidade funcional e redução de qualidade de vida, pacientes com doença renal
crônica (DRC) são extremamente inativos. Sendo assim, o exercício apresenta
papel essencial no manejo da doença e tem sido fortemente recomendado,
independentemente da severidade da doença. Mapear as principais evidências
sobre a temática oportuniza a prática baseada em evidências. Objetivo:
Sumarizar os efeitos de intervenções baseadas em exercícios físicos em
pacientes com DRC a partir da elaboração de um mapa de evidências. Métodos:
Após busca abrangente nas bases de dados, os estudos elegíveis foram analisados
por duas revisoras. Os dados foram extraídos e plotados em uma matriz
associando intervenções e desfechos. A síntese narrativa incluiu somente os
achados relativos aos estudos de revisão publicados nos últimos cinco anos. O
nível de confiança foi avaliado conforme recomendado. Resultados: Ao
todo, 75 estudos de revisão publicados entre 2005 e 2022 foram incluídos no
mapa, porém apenas 50 foram descritos na síntese narrativa. Encontramos 179
associações, principalmente positivas, a partir da análise da plotagem de 20
intervenções categorizadas em sete grupos e 27 desfechos em 13 grupos. Não
foram reportados efeitos negativos, potencialmente negativos ou adversos,
sugerindo que a prática de exercício é segura para pacientes com DRC. Conclusão:
As evidências mapeadas apresentam, em sua maioria, alto nível de confiança,
corroborando o papel da prescrição do exercício para pacientes com DRC como
intervenção segura e com efeitos majoritariamente positivos para múltiplos
desfechos, com destaque para aptidão física, desfechos clínicos, e qualidade de
vida e bem-estar.
Palavras-chave: nefropatias; exercício físico; prática
clínica baseada em evidências.
Introduction
Chronic kidney disease (CKD) is a clinical syndrome
with slow and progressive evolution resulting from irreversible morphofunctional alteration of the kidney for more than
three months [1]. It can be classified into five stages according to the
glomerular filtration rate (G1-G5), three according to albuminuria (A1-A3), and
three groups (i.e., pre-dialysis, dialysis, and transplantation) [1,2].
Treatment and control of risk factors for their development (i.e., diabetes,
hypertension, obesity, cardiovascular disease, and smoking) are the main ways
to prevent disease [3].
Worldwide, more than 850 million people have CKD,
which is responsible for 2.4 million deaths annually [4]. CKD is part of
noncommunicable chronic diseases with a silent development, increased
prevalence, high mortality, and high costs for health systems worldwide [3].
Its prevalence in the Brazilian population is still uncertain, but it is
estimated that 3 to 6 million Brazilians have CKD [5]. This population has a
mortality rate of 15 to 30 times higher than healthy individuals due to the
impairment of 60-65% of the functional capacity with a consequent lower quality
of life [6]. Commonly, there is the presence of multiple symptoms (i.e.,
restless leg syndrome, sleep disorder, depression, anxiety, muscle cramps,
fatigue) that may be associated with metastatic cancer [7].
One of the most frequent complaints of patients is the
reduction of functional exercise capacity manifested by decreasing exercise
tolerance and reducing performance in daily life activities [8]. Both the
hemodialysis procedure (HD) and uremic myopathy are associated with the
breaking of muscle proteins that affects peripheral and proximal muscles and,
consequently, physical capacity [8].
Recently, exercise has been considered a first-rate
treatment for various chronic diseases, including psychiatric, neurological,
metabolic, cardiovascular, pulmonary disease, and musculoskeletal disorders,
and cancer [9]. Given this scenario, exercise has been successfully used as an
adjuvant treatment in improving CKD and reducing its progression [10]. Among
the benefits of exercise programs for patients with CKD and transplanted, the
improvement of functional exercise capacity and quality of life stand out,
regardless of the type of exercise, intensity, or duration of intervention
[11]. Since CKD patients are extremely inactive, exercise promotes positive
cardiovascular effects, as well as improves the efficacy of dialysis [12].
Thus, patients with CKD should be encouraged to exercise and increase their
physical activity levels [10]. However, there may be differences in results
according to the stage of the disease and dialysis or transplantation, which
suggests the need for study designs based on the prescription of a wide variety
of exercises and the importance of evidence-based practice [13].
Given the diversity of exercise, physical activity,
and body practices, as well as prescription strategies, sector or service, and
supervision/guidance, the evidence gap map allows mapping the effects of
physical exercise in patients with CKD considering different contexts [14]. The
map provides friendly access to existing knowledge, contributing to
professional updates/training and favoring evidence-based practice [14]. In
addition to pointing out the role of physiotherapy professionals in hemodialysis
and nephrology services, this professional can contribute as a member of the
team in healthcare setting and, hence, reduce healthcare costs of this service
according to their skills, especially the prescription of exercises [15].
Therefore, this evidence gap map aimed to summarize
the effects of exercise-based interventions prescribed for patients with CKD.
Methods
This evidence gap map is based on the methodology
developed by the International Initiative for Impact Evaluation (3IE) and adapted
by the Latin American and Caribbean Center on Health Sciences Information in
the Pan American Health Organization and the World Health Organization
(Bireme/PAHO/WHO [16]. Accordingly, it is a method of evidence synthesis based
on the review of specific area/thematic literature reviews, followed by the
development of an evidence matrix from the plot of interventions and outcomes
[14]. Although previously written according to the recommendations, the
protocol was not registered elsewhere. However, consultation with the protocol
can be performed upon request to the authors responsible for the study. The
scope of the study was defined through the acronym PCC, as described below:
Population or problem: Patients with CKD, regardless
of sex, race-ethnicity, age, socioeconomic status, education, and presence of
associated comorbidities;
Concept: Multiple and/or nonspecific outcomes in
health;
Context: Interventions based on physical exercises,
regardless of the modality, frequency, duration of the session and/or the
intervention, intensity, public or private sector, and level of health care.
Information sources
Potentially eligible citations were identified and
recovered from the searches conducted in the electronic databases Cochrane
Library, Physiotherapy Evidence Database, PubMed, and Virtual Health Library on
April 26, 2022.
