Rev Bras Fisiol Exerc 2022;21(5):303-11
doi: 10.33233/rbfex.v21i5.5404
ORIGINAL ARTICLE
Reliability and reproducibility of the measurement of different muscle
strength manifestations
Confiabilidade e
reprodutibilidade da medida de diferentes manifestações da força muscular
Daniela Bárbara Moreira
Martins¹, Ítalo Santiago Alves Viana¹, Sandro Fernandes da Silva², Claudia
Eliza Patrocínio de Oliveira1, Osvaldo Costa Moreira¹
1Universidade Federal de Viçosa – Campus
Florestal, Florestal, MG, Brazil
2Universidade Federal de Lavras, Lavras,
MG, Brazil
Received: September 10, 2022; Accepted: November 5, 2022.
Correspondence: Osvaldo Costa Moreira, E-mail:
osvaldo.moreira@ufv.br
How to cite
Martins DBM, Viana
ISA, Silva SF, Oliveira CEP³, Moreira OC. Reliability and reproducibility of the measurement of different muscle
strength manifestations. Rev Bras
Fisiol Exerc. 2022;21(5): 303-11.doi: 10.33233/rbfex.v21i5.5404
Abstract
Introduction: Studies that evaluate the reproducibility of CVIM
and muscle power tests are scarce and often have low practical applicability.
Objective: To evaluate the reliability and reproducibility of tests for
measuring different manifestations of muscle strength. Methods: Nineteen
healthy men, aged 23.36 ± 2.35 years, 1.82 ± 0.06 m and 80.17 ± 11.57 kg, with
no experience with resistance training (RT) and no experience with the test
protocols performed were evaluated. The volunteers were submitted to two
assessments of maximum isometric strength (CVIM), maximum dynamic strength
(1RM), and muscle power, respectively, separated by 72 hours. Results:
For all muscle strength assessment protocols, an intraclass correlation
coefficient (ICC) with high to very high strength of agreement (ICC ≥
0.79) was found. However, all measurements showed a moderate coefficient of
variation (CV): CVIM (CV = 12.0%), mean muscle power at 40%, 60%, and 80% of
the 1RM (CV = 16.2%, 11, 0% and 14.0% respectively) and peak muscle power (PP)
at 60% and 80% of 1RM (CV = 11.8% and 13.3% respectively), except for RM (CV =
6.4%), and PP at 40% of 1RM (CV = 5.8%), with an acceptable measurement
standard error (SEM). Conclusion: The high to very high values for the
ICC indicate an excellent reliability of the measurements in the different
manifestations of muscle strength. However, since the volunteers had no
experience with RT, a familiarization process prior to carrying out the tests
is recommended, in order to improve their reproducibility indicators.
Keywords: health; muscle strength; muscle power.
Resumo
Introdução: Estudos que avaliam a
reprodutibilidade dos testes de CVIM e potência muscular são escassos e, muitas
vezes, com baixa aplicabilidade prática. Objetivo: Avaliar a confiabilidade e a
reprodutibilidade de testes para a medida de diferentes manifestações da força
muscular. Métodos: Foram avaliados 19 homens saudáveis, com 23,36 ± 2,35
anos, com 1,82 ± 0,06 m e 80,17 ± 11,57 kg, sem experiência com treinamento de
resistido (TR) e sem vivência com os protocolos dos testes realizados. Os
voluntários foram submetidos a duas avaliações de força máxima isométrica
(CVIM), força máxima dinâmica (1RM), e potência muscular, respectivamente,
separadas por 72h. Resultados: Para todos os protocolos de avaliação da
força muscular foi encontrado um coeficiente de correlação intraclasse (CCI)
com força de concordância alta a muito alta (CCI ≥ 0,79). No entanto,
todas as medidas apresentaram coeficiente de variação (CV) moderados: CVIM (CV
= 12,0%), potência muscular média a 40%, 60% e a 80% da 1RM (CV = 16,2%, 11,0%
e 14,0% respectivamente) e potência muscular pico (PP) a 60% e a 80% da 1RM (CV
= 11,8% e 13,3% respectivamente), à exceção da RM (CV = 6,4%), e da PP a 40% de
1RM (CV = 5,8%), com um erro padrão de medida (EPM) aceitável. Conclusão:
Os valores altos a muito altos para o CCI indicam uma excelente confiabilidade
das medidas nas diferentes manifestações de força muscular, no entanto, visto
que os voluntários não tinham experiência com TR, recomenda-se um processo de
familiarização prévio à realização dos testes, no sentido de melhorar os
indicadores de reprodutibilidade dos mesmos.