Search strategy
The search strategy was elaborated by one of the
reviewers (TLVDPO) to provide a comprehensive and understanding search of the
literature. The descriptors and alternative terms were defined and selected in
English and Portuguese after consulting the health descriptors (DECS/Mesh):
population or problem (kidney failure, kidney failure, chronic renal
insufficiency, chronic renal failure, and their respective terms Alternatives)
and context (exercise, exercise therapy, breathing exercise, exercise, and movement
techniques, muscle stretching exercises, high-intensity interval training, and
their respective alternative terms). Having seen the interest in mapping
multiple outcomes, no terms regarding outcomes were included. Although there
are no restrictions on the date of publication, we use filters (i.e., type of
study and language) when available in order to identify review studies of
interest.
Eligibility criteria
We considered eligible: (1) Systematic review studies
(systematic reviews with or without meta-analysis, and overview systematic
review) available in full text (2), which (3) evaluated the effects of
exercise-based interventions for (4) patients with CKD, regardless of age, sex,
race-ethnicity, socioeconomic status, education and presence of associated
comorbidities. Primary studies, letters to the editor, opinion articles,
comments, publications from annals of congresses, and ongoing review protocols
were excluded.
There was no restriction on the date of publication,
but only systematic review studies published in English, Portuguese, and
Spanish were included. The option for language restriction was a choice of
reviewers to minimize possible evidence interpretation errors due to language
barriers.
Evidence selection
The analysis and selection of the studies occurred
through the Rayyan application for bibliographic management. Two independent
reviewers (TLVDPO, LGDSDM) screened titles and abstracts. After the resolution
of disagreements by consensus and verification of eligibility from consultation
with the full text, ineligible studies were excluded. Citations of studies
considered potentially relevant by at least one reviewer were analyzed through
the full text.
Extraction and analysis of data
Data extraction and analysis were performed by two
reviewers (TLVDPO, LGDSDM) in a standardized excel spreadsheet and according to
the protocol previously elaborated at the beginning of the review. The
characterization data of the review studies (i.e., study title, year and country
of publication, type, and design of the review) and main interventions,
outcomes, and effects (i.e., no effect, not reported, potentially negative,
negative, inconclusive, potentially positive, positive) were extracted from the
reading of the full text.
After completing data extraction, the categories and
subcategories of interventions and outcomes were defined based on the
literature on the subject. The results were analyzed and reported in an
evidence matrix based on plotting interventions and outcomes. The concentration
and quality of the evidence were presented according to different colors and
graphic elements. Finally, the interactive version of the evidence map was
built using the Tableau ® tool.
Evidence quality assessment
The methodological quality assessment of the included
review studies was performed by two reviewers (TLVDPO, LGdSdM)
using the instrument A MeaSurement Tool to Assess
Systematic Reviews (AMSTAR 2) [17]. Studies that did not meet the requirements
of this instrument were not included in this map to avoid reporting evidence
without assessing the confidence level.
Results
A total of 495 potentially eligible citations were
identified, but only 75 studies were included in the map after screening and
verification of eligibility (Figure 1). The map in its interactive version is
available in the evidence map.
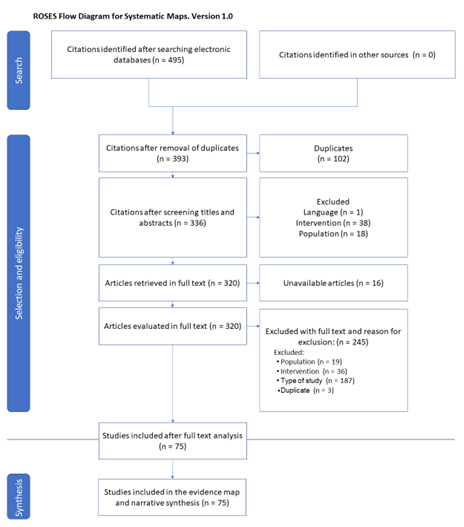
Source: adaptation of the Reporting standards for
Systematic Evidence Syntheses recommendation [18].
Figure 1 - Evidence map flowchart
We analyzed publications between 2005 and 2022 with a
predominance of systematic review and meta-analysis studies (n = 37), which
mostly evaluated effectiveness (n = 65). Additionally, we included six
meta-analysis studies, 27 systematic review studies, and four Cochrane-type
systematic reviews. The narrative synthesis privileged the publications of the
last five years (n = 50).
Focus countries indicate where the primary studies
included in the reviews were conducted. Among them, we observed 45 countries in
23 studies, with emphasis on Brazil (n = 10), China (n = 14), Australia (n =
6), Canada (n = 3), United States of America (n = 3), Japan (n = 2), and Taiwan
(n = 2). We emphasize that we did not analyze the primary studies included in
the systematic reviews. Therefore, data from the same primary study may have
been systematized in more than one review. Thus, the analysis of the amount and
concentration of evidence must be done with caution.
Target population
The study sample consisted mainly of adults (n = 40),
with only three studies with patients of all ages and seven that did not inform
age or age group. As for sex, only one study focused on male participants,
while 19 studies included patients of both sexes (n = 19), and another 30 did
not report whether included only males or females or both of them.
Patients with CKD covered all stages of
classification, hemodialysis, and kidney transplants. Additionally, patients
with restless legs syndrome (n = 3), overweight or obesity (n = 1), diseases
related to oxidative stress (n = 1), and hypertension (n = 1) were evaluated.
Unfortunately, there were no considerations related to race-ethnicity,
socioeconomic status, or other health inequities.
Interventions and outcomes
The 50 studies included in the narrative synthesis
evaluated the effect of 20 types of interventions divided into seven groups:
Stretching, Physical Activity, Physical Activity and Exercise, Exercise,
Combined and/or Multimodal Intervention, Integrative and Complementary
Practices, and Others. These interventions were associated with 27 health
outcomes distributed into 13 groups: Physical Fitness, Muscular Fitness,
Anthropometric and Body Composition Outcomes, Clinical Outcomes,
Epidemiological Outcomes, Renal Outcomes, Fatigue, Level of Physical Activity,
Quality of Life and Well-being, Mental Health, Optimization of Dialysis,
Adverse Effects, and Others.
Overall, there were 179 associations between
interventions and outcomes. It is important to highlight that the same
intervention can be applied to more than one outcome and vice versa. The
Physical Exercise intervention group was the most associated (127
associations), followed by the Combined and/or Multimodal Intervention group
(31 associations). Among the outcomes, the Physical Fitness group received 39
associations, while Clinical outcomes had 26 associations, and Quality of Life
and Well-being received 25 associations.
Effects of interventions on outcomes
The effects of the interventions were mainly positive
(88 associations) and potentially positive (38 associations). However, we found
inconclusive effects (35 associations), as well as interventions without effect
(16 associations). No study reported a negative or potentially negative effect
for the analyzed interventions. The main associations found were highlighted in
Table I.
We observed a positive effect mainly for physical
fitness (32 associations), quality of life (10 associations), cardiovascular
outcomes (8 associations), muscular fitness (7 associations), restless legs
syndrome (6 associations), and depression (5 associations). For potentially
positive effects, the most frequent outcomes were quality of life (9
associations) and muscle fitness (5 associations). There were more inconclusive
effects for physical fitness and quality of life and well-being (4
associations), cardiovascular outcomes (3 associations), and musculoskeletal
outcomes (4 associations).
Table I - Main associations between interventions and
outcomes based on the evidence map analysis
Exercise-based interventions had no negative effects,
but we observed 35 associations with inconclusive effects. Additionally, no
exercise-related adverse effects have been reported for patients with CKD.
Confidence level
Regarding the critical appraisal analysis, studies
were classified as high (n = 34; 68%), moderate (n = 9; 18%), low (n = 5; 10%),
or critically low confidence level. (n = 2; 4%).
Lastly, the associations between interventions and
outcomes can be observed according to the effect found and the level of
confidence obtained through the application of AMSTAR 2 (Table II).
Table II - Associations between interventions and outcomes
according to effect and confidence level
Discussion
The present study developed an interactive evidence
gap map on the effects of exercise-based interventions prescribed for patients
with CKD. Overall, 50 review studies were included in the narrative synthesis
of this evidence gap map and reported a variety of exercise modalities
prescribed for patients with CKD.
Exercise-based interventions were mostly effective and
can be considered safe, while no significant negative and/or adverse effects
were reported. Therefore, the evidence map contributes to understanding the
role of these interventions in the healthcare of patients with CKD, favoring
the translation of knowledge and the identification of important gaps to be
investigated.
The general characterization showed a higher
proportion of systematic reviews and meta-analyses (56%) [19-46], whose sample
consisted of adults. The restricted approach of participants from a wide age
group and/or children is compatible with the greater concentration of
epidemiological data in adults [47] between 20-65 years [5]. This situation
limits the recognition and even the management of CKD in earlier stages, which
tends to result in case studies with renal impairment at an advanced stage
[47,48]. It should be added that studies on CKD are carried out mainly after
the start of dialysis treatment or transplantation, despite CKD being
associated with risk factors, which include health inequalities among them
[49]. Additionally, this population has a high mortality, i.e., approximately
50% of the elderly survive about five years after starting dialysis [50]. These
points may contribute to explaining the profile of patients analyzed in the
studies.
All CKD classification stages were analyzed, dependent
or not on dialysis and kidney transplant recipients. A previous study pointed
out that the studies are mainly focused on patients with end-stage CKD who
undergo regular dialysis [48], and preferably the exercise protocols occurred
within the first two hours after the start of dialysis to avoid cardiovascular
instability [35]. This point may justify our findings as only ten included
studies were performed with patients without dialysis or kidney transplantation
[23,27,28,30,31,37,40,48,51,52] and three did not make it clear whether the
studied population was or not dependent on renal replacement therapy
[29,44,53]. In patients without dialysis treatment (pre-dialysis) or
transplanted, combined aerobic and exercises have a potential effect in
delaying the deterioration of renal function [30].
Literature was prominently published in China
[19,36,41,48,54] and Brazil [33, 34,38,43,46,55,56]. Brazil is a prominent
country on the global stage since presents one of the largest populations on
chronic outpatient dialysis and one of the highest rates of annual kidney transplants.
Thus, CKD is a relevant public health problem with increasing prevalence
worldwide, but it is getting worse in countries like China and Brazil due to
the rapid demographic transition associated with the persistence of economic,
health, and social inequalities [5,57]. Still, CKD may be associated with risk
factors, such as sociodemographic conditions, lifestyle, and chronic diseases
[49], which may also justify the greater literature in these regions.
Multiple interventions were found, and hence,
different outcomes. These findings may be associated with a high burden of
symptoms observed in these patients [7]. According to a previous systematic
review, about thirty symptoms are prevalent in patients with CKD, which may
vary according to the stage of the disease [7]. It is also important to
consider the methodology adopted, which favors the analysis of comprehensive
evidence, especially in comparison with the specificity of systematic reviews,
for example.
Among the interventions, the modality of aerobic
exercises combined with resistance exercises presented the most evidence
[8,23,24,27,28,35,36,43,46,48,56,58]. This exercise modality has been strongly
recommended for promoting positive effects on functional exercise capacity,
muscle function, body composition, restless legs syndrome, sleep quality,
fatigue, quality of life, inflammatory markers, depressive symptoms, and blood
pressure [8,23,24,27,28,35,36,43,46,48,56,58,59]. As expected, multicomponent
exercise tends to have a wide range of physiological and psychosocial effects,
given that it combines different exercise modalities. It should be added that
these findings are consistent with the recent literature, especially focused on
exercises prescription for middle-aged and elderly individuals, intending to
offer more comprehensive and potentially effective interventions.
In our study, we found 25 associations related to
clinical outcomes, which include cardiovascular and musculoskeletal outcomes,
especially when aerobic exercise was prescribed. Exercises have been strongly
suggested for patients with CKD, mainly due to the positive antihypertensive
effects even in shorter interventions (i.e., less than six months in duration),
which can lead to a reduction of 5.61 mmHg in systolic pressure and 2.87 mmHg
in stages 2-5 of non-dialysis patients [48]. In patients with CKD stages 3-4,
in contrast, there is an effect of aerobic exercise on the estimated glomerular
filtration rate and exercise tolerance, although limited, but not on blood pressure
[44]. However, the findings must be analyzed with caution due to the confidence
level being considered low to moderate. Despite this, the findings reiterate
previous recommendations available in the KDIGO Clinical Practice Guideline
(2021) on Blood Pressure Management in CKD, which suggest that patients with
elevated BP and CKD be advised to perform moderate-intensity physical activity
for at least 150 minutes a week [60].