Palavras-chave: saúde; força muscular; potência
muscular.
Introduction
Strength training has been recommended for the
improvement of musculoskeletal fitness, its use involves the application of
high loads to provide greater adaptations such as increased strength and muscle
mass [1,2,3]. In summary, we mention one of the principles of Strength Training,
the principle of overload. In this perspective, monitoring the evolution of
loads used in a strength-training program is necessary to identify changes
induced by this modality.
Some strength tests have been used to monitor training
loads. The maximal repetition test (1RM) is one of the most used methods for
evaluating the maximum load in isoinercial movements
in scientific research. According to the literature, the 1RM test is considered
the gold standard in the evaluation of load-displacement through dynamic force,
since it is a practical method, has a low operational cost, and with a large
margin of safety for its applicability [4,5] provided that the test protocol is
correctly conducted. However, its use requires some methodological care, among
which pre-test familiarization has been one of the most studied. It is also
evidenced in the literature that the lack of familiarization with the 1-RM test
procedures may compromise the results obtained [6].
In addition, muscle strength can manifest itself in
different ways: maximum, power and resistance, and these components can be
expressed dynamically or isometrically [7,8]. To evaluate these different
manifestations of strength, different tests can be used, such as 1RM tests,
maximum voluntary isometric contraction (MVIC), and isokinetic evaluations,
among others [9].
However, the literature focuses on studies on the
reproducibility of the 1RM test [10,11,12], and studies that evaluated the
reproducibility of MVIC or muscle power tests are scarce and often with low
practical applicability. Thus, the evaluation of the reproducibility of
protocols that evaluate different manifestations of muscle strength can add
information to the scientific literature, especially on neglected tests, such
as MVIC and muscle power, as well as provide practical information for the
evaluation and monitoring of the different manifestations of muscle strength
for professionals involved in the prescription of physical
training/rehabilitation programs.
Because of lack of the literature cited above, the
present study aims to evaluate the reliability and reproducibility of tests to
measure different manifestations of muscle strength, more specifically, MVIC,
1RM and muscle power.
Methods
This work deals with the development of an
experimental and prospective study, which comprised two phases and was carried
out, in its entirety, in the Morphophysiology
Laboratory of the Physical Education course of the Federal University of Viçosa Campus UFV-Florestal.
Before any experiment, the present work was approved
by the Ethics Committee for Research in Human Beings of UFV (CAAE:
93793118.1.0000.5153; Opinion number: 2,919,591). In addition, all the
procedures used here are by the Ethical Standards for Research in Exercise and
Sports Sciences and carried out by the Declaration of Helsinki [13].
Participants
The study population consisted of university students
aged between 19 and 28 years, male, and living in the city of Florestal/MG.
The inclusion criteria adopted were: being between 18
and 28 years old; being clinically able to perform the tests; not presenting
any acute or chronic disease that may be affected by the performance of the
tests; and consenting freely and voluntarily to perform all the procedures of
the study.
Exclusion criteria were: to present any bone or joint
limitation that prevents the tests; and be a user of hormonal or
anti-inflammatory drugs, which may affect the outcome of the evaluations.
Volunteers who met the inclusion criteria and did not
present any exclusion criteria were admitted to the study.
Considering a minimum effect size of 0.68 for muscle
strength (15), a probability of α error of 0.05, and a power of (1 - β
error) of 0.95, the total study sample should have at least 16 people,
according to the G*Power program of the University of Düsseldorf.
Protocols and procedures
To verify the reproducibility of the measurement tests
of the different manifestations of muscle strength, the MVIC, 1RM, and muscle
power tests were performed.
In the evaluation of the MVIC of the lower limbs, a
load cell or extensiometric cell (MK, model
CSL/ZL-1T, MK Controle, Brazil) with a sampling
frequency of 1000 Hz was used. Before the test was carried out, the device was
adjusted so that the knees of the evaluated patients were at a 90° bending
angle, measured with a goniometer (Carci, São Paulo,
Brazil). At the evaluator's command, the evaluated performed a maximum
isometric tension of the femoral quadriceps for 5 seconds, without letting the
gluteal region lose the count with the seat so that there was no change in
angulation and mechanical advantage in the lever created between the resistant
force, powerful force and support point. During the execution, verbal stimuli
were given to induce a higher tension, as well as the permanence of their
maximum levels throughout the test. Two attempts were made, separated by an
interval of 2 minutes between them, considered the highest value obtained in
the two attempts [14,15].