Another aspect worth mentioning concerns the
association between CKD and obesity. In this study, we found 39 associations
between exercise and physical fitness, 11 associations with anthropometric and
body composition outcomes, 14 cardiovascular outcomes, and four related to
inflammatory markers, among others. These associations are closely related to
obesity in patients with CKD, with a greater number of positive associations
related to aerobic exercise and the combination of aerobic and resistance
exercise [8,23,25,27,28,33-37,39-41,43,44,46,48,51,52,54-56,58,61-64].
We found 88 associations with positive effects after
exercises performed during hemodialysis or on days without dialysis
[8,21-24,27-29,32,34-37,39,41,43,44,46,48,51,53-56,58,59,61-66]. Heiwe and Jacobson [13] emphasize that exercise should be
one of the care components for adults receiving dialysis, especially for
cardiovascular risk factors management. Additionally, it should be mentioned
that aerobic capacity is improved by regular exercise training programs,
regardless of the type of exercise, intensity, or duration of intervention
[13]. Any training modality performed for 2 to 12 months can significantly
improve depression and functional exercise capacity, contributing to a better
prognosis and survival of adults undergoing dialysis [50].
Three studies evaluated the association between
exercise and telehealth with positive effects for outcomes such as physical
fitness [64]. Stevenson et al. [67] reported that the use of a physical
activity monitoring application (step count) does not promote statistically
significant effects for increasing the level of physical activity but favors
the management of dietary sodium intake and fluid management. It is important
to highlight that this evidence is of low quality, with inconclusive effects
due to methodological limitations, as well as the heterogeneity of modalities
and types of interventions [67]. Conversely, the combination of aerobic
exercise and virtual reality, results in positive and potentially positive
effects on quality of life [64], regardless of the exercise modality [64].
Telehealth has been widely investigated and considered a potential strategy to
reduce costs, expand access to health care, provide opportunities for chronic
conditions management, and promote a more active and healthier lifestyle. Although
it was not the focus of the mapping proposed in this study, determining its
applicability to patients with CKD is an important perspective to be analyzed
in the future, both in primary and secondary studies.
Respiratory muscle training was evaluated in 4
studies, and it showed positive effects on respiratory muscle function,
psychosocial outcomes, biochemical markers, functional exercise capacity,
adequacy of dialysis, and aerobic capacity [34,62,65], in addition to
potentially promoting effects positive concerning the quality of life [22] in
the absence of adverse events [62].
Regarding physical activity, a systematic review and
meta-analysis study demonstrated that increased physical activity levels were
associated with reduced mortality in patients with end-stage CKD treated with
hemodialysis [20]. However, the authors point out that the scarcity of
well-designed, controlled, and randomized clinical trials with a sufficient
number of participants compromises the generalizability of the findings [20].
It is relevant to mention that the definition of the search strategy, although
comprehensive, may have privileged the identification of interventions that
emphasized the prescription of exercises to the detriment of the promotion of
the physical activity. Similarly, the search strategy may have limited the
publications related to body practices. Although this has been minimized by the
adoption of highly inclusive eligibility criteria, it would be interesting to
improve and deepen the search for evidence related to these types of
interventions.
Five studies reported that exercise performed in
exercise centers and/or at home had positive effects on quality of life
[59,66]. Concerning anxiety and depression, these interventions lead to potentially
positive effects [24]. A recent study conducted in the United States observed
positive effects of home-based exercise on frailty in patients with end-stage
CKD, including improvement in muscle strength, walking speed, level of physical
activity, depression, and weight loss [68]. It is necessary to consider that
35% of patients with CKD are frail, being eligible for kidney transplantation
[68]. However, the long wait for the transplant leads to ineligibility as these
individuals become more fragile [68]. Some patients report a fear of exercising
during dialysis, but the literature is still limited about home-based exercises
for this population [50]. In this sense, Sheng et al. [69] suggest greater
viability of intradialytic exercise, minimizing the occurrence of complications
and reducing the dropout rate as it does not require extra time for training.
We found 14 associations between exercise and
cardiovascular outcomes [36,40,41,43-45,48,56,61,63,64]. A recent
meta-analysis reported that 463 million adults are currently living with
diabetes worldwide, i.e., 1 in 11 adults aged 20 to 79 years have diabetes
[53]. Among these subjects, 35% may develop end-stage CKD after five years, and
18% will die from diabetic nephropathy within 20 years [53]. Given this
scenario, physical activity has a protective effect and may delay the
progression of diabetic nephropathy [53]. Similarly, a systematic review
reinforced the importance of exercise for this population, especially for
reducing mortality related to cardiovascular events [61]. Additionally, a
meta-analysis showed that exercise is a potential strategy in the prevention
and treatment of numerous health conditions, including CKD [19].
Restless legs syndrome (i.e., a movement disorder
characterized by a strong urge to move the limbs, especially the legs, which
may present with dysesthesias, exacerbated at night or during periods of
inactivity) is common in patients with end-stage CKD, significantly affecting
sleep quality and, hence, increasing the risk of developing depression and
anxiety [24]. Among the included studies, three studies evaluated the effects
of exercise in relieving symptoms of restless legs syndrome and found positive
effects from interventions of intradialytic stretching and regular aerobic
exercises [21,32]. Likewise, the combination of aerobic and resistance exercise
also had positive effects on this outcome [24].
Three studies reported an inconclusive effect
[20,28,64], and four did not observe significant effects [21,41,62,63]. In
contrast, no studies reported adverse events (i.e., any injury or disease
exacerbation attributed to the exercise regimen), which could include
headaches, hypotension, angina, or even fistula-related problems. This evidence
reinforces the role of exercise in the care of patients with CKD, as it is a
widely effective and safe intervention.
A previous review study described how challenging it
is for dialysis center staff to promote regular exercise practice, as only 25%
of patients can exercise without any difficulty [70]. In addition, the health
services routine makes counseling by the team incipient and irregular, which
perpetuates the lack of knowledge of the benefits and types of exercise that
can be performed by patients [70]. Another important point to be analyzed is
that, despite the positive and relevant results, few hemodialysis services have
physiotherapists in their CKD care team. Thus, the evidence described warns
against underestimating the contribution of this professional in hemodialysis
clinics and nephrology services [71]. This scenario may also be associated with
the high annual expenses for hemodialysis and peritoneal dialysis in Brazil,
with 75% of the population depending exclusively on the SUS [72].
Given current trends of the increasing prevalence of
CKD, it is imperative to carry out economic evaluation studies in this area to
provide a greater understanding of the cost-effectiveness of interventions and
encourage the adoption of preventive actions, early diagnosis, and treatment of
CKD [73]. Lastly, more studies are needed that include a wide age range and
race-ethnicity, sex, health condition, social capital, and education, among
other health inequalities, thus providing opportunities for the elaboration and
implementation of a health agenda that meets the real demands of countries with
marked social inequality, such as Brazil.
Limitations and strengths
This evidence gap map is mostly clinical due to the
scope of the study and methodological choices. However, it may be a limitation
of the current literature that tends to emphasize and reproduce the biomedical
model to the detriment of the biopsychosocial model. Given this scenario, the
findings are restricted, which may compromise the applicability of the map
concerning health management.
This study does not describe the duration of
interventions, intensity, frequency, volume, and progression of exercises. This
information can be found in the full text of the primary studies included in
the analyzed review studies. The evidence map does not assess the risk of bias.
However, this limitation was minimized through the use of AMSTAR 2 for critical
appraisal evaluation. Despite the expressive number of studies with a high
level of confidence, possibly related to the choice of population and the
number of Cochrane-type review studies included, the use of AMSTAR 2 evidences
the need to improve the development of protocols for literature reviews, as
well as their conduction and description of the main findings, regardless of
the performance of meta-analysis.
This study has several strengths that deserve to be
highlighted. Among them is the ability to access evidence on exercise-based
interventions for patients with CKD and their main clinical outcomes in a
user-friendly graphical presentation. Although it does not have statistical
analysis, access to studies is provided through hyperlinks. Additionally, the
findings were accompanied by the confidence level, contributing to the critical
analysis of the evidence and, hence, clinical decision-making. Finally, it is
worth considering that the map favors the identification of knowledge gaps,
which may be the subject of future studies.
Recommendations
Given the current scenario, the regular practice of
exercises has been strongly recommended due to its physiological and
psychosocial benefits, mainly for chronic disease treatments such as CKD,
regardless of severity. Therefore, the evidence reiterates the role of exercise
in the care of these patients and highlights the need to encourage the
implementation of exercise programs for this population and encourage increase
levels of physical activity. Additionally, the regulation of the participation of
the physiotherapy professional as a member of the multidisciplinary team in
nephrology centers is imperative and may have a substantial impact on health
expenses, reduction of the accelerated progression of the disease, and,
consequently, the reduction of morbidity and mortality in this population.
Conclusion
Evidence supports the recommendation of exercise
prescriptions for patients with CKD. In general, we observed mostly positive
and potentially positive associations between different types of regular
intradialytic, interdialytic, and home exercise for clinically relevant
outcomes, such as physical fitness, cardiovascular outcomes, mental health, and
quality of life, regardless of CKD severity. Finally, we found no negative
effects or adverse events reported for this population.
Potential conflict of interest
No conflicts of interest potentially relevant to this
article were reported.
Financing source
There were no external funding sources for this study.
Authors' contribution
Conception and design of the research: Ostolin TLVDP, Moura LGS; Data collection: Ostolin TLVDP, Moura LGS; Data analysis and interpretation:
Ostolin TLVDP, Moura LGS; Manuscript writing: Moura
LGS; Critical review of the manuscript for important intellectual content: Ostolin TLVDP
References
- KDIGO 2020. Clinical practice guideline for diabetes management in
chronic kidney disease. Kidney Int. [Internet]. 2020 [cited 22 Jul 22].
Available from: https://www.elsevier.com/books-and-journals/
- Ammirati AL. Chronic
kidney disease. Rev Assoc Med Bras. 2020;66(1):3-9. doi: 10.1590/1806-9282.66.S1.3 [Crossref]
- Brasil. Ministério da Saúde.
Doenças renais crônicas. [Internet]. [cited 2022 Jul 22]. Available from:
https://www.gov.br/saude/pt-br/assuntos/saude-de-a-a-z/d/drc
- Brasil. Ministério da Saúde.
12/3: Dia mundial do rim. Biblioteca Virtual em Saúde MS [Internet]. [cited
2022 Jul 25]. Available from:
https://bvsms.saude.gov.br/12-3-dia-mundial-do-rim/
- Marinho AGBW, Penha AP, Silva MTS, Galvão TF. Prevalência de doença renal crônica em adultos no Brasil: revisão sistemática da literatura. Cad Saúde Coletiva. 2017;25(3):379-88. doi: 10.1590/1414-462X201700030134 [Crossref]
- Barcellos FC, Santos IS, Umpierre D, Bohlke M, Hallal PC. Effects of exercise in the whole spectrum of chronic kidney disease: a systematic review. Clin Kidney J. 2015;8(6):753. doi: 10.1093/ckj/sfv099 [Crossref]
- Almutary H, Bonner A,
Douglas C. Symptom burden in chronic kidney disease: a review of recent
literature. J Ren Care. [Internet]. 2013 [cited 2022 nov
9];39(3):140-50. Available from:
https://onlinelibrary.wiley.com/doi/full/10.1111/j.1755-6686.2013.12022.x
- Ibrahim AA, Althomali OW, Atyia MR, Hussein HM, Abdelbasset WK, Eldesoky MTM, et al. A systematic review of trials investigating the efficacy of exercise training for functional capacity and quality of life in chronic kidney disease patients. Int Urol Nephrol. 2022];54(2):289-98. doi: 10.1007/s11255-021-02917-4 [Crossref]
- Pedersen BK, Saltin B. Exercise as medicine - Evidence for prescribing exercise as therapy in 26 different chronic diseases. Scand J Med Sci Sports. 2015;25:1-72. doi: 10.1111/sms.12581 [Crossref]
- Wilkinson TJ, Shur NF, Smith AC. “Exercise as medicine” in chronic kidney disease. Scand J Med Sci Sports. 2016;26(8):985-8. doi: 10.1111/sms.12581 [Crossref]
- Heiwe S, Jacobson SH. Exercise training in adults with CKD: A systematic review and meta-analysis. Am J Kidney Dis. 2014;64(3):383-93. doi: 10.1053/j.ajkd.2014.03.020 [Crossref]
- Sheng K, Zhang P, Chen L, Cheng J, Wu C, Chen J. Intradialytic exercise
in hemodialysis patients: A systematic review and meta-analysis. Am J Nephrol.