To perform the 1RM test, the knee extension exercise
was used in a BH fitness Nevada Pro-t extensor machine. The initial position
adopted was similar to the MVIC test, with the individual seated with his back
resting on the back of the device, his hands holding the lateral support, and
the knees in 90° flexion. To perform the test, the volunteer was asked to
extend the knee until it formed an angle of approximately 180° (final position)
and to return to the initial position. Before the determination of 1RM, the
evaluated performed the previous warm-up, which consisted of four repetitions
with a load of 50% of the maximum voluntary contraction value. At the end of
the warm-up, the volunteer evaluated his perception of effort, using the
OMNI-RES scale from 0 to 10 [16]. The load was increased at the discretion of
the evaluator, according to the ease of execution and the perception of effort
of the evaluated, the volunteer was asked to perform two repetitions with the
new load. The load was increased until the evaluated could perform only one
repetition. A maximum of five attempts could be made to determine the 1RM, with
a rest interval of 2 minutes between each attempt [14,15].
The evaluation of lower limbs power was achieved
through the same knee extension machine used in the MVIC and 1RM tests,
starting from the same initial position (90º of kneeling flexion) and reaching
the same final position (180º knee extension) of the 1RM test. Three different
loads were used to evaluate the power, obtained from percentage values of 1RM
(40%, 60%, and 80% of 1RM), in which the evaluated performed the knee extension
movement (concentric phase of movement) at the highest possible speed. The
return of the knees to the initial position occurred in a controlled manner,
with a micropause of 1 to 2 seconds, to prevent the effect of accumulated
elastic force from interfering in the next execution. The loads of this test
were randomized in each volunteer to control a possible bias related to the
learning effect or the cumulative action of fatigue. In each load, three
repetitions were performed with a 2-minute rest interval between loads [15]. A
linear position transducer or Chronojump Encoder (Chronojump BoscoSystem,
Barcelona, Spain) was used, with a sampling frequency of 1000 Hertz, and the Chronojump Software, version 1.6.2, (Chronojump
BoscoSystem, Barcelona, Spain), to determine the
power values. Through this instrument, it was possible to obtain information
about average power (AP) and peak power (PP).
The experimental design adopted in this study allowed
the evaluation of the reliability of the reproducibility of the tests to
measure the different manifestations of muscle strength. For this, all the
evaluated patients underwent two evaluations, separated by 72h, in which they
performed the same procedures. From these evaluations, data regarding 1RM,
MVIC, AP, and PP of each participant were analyzed. These outcome parameters
were used to calculate the coefficient of variation (CV), the intraclass
correlation coefficient (ICC), and its 95% confidence interval (CI 95%).
Statistical treatment
All statistical analyses were performed in the
statistical program SPSS for Windows, version 23 (IBM, Chicago, USA).
Initially, the data were submitted to the Shapiro-Wilk test to verify normality
and, later, generated means and standard deviations (SD) for descriptive
analysis of the data. The reliability of the measurement tests of the different
manifestations of muscle strength will be determined by the calculation of CV
and ICC. The ICC was also used to verify the reproducibility of muscle strength
measurements, with confidence interval of 95% (CI 95%). ICC values equal to or
greater than 0.90 can be considered very high, values between 0.70 and 0.89,
can be considered high and values between 0.50 and 0.69, are moderate [17,18].
The values for the standard error of the measurement (SEM) were also calculated
by the product of the basal standard deviation with the square root of (1-r),
in which r is the intraclass correlation (SEM = SD x √1-ICC). In
addition, the minimally detectable change (MDC) by the SEM product was
calculated with the square root of two (due to the variance of the measurement
error of each instrument) and with the value of 1.96, which represents that of
a normal standard curve associated with a 95% confidence interval (MDC = 1.96 x
√2 x SEM) [18,19]. A statistical significance level of p < 0.05 was
established for all treatments.
Results
The present study participated in 19 male volunteers,
with no previous experience with strength training or who did not train for at
least six months, with a mean age of 23.36 ± 2.35 years, mean height of 1.82 ±
0.06 m, and mean body mass of 80.17 ± 11.57 kg. During the tests, there were no
reports of osteomyoarticular or metabolic problems
related to their performance.
Data on the reliability and reproducibility of test
protocols to measure the different manifestations of muscle strength can be
observed in Table I. It is possible to observe, from the values found, that for
all protocols for evaluating the different manifestations of muscle strength, a
high to very high ICC was found (≥ 0.79). However, all measures presented
moderate CV (except for 1RM and PP at 40% of 1RM), with an acceptable SEM.