2014;40(5):478-90. doi: 10.1159/000368722 [Crossref]
- Heiwe S, Jacobson SH. Exercise training in adults with CKD: A systematic review and meta-analysis. Am J Kidney Dis. 2014;64(3):383-93. doi: 10.1053/j.ajkd.2014.03.020 [Crossref]
- Snilstveit B, Vojtkova M, Bhavsar A, Stevenson J, Gaarder M. Evidence & Gap Maps: A tool for promoting evidence informed policy and strategic research agendas. J Clin Epidemiol. 2016;79:120-9. doi: 10.1016/j.jclinepi.2016.05.015 [Crossref]
- COFFITO. Conselho Federal de
Fisioterapia e Terapia Ocupacional Resolução No424, de 08 de julho de 2013.
- Fundação Oswaldo Cruz.
Sumário de Mapas de Evidências: metodologia e aplicação [Internet]. [cited
2022 Jul 23]; Available from: https://cursos.campusvirtual.fiocruz.br/local/meucampus/courseinfo.php?id=343
- Shea BJ, Reeves BC, Wells G, Thuku M, Hamel C, Moran J, et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomized or non-randomized studies of healthcare interventions, or both. BMJ. 2017;358:4008. doi: 10.1136/bmj.j4008 [Crossref]
- Haddaway NR, Macura B, Whaley P, Pullin AS. ROSES RepOrting standards for Systematic Evidence Syntheses: pro forma, flow-diagram and descriptive summary of the plan and conduct of environmental systematic reviews and systematic maps. Environ Evid. 2018;7:7. doi: 10.1186/s13750-018-0121-7 [Crossref]
- Lu Z, Xu Y, Song Y, Bíró I, Gu Y. A mixed comparison of different intensities and types of physical exercise in patients with diseases related to oxidative stress: a systematic review and network meta-analysis. Front Physiol. 2021;12:700055. doi: 10.3389/fphys.2021.700055 [Crossref]
- Thangarasa T, Imtiaz R, Hiremath S, Zimmerman D. Physical activity in patients treated with peritoneal dialysis: a systematic review and meta-analysis. Can J Kidney Health Dis. 2018;5:1-13. doi: 10.1177/205435811877982 [Crossref]
- Chen JJ, Lee TH, Tu YK, Kuo G, Yang HY, Yen
CL, et al. Pharmacological and nonpharmacological treatments for restless legs
syndrome in end stage kidney disease: a systematic review and component network
meta-analysis. Nephrol Dial Transplant. [Internet] 2021 [cited 2022 Jul 23].
Available from: https://pubmed.ncbi.nlm.nih.gov/34612498
- Hu H, Liu X, Chau PH, Choi EPH. Effects of intradialytic exercise on health-related quality of life in patients undergoing maintenance haemodialysis: a systematic review and meta-analysis. Qual Life Res. 2022;31(7):1915-32. doi: 10.1007/s11136-021-03025-7 [Crossref]
- Villanego F, Naranjo J, Vigara LA, Cazorla JM, Montero ME, García T, et al. Impacto del ejercicio físico en pacientes con enfermedad renal crónica: revisión sistemática y metaanálisis. Nefrología. 2020;40(3):237-52. doi: 10.1016/j.nefro.2020.01.002 [Crossref]
- Hargrove N, el Tobgy N, Zhou O, Pinder M, Plant B, Askin N, et al. Effect of aerobic exercise on dialysis-related symptoms in individuals undergoing maintenance hemodialysis: a systematic review and meta-analysis of clinical trials. Clin J Am Soc Nephrol. 2021;16(4):560-74. doi: 10.2215/CJN.15080920 [Crossref]
- Lu Y, Wang Y, Lu Q. Effects of exercise on muscle fitness in dialysis patients: a systematic review and meta-analysis. Am J Nephrol. [Internet] 2019;50(4):291-302. doi: 10.1159/000502635 [Crossref]
- Ferreira TL, Ribeiro HS,
Ribeiro ALA, Bonini-Rocha AC, Lucena JMS, Oliveira PA, et al. Exercise
interventions improve depression and anxiety in chronic kidney disease
patients: a systematic review and meta-analysis. Int Urol
Nephrol. [Internet] 2021 [cited 2022 Jul 23];53(5):925-33. Available from:
https://pubmed.ncbi.nlm.nih.gov/32869171/
- Wu L, Liu Y, Wu L, Yang J, Jiang T, Li M. Effects of exercise on markers of inflammation and indicators of nutrition in patients with chronic kidney disease: a systematic review and meta-analysis. Int Urol Nephrol. 2022;54(4):815-26. doi: 10.1007/s11255-021-02949-w [Crossref]
- Nakamura K, Sasaki T, Yamamoto S, Hayashi H, Ako S, Tanaka Y. Effects of exercise on kidney and physical function in patients with non-dialysis chronic kidney disease: a systematic review and meta-analysis. Sci Rep. 2020;10(1):18195. doi: 10.1038/s41598-020-75405-x [Crossref]
- Nantakool S, Rerkasem K, Reanpang T, Worraphan S, Prasannarong M. A systematic review with meta-analysis of the effects of arm exercise training programs on arteriovenous fistula maturation among people with chronic kidney disease. Hemodial Int. 2020;24(4):439-53. doi: 10.1111/hdi.12875 [Crossref]
- Wu X, Yang L, Wang Y, Wang C, Hu R,
Wu
- Yang L, Wu X, Wang Y, Wang C, Hu R, Wu Y. Effects of exercise training on proteinuria in adult patients with chronic kidney disease: A systematic review and meta-analysis. BMC Nephrol. 2020;21(1):172. doi: 10.1186/s12882-020-01816-7 [Crossref]
- Huang CW, Lee MJ, Wang LJ, Lee PT, Tu YK, Hsu CW, et al. Comparative efficacy and acceptability of treatments for restless legs syndrome in end-stage renal disease: a systematic review and network meta-analysis. Nephrol Dial Transplant. 2020;35(9):1609-18. doi: 10.1093/ndt/gfz097 [Crossref]
- Schardong J, Stein C, della Méa Plentz R. Neuromuscular electrical stimulation in chronic kidney failure: a systematic review and meta-analysis. Arch Phys Med Rehabil. 2020;101(4):700-11. doi: 10.1016/j.apmr.2019.11.008 [Crossref]
- Ferrari F, Helal L, Dipp T, Soares D, Soldatelli Â, Mills AL, et al. Intradialytic training in patients with end-stage renal disease: a systematic review and meta-analysis of randomized clinical trials assessing the effects of five different training interventions. J Nephrol. 2020;33(2):251-66. doi: 10.1007/s40620-019-00687-y [Crossref]
- Andrade FP, Rezende PS,
- Huang M, Lv A, Wang J, Xu N, Ma G, Zhai Z, et al. Exercise training and outcomes in hemodialysis patients: systematic review and meta-analysis. Am J Nephrol. 2019;50(4):240-54. doi: 10.1159/000502447 [Crossref]
- Peng S, He J, Huang J, Lun L, Zeng J, Zeng S, et al. Self-management interventions for chronic kidney disease: A systematic review and meta-analysis. BMC Nephrol. 2019;20(1):1-13. doi: 10.1186/s12882-019-1309-y [Crossref]
- Ferreira GD, Bohlke M, Correa CM, Dias EC, Orcy RB. Does intradialytic exercise improve removal of solutes by hemodialysis? a systematic review and meta-analysis. Arch Phys Med Rehabil. [Internet] 2019 [cited 2022 Jul 23];100(12):2371-80. doi: 10.1016/j.apmr.2019.02.009 [Crossref]
- Clarkson MJ, Bennett PN, Fraser SF, Warmington SA. Exercise interventions for improving objective physical function in patients with end-stage kidney disease on dialysis: A systematic review and meta-analysis. Am J Physiol Renal Physiol. 2019;316(5):F856–72. doi: 10.1152/ajprenal.00317.2018 [Crossref]
- Thompson S, Wiebe N, Padwal RS, Gyenes G, Headley SAE, Radhakrishnan J, et al. The effect of exercise on blood pressure in chronic kidney disease: A systematic review and meta-analysis of randomized controlled trials. PLoS One. 2019;14(2):e0211032. doi: 10.1371/journal.pone.0211032 [Crossref]
- Pu J, Jiang Z, Wu W, Li L, Zhang L, Li Y, et al. Efficacy and safety of intradialytic exercise in haemodialysis patients: a systematic review and meta-analysis. BMJ Open. 2019;9(1):e020633. doi: 10.1136/bmjopen-2017-020633 [Crossref]
- Salhab N, Karavetian M, Kooman J, Fiaccadori E, el Khoury CF. Effects of intradialytic aerobic exercise on hemodialysis patients: a systematic review and meta-analysis. J Nephrol. 2019;32(4):549-66. doi: 10.1007/s40620-018-00565-z [Crossref]
- Scapini KB, Bohlke M, Moraes OA, Rodrigues
CG, Inácio JF, Sbruzzi G,
et al. Combined training is the most effective training modality to improve
aerobic capacity and blood pressure control in people requiring haemodialysis for end-stage renal disease: systematic
review and network meta-analysis. J
Physiother. [Internet]. 2019;65(1):4-15. Disponível
em:
https://diretoriacientificaicfuc.org.br/wp-content/uploads/2021/07/Combined-training-is-the-most.pdf
- Wyngaert K vanden, van Craenenbroeck AH, van Biesen W, Dhondt A, Tanghe A, van Ginckel A, et al. The effects of aerobic exercise on eGFR, blood pressure and VO2peak in patients with chronic kidney disease stages 3-4: A systematic review and meta-analysis. PLoS One. 2018;13(9):e0203662. doi: 0.1371/journal.pone.0203662 [Crossref]
- Young HML, March DS, Graham-Brown MPM, Jones AW, Curtis F, Grantham CS,
et al. Effects of intradialytic cycling exercise on exercise capacity, quality
of life, physical function and cardiovascular measures in adult haemodialysis patients: a systematic review and
meta-analysis. Nephrology Dialysis Transplantation. [Internet] 2018 [cited 2022
Jul 23];33(8):1436-45. Available from:
https://academic.oup.com/ndt/article/33/8/1436/4955890
- Gomes Neto M, de Lacerda FFR, Lopes AA, Martinez BP, Saquetto MB. Intradialytic exercise training modalities on physical functioning and health-related quality of life in patients undergoing maintenance hemodialysis: systematic review and meta-analysis. Clin Rehabil. 2018;32(9):1189-202. doi: 10.1177/0269215518760380 [Crossref]
- Koch Nogueira PC, Santis Feltran L de, Camargo MF, Leão ER, Benninghoven JR, Gonçalves NZ, et al. Prevalência estimada da doença renal crônica terminal em crianças no Estado de São Paulo. Rev Assoc Med Bras. 2011;57(4):443-9. doi: 10.1590/S0104-42302011000400020 [Crossref]
- Zhang L, Wang Y, Xiong L, Luo Y, Huang Z, Yi B. Exercise therapy improves eGFR, and reduces blood pressure and BMI in non-dialysis CKD patients: Evidence from a meta-analysis. BMC Nephrol. 2019;20(1):1-12. doi: 10.1186/s12882-019-1586-5 [Crossref]
- Kelen de Aguiar LI, Ruscitto Prado III R, Gazzinelli AI, Carvalho Malta DI, Kelen de Aguiar Avenida Professor Alfredo L. Fatores associados à doença renal crônica: inquérito epidemiológico da Pesquisa Nacional de Saúde Factors associated with chronic kidney disease: epidemiological survey of the National Health Survey. Rev Bras Epidemiol. 2020;23. doi: 10.1590/1980-549720200044 [Crossref]
- Bernier-Jean A, Beruni NA, Bondonno NP, Williams G, Teixeira-Pinto A, Craig JC, et al. Exercise training for adults undergoing maintenance dialysis. Cochrane Database of Systematic Reviews. 2022;(1). doi: 10.1002/14651858.CD014653/full [Crossref]
- Yamamoto R, Ito T, Nagasawa Y, Matsui K, Egawa
M, Nanami M, et al. Efficacy of aerobic exercise on the cardiometabolic and
renal outcomes in patients with chronic kidney disease: a systematic review of
randomized controlled trials. J Nephrol 2021;34(1):155-64. doi: 10.1007/s40620-020-00865-3 [Crossref]
- Evangelidis N, Craig J, Bauman A, Manera K, Saglimbene V, Tong A. Lifestyle behaviour change for preventing the progression of chronic kidney disease: a systematic review. BMJ Open. 2019;9(10):e031625. doi: 10.1136/bmjopen-2019-031625 [Crossref]