Table I - Results for reliability and reproducibility of
measurements obtained in test protocols for different manifestations of muscle
strength
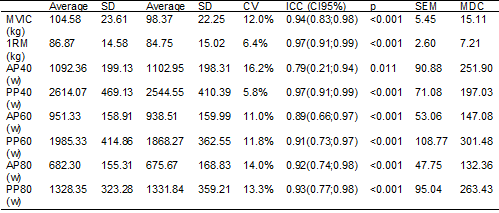
SD = standard deviation; CV = coefficient of
variation; ICC = intraclass correlation coefficient; 95% CI = 95% confidence
interval; SEM = measurement standard error; MDC= minimally detectable change; MVIC
= maximal isometric strength; 1RM = maximal dynamic strength; AP40 = muscle
power average at 40% of 1RM; PP40 = peak of muscle power at 40% of 1RM; AP60 =
muscle power average at 60% of 1RM; PP60 = peak of muscle power at 60% of 1RM;
AP80 = muscle power average at 80% of 1RM; PP80 = peak of muscle power at 80%
of 1RM
Discussion
The present study aimed to evaluate the reliability
and reproducibility of tests to measure different manifestations of muscle
strength. As main results were found high to very high values for the ICC that
indicate excellent reliability of the measurements in the different
manifestations of muscle strength; in individuals without experience with
strength training and without familiarization with the tests, considerable variability
was found for all measurements, except for 1RM and PP at 40% of 1RM; and the
tests showed good measurement accuracy for MVIC, 1RM, and PP, due to the low
SEM values found.
Although the CV value found was moderate for the
results of MVIC (12%), the ICC found for the MVIC test (0.94) is in line with
the results obtained by Neves et al. [20] who evaluated 30 volunteer
students (of both sexes and age between 18 and 25 years) in the knee extension
exercise in the flexo-extensor chair. For the collection
of the results, a load cell of 250 kg positioned in the flexor chair and
connected to the Software Miotool USB 400 was used,
which translated the values to the computer. At the applicator command, the
evaluated person was instructed to perform maximum voluntary isometric force
and verbally stimulated to maintain the maximum levels for 6 seconds. At the
end of the time, he was instructed to relax and rest for 1 minute, until the
next attempt, six attempts were made for each lower limb, three attempts commanded
by an evaluator and three commanded by another evaluator. The protocol was
repeated after 48h. The analysis of the values was performed by Cronbach's
alpha and the results showed a strong correlation on the first day (α =
0.980) on the second day they found values similar to the first (α =
0.982), this means that the test had an excellent reliability index.
Although there are differences between the protocol
used by Neves et al. [20] and the protocol we used in this study, both
provided relevant data for the literature, with a high degree of reliability
and reproducibility. We emphasize that for better and more reliable results it
is recommended to familiarize with the test and with the movement that will be
performed, according to Brown and Weir [9] and more the strength test has
generally shown to be reliable, novice individuals are likely to improve their
scores in subsequent tests simply due to familiarization and comfort during the
test.
Verdik et
al. [21] prove the reproducibility of the 1RM test as a valid measure of
knee extensor strength, regardless of physical conditioning and age of the
subject. Although the 1RM test is low operational cost and easy to
reproducibility, according to Dias et al. [22] some points should be
taken into consideration before its execution, such as: starting the test
rested and effortlessly strenuous for at least 24 hours prior to the test; have
knowledge of the movement that will be performed and if you have not had an
experience that goes through a learning session; be motivated to achieve your
best performance and consequently its best result; perform previous heating;
not let 1RM attempts pass 5; and that there is a recovery interval between
attempts so that there is no energy impairment in subsequent ones. Given the
low CV value found in the 1RM test results (6.4%), it is possible to consider
that, from the results found, it has good applicability, reliability, and
reproducibility.
The CV and ICC values found for PP at 40% appear to be
similar to those found by Pagaduan and Blas [23] who
tested 15 college students from the following protocol: perform a jump as high
as possible against a contact platform and with a 20 kg bar placed on the
shoulders, in order to verify the reliability of a movement jump loaded using
the Chronojump-BoscoSystem and thus establish the
reproducibility of the test to aggregate the literature related to
lower-lower-heed potency. The results were obtained from the Chronojump-BoscoSystem Software and the statistical analysis
they found the ICC considered moderate to high (0.86) and a low value for CV
(6.7%), which fits into a reliable test according to the software used. We
emphasize that studies evaluating the reproducibility of power tests are scarce
and make it difficult to directly compare the results obtained in our study
with those obtained in other studies. Although it is not the same protocol and
the same test used in our study, we evidenced the high potential that these
tests have to aggregate the literature to measure the different types of
strength already mentioned.