- Cai Z, Yang Y, Zhang J. Effects of physical activity on the progression
of diabetic nephropathy: a meta-analysis. Biosci Rep
[Internet] 2021 [cited 2022 Jul 23];41(1). Available from:
https://pubmed.ncbi.nlm.nih.gov/33289502/
- Pei G, Tang Y, Tan L, Tan J, Ge L, Qin W. Aerobic exercise in adults with chronic kidney disease (CKD): a meta-analysis. International Urology and Nephrology. 2019;51(10):1787-95. doi: 10.1007/s11255-019-02234-x [Crossref]
- Nicolodi GV, della Méa Plentz R, Righi NC, Stein C. Effects of aerobic exercise on patients with pre-dialysis chronic kidney disease: a systematic review of randomized controlled trials. doi: 101080/0963828820211900929 [Crossref]
- De A, Fernandes O, Alves Y, Sens S, Fonseca Junior PR, Calhes Franco De Moura R, et al. Impacto do uso do cicloergômetro na função respiratória, cardiovascular, capacidade aeróbica, funcional e qualidade de vida de pacientes com doença renal crônica em hemodiálise. Fisioter Bras. 2019;20(2):302-9. doi: 10.33233/fb.v20i2.2220 [Crossref]
- Ferraz FHRP, Rodrigues CIS, Gatto GC, Sá NM. Diferenças e desigualdades no acesso a terapia renal substitutiva nos países do BRICS. Cienc Saude Coletiva. 2017;22(7):2175-85. doi: 10.1590/1413-81232017227.00662017 [Crossref]
- Bakaloudi DR, Siargkas A, Poulia KA, Dounousi E, Chourdakis M. The effect of exercise on nutritional status and body composition in hemodialysis: a systematic review. Nutrients. 2020;12(10):3071. doi: 10.3390/nu12103071 [Crossref]
- Wen X, Wang Y, Zhao Q, Zhang H, Shi H, Wang M, et al. Nonpharmacological interventions for depressive symptoms in end-stage renal disease: a systematic review. West J Nurs Res. 2020;42(6):462-73. doi: 10.1177/0193945919857540 [Crossref]
- KDIGO 2021. Clinical practice guideline for the management of blood pressure in chronic kidney disease. Kidney Int. 2021;99(3S):S1-S87. doi: 10.1016/j.kint.2020.11.003 [Crossref]
- Esmailiyan M, Amerizadeh A, Vahdat S, Ghodsi M, Doewes RI, Sundram Y. Effect of different types of aerobic exercise on individuals with and without hypertension: an updated systematic review. Curr Probl Cardiol. 2021;48(3). doi: 10.1016/j.cpcardiol.2021.101034 [Crossref]
- Bündchen DC, Sousa H, Afreixo V, Frontini R, Ribeiro O, Figueiredo D, et al. Intradialytic exercise in end-stage renal disease: An umbrella review of systematic reviews and/or meta-analytical studies. Clin Rehabil. 2021;35(6):812-28. doi: 10.1177/0269215520986784 [Crossref]
- Valenzuela PL, Morales JS, Ruilope LM, Villa P, Santos-Lozano A, Lucia A. Intradialytic neuromuscular electrical stimulation improves functional capacity and muscle strength in people receiving haemodialysis: a systematic review. J Physiother. 2020;66(2):89-96. doi: 10.1016/j.jphys.2020.03.006 [Crossref]
- Afsar B, Siriopol D, Aslan G, Eren OC, Dagel T, Kilic U, et al. The impact of exercise on physical function, cardiovascular outcomes and quality of life in chronic kidney disease patients: a systematic review. Int Urol Nephrol. 2018;50(5):885-904. doi: 10.1007/s11255-018-1790-4 [Crossref]
- Kowal G, Rydzewski A. The effects of respiratory muscle training in chronic kidney disease patients on haemodialysis and peritoneal dialysis: a review. Medical Studies/Studia Medyczne. 2018;34(1):78-85. doi: 10.5114/ms.2018.74825 [Crossref]
- Natale P, Palmer SC, Ruospo M, Saglimbene VM, Rabindranath KS, Strippoli GFM. Psychosocial interventions for preventing and treating depression in dialysis patients. Cochrane Database Syst Rev. 2019;2019(12). doi: 10.1002/14651858.CD004542.pub3/full [Crossref]
- Stevenson JK, Campbell ZC, Webster AC, Chow CK, Tong A, Craig JC, et al. eHealth interventions for people with chronic kidney disease. Cochrane Database Syst Rev. 2019;8(8). doi: 10.1002/14651858.CD012379.pub2 [Crossref]
- Yoo J, Ruppar T, Wilbur JE, Miller A, Westrick JC. Effects of home-based exercise on frailty in patients with end-stage renal disease: systematic review. Biol Res Nurs. 2022;24(1):48-63. doi: 10.1177/10998004211033031 [Crossref]
- Sheng K, Zhang P, Chen L, Cheng J, Wu C, Chen J. Intradialytic exercise in hemodialysis patients: a systematic review and meta-analysis. Am J Nephrol. [Internet] 2014 [cited 2022 Jul 23];40(5):478-90. doi: 10.1159/000368722 [Crossref]
- Murakami M, Aoki T, Sugiyama Y, Takeuchi M, Yui T, Koyama M, et al. Association between the transtheoretical model approach and sustained intradialytic pedaling exercise: A retrospective cohort study. Medicine. 2021;100(42):e27406. doi: 10.1097/MD.0000000000027406 [Crossref]
- Sanchez HM, Nascimento DMB, Castro K, Sanchez EGM, Melo Junior JP, Agostinho PLS. Benefícios da fisioterapia intradialítica na qualidade de vida, dor, edema e função respiratória de doentes renais crônicos. Fisioter Mov. 2018;31(0). doi: 10.1590/1980-5918.031.AO07 [Crossref]
- Brasil MS. Ministério da
Saúde reajusta valores para tratamento de hemodiálise. [Internet].
[cited 2022 Nov 11]. Available from:
https://www.gov.br/saude/pt-br/assuntos/noticias/2021-1/dezembro/ministerio-da-saude-reajusta-valores-para-tratamento-de-hemodialise
- Alcalde PR, Kirsztajn GM. Gastos do Sistema Único de Saúde brasileiro com doença renal crônica. J Bras Nefrol. 2018;40(2). doi: 10.1590/2175-8239-JBN-3918 [Crossref]