The values found for CV in the 1RM test and the PP
test at 40% of 1RM are considered low, 6.4%, and 5.8%, respectively, presenting
excellent reproducibility. On the other hand, the other protocols presented
values between 11% and 16%, and moderate reproducibility was considered.
According to Atkinson and Nevill [24], absolute
reproducibility has been considered acceptable when the value found is below
10%. However, it is worth noting that this change in the coefficient of
variation can be explained by some points such as lack of familiarization with
the test, fatigue, and the load used in the two days of testing.
Determining SEM measures is crucial in order to be
able to compare the measures between the evaluations. To measure and evaluate
the reliability of both protocols we used SEM and MDC in all values, and from
the results, we can say that the tests performed presented excellent
reliability measures and good results for the reproducibility of the tests of
the different manifestations of muscle strength.
Conclusion
Because of the high to very high values for the ICC,
it can be concluded that the present study demonstrates that, even in
beginners, muscle strength assessment tests present excellent reliability of
measurements in the different manifestations of muscle strength. However, a CV
was found with considerable variability, indicating that, because they are
volunteers without previous experience with RT, a familiarization process prior
to the tests is recommended, in order to improve their reproducibility
indicators.
Conflict of interest
The authors declare that there are no conflicts of
interest.
Financing
Funded by the FAPEMIG (Research Support Foundation of
Minas Gerais State).
Authors' contributions
Conception and design of the research: Martins DBM, Moreira OC; Obtaining data: Martins DBM, Moreira
OC, Santiago IA; Analysis and interpretation of data: Martins DBM,
Moreira OC. Statistical analysis: Martins DBM, Moreira OC; Writing of
the manuscript: Moreira OC, Martins DBM, Santiago AI, Oliveira CEP; Critical
revision of the manuscript regarding intellectual content important:
Oliveira CEP, Silva SF
References
- American College of Sports Medicine. Appropriate physical activity
intervention strategies for weight loss and prevention of weight regain for
adults. Med Sci Sports Exerc. 2009;41(2):459-71. doi: 10.1249/mss.0b013e3181949333 [Crossref]
- American College of Sports Medicine. Quantity and quality of exercise for developing and maintaining cardiorespiratory, musculoskeletal, and neuromotor fitness in apparently healthy adults: guidance for prescribing exercise. Med Sci Sports Exerc. 2011;43(7):1334-59. doi: 10.1249/mss.0b013e318213fefb [Crossref]
- Santos LV, Pereira ET, Reguera-García MM, Oliveira CEP, Moreira OC. Resistance
training and muscle strength in people with spinal cord injury: a systematic
review and meta-analysis. J Bodyw Mov Ther. 2022;29:154-60. doi: 10.1016/j.jbmt.2021.09.031 [Crossref]
- Rhea MR, Alvar BA, Burkett LN, Ball SD. A meta-analysis to determine the dose response for strength development. Med Sci Sports Exerc. 2003;35(3):456-64. doi: 10.1249/01.MSS.0000053727.63505.D4 [Crossref]
- Mayhew JL, Johnson BD, Lamonte MJ, Lauber D, Kemmler W. Accuracy of prediction equations for determining one repetition maximum bench press in women before and after resistance training. J Strength Cond Res. 2008;22(5):1570-7. doi: 10.1519/JSC.0b013e31817b02ad [Crossref]
- Rydwik E, Karlsson C, Frändin K, Akner G. Muscle strength testing with one repetition maximum in the arm/shoulder for people aged 75 + - test-retest reliability. Clin Rehabil. 2007;21(3):258-65. doi: 10.1177/0269215506072088 [Crossref]
- Knuttgen HG. Measurement and terminology for authors and reviewers. J Sports Med Phys Fitness. 2019;59(2):341-2. doi: 10.23736/S0022-4707.18.09363-5 [Crossref]
- Moreira OC, Oliveira CEP, Maroto-Izquierdo S, Cuevas MJ, Paz JA. Effects of short-term strength training on body composition, muscle strength and functional capacity of elderly: a systematic review and meta-analysis. Biosci J. 2019;35(6):1941-57. doi: 10.14393/BJ-v35n6a2019-42775 [Crossref]
- Brown LE, Weir JP. Asep procedures
recommendation I: accurate assesment of muscular
strength and power. JEPonline. 2001;4(3):1-21.
- Dias RMT, Cucato GG, Camara LC, Wolosker N. Reprodutibilidade do teste de 1-RM em indivíduos com doença arterial obstrutiva periférica. Rev Bras Med Esporte. 2010;16(3):201-4. doi: 10.1590/s1517-86922010000300009 [Crossref]
- Mitter B, Csapo
R, Bauer P, Tschan H. Reproducibility of strength performance
and strength-endurance profiles: A test-retest study. PLoS
One. 2022;17(5):e0268074. doi: 10.1371/journal.pone.0268074 [Crossref]
- Schoenell MCW, Tiggemann CL, Cadore EL, Tartaruga MP, Kruel LFM. Correlação e reprodutibilidade de testes abdominais em mulheres jovens. Rev Bras Ciênc Esporte. 2013;35(3):561-574. doi: 10.1590/s0101-32892013000300003 [Crossref]
- Williams JR. The Declaration of Helsinki and public health. Bull World
Health Organ. 2008;86(8):650-2. doi: 10.2471/blt.08.050955 [Crossref]
- Oliveira CEP, Moreira OC, Carrión-Yagual ZM, Medina-Pérez C, Paz JA. Effects of classic progressive resistance training versus eccentric-enhanced resistance training in people with multiple sclerosis. Arch Phys Med Rehabil. 2018;99(5):819-25. doi: 10.1016/j.apmr.2017.10.021 [Crossref]
- Moreira OC, Cardozo RMB, Vicente MA, Matos DG, Mazini Filho ML, Guimarães MP, et al. Acute effect of stretching prior to resistance training on morphological, functional and activation indicators of skeletal muscle in young men. Sport Sci Health. 2022:18:193-202. doi: 10.1007/s11332-021-00793-0 [Crossref]
- Robertson RJ, Goss FL, Rutkowski J, Lenz B, Dixon C, Timmer J, et al. Concurrent validation of the OMNI perceived exertion scale for resistance exercise. Med Sci Sports Exerc. 2003;35(2):333-41. doi: 10.1249/01.MSS.0000048831.15016.2A [Crossref]
- Bosquet L, Maquet D, Forthomme B, Nowak N, Lehance C, Croisier JL. Effect
of the lengthening of the protocol on the reliability of muscle fatigue
indicators. Int J Sports Med. 2010;31(2):82-8. Epub
2009 Dec 17. doi: 10.1055/s-0029-1243168 [Crossref]
- Mentiplay BF, Perraton LG, Bower KJ, Adair B, Pua YH, Williams GP, et al. Assessment of lower limb muscle strength and power using hand-held and fixed dynamometry: a reliability and validity study. PLoS One. 2015;10(10):e0140822. doi: 10.1371/journal.pone.0140822 [Crossref]
- Beckerman H, Roebroeck ME, Lankhorst GJ, Becher JG, Bezemer PD, Verbeek AL. Smallest real difference, a link between reproducibility and responsiveness. Qual Life Res. 2001;10(7):571-8. doi: 10.1023/a:1013138911638 [Crossref]
- Neves CDC, Tossige-Gomes R, Avelar NCP, Simão AP, Lacerda ACR.
Avaliação da confiabilidade da força isométrica de extensores de joelho pelo
uso da célula de carga. Ter Man. 2011;9(41):16-21.
- Verdijk LB, van Loon L, Meijer K, Savelberg HH. One-repetition maximum strength test represents a valid means to assess leg strength in vivo in humans. J Sports Sci. 2009;27(1):59-68. doi: 10.1080/02640410802428089 [Crossref]
- Dias RMR, Avelar A, Menêses LA, Salvador PEM, Da Silva PRD, Cyrino ED. Segurança, reprodutibilidade, fatores intervenientes e aplicabilidade de testes de 1-RM. Motriz. 2013;19(1):231-42. doi: 10.1590/S1980-65742013000100024 [Crossref]
- Pagaduan CJ, Blas X.
Reliability of a loaded countermovement jump performance using the chronojump-boscosystem. Kinesiologia
Slovenica. 2012;18(2):45-8.
- Atkinson G, Nevill AM. Statistical methods for assessing measurement error (reliability) in variables relevant to sports medicine. Sports Med. 1998;26(4):217-38. doi: 10.2165/00007256-199826040-00002 [Crossref]
