Rev Bras Fisiol Exerc. 2023;22:e225443
doi: 10.33233/rbfex.v22i1.5443
REVIEW
Biochemical markers related to performance in women athletes
Marcadores
bioquímicos relacionados à performance em mulheres atletas
Antônio Carlos
Leal Cortez1,2, Alexandrino Barbosa de Sousa Neto1, Antônio
Carlos Gomes3
1Centro Universitário Santo Agostinho (UNIFSA),
Teresina, PI, Brazil
2
Universidade
Federal do Estado do Rio de Janeiro
(UNIRIO), RJ, Brazil
3Centro Universitário Tereza D’ávila (UNIFATEA),
Lorena, SP, Brazil
Received: May 9, 2023; Accepted: June 22, 2023.
Correspondence: Antônio Carlos
Leal Cortez: antoniocarloscortez@hotmail.com
How to cite
Cortez ACL, Sousa Neto
AB, Gomes AC. Biochemical markers related to performance in women athletes. Rev Bras Fisiol Exerc. 2023;22:e225443. doi: 10.33233/rbfex.v22i1.5443
Abstract
Introduction: It is notorious
that there are differences in relation to the biological composition between men
and women, especially when we refer to physical performance, in which the morphological,
physiological and biochemical characteristics are observed distinct between the
sexes, even more, when it comes to the use of markers biochemicals related to the
performance of female athletes. Objective: To elucidate the main biochemical
markers that are related to performance in female athletes. Methods: The
reflective theoretical path presented in this theoretical essay on health, outlined
here on biochemical markers related to female performance, is based on a scientific
literature review, as well as on national and international documents that addressed
the issue in question. Results: The scientific evidence presented in the
selected studies allowed us to present data regarding the anatomical-physiological
effects of training on female athletes and on the main biochemical markers: Creatinokinase, C-Reactive Protein, Lactate Dehydrogenase, Erythrocytes,
Hematocrits, Hemoglobin, Testosterone, Estrogen, Progesterone, which suffer direct
action according to the volume x training intensity, as well as the athlete's menstrual
cycle. Conclusion: The scientific evidence presented during the study elucidated
the main anatomo-physiological and biochemical differences
between men and women and how they directly interfere, from the training process
to performance, with no consensus on physiological parameters and specific biochemical
markers for female athletes.
Keywords: female athlete; biomarkers; athletic
performance.
Resumo
Introdução: É notório que existem diferenças em relação
à composição biológica entre homens e mulheres, principalmente quando nos referimos
ao desempenho físico, no qual são observadas as características morfológicas, fisiológicas
e bioquímicas distintas entre os sexos, ainda mais, quando se trata da utilização
dos marcadores bioquímicos relacionados à performance das mulheres atletas. Objetivo:
Elucidar os principais marcadores bioquímicos que estão relacionados à performance
em mulheres atletas. Métodos: O percurso teórico reflexivo apresentado neste
ensaio teórico em saúde, aqui delineado sobre os marcadores bioquímicos relacionados
à performance feminina, pauta-se em revisão de literatura científica, bem como em
documentos nacionais e internacionais que abordaram a temática em questão. Resultados:
As evidências científicas apresentadas nos estudos selecionados nos permitiram apresentar
dados referentes aos efeitos anátomo-fisiológicos do treinamento em mulheres atletas
e sobre os principais marcadores bioquímicos: Creatinoquinase,
Proteína C-Reativa, Lactato Desidrogenase, Eritrócitos,
Hematócritos, Hemoglobina, Testosterona, Estrógeno, Progesterona, que sofrem ação
direta de acordo com o volume x intensidade de treinamento, bem como com o ciclo
menstrual da atleta. Conclusão: As evidências científicas apresentadas no
decorrer do estudo elucidaram as principais diferenças anátomo-fisiológicas e bioquímicas
entre homens e mulheres e como elas interferem diretamente, desde o processo de
treinamento até a performance, não havendo consenso sobre parâmetros fisiológicos
e de marcadores bioquímicos específicos para mulheres atletas.
Palavras-chave: mulher atleta; biomarcadores; desempenho
atlético.
Introduction
From the moment that international sports
bodies allowed the participation of female athletes in official sports competitions
such as the 1924 Olympic Games in Paris/France, women began to participate more
actively within the world sports scene in different sports. During all these years
until today, women have been occupying more and more space in sports, even taking
into account their anatomy and physiology and how their bodies and their biochemical
reactions are expressed in the face of adaptations resulting from sports training
[1].
It is clear that there are differences
in relation to the biological composition between men and women, especially when
we refer to physical performance, in which the physiological and morphological characteristics
of men and women are observed. The different neuromuscular and metabolic responses
between men and women reflect the action of characteristic hormones: testosterone
for men and estrogen for women [2]. The action of these two substances directly
influence cellular composition, with testosterone being directly linked to protein
deposition in muscles, bones, skin and other parts of the body. Estrogen, on the
other hand, is linked to increased fat deposition in the breasts, hips and subcutaneous
tissue, which explains the greater amount of fat in females [3].
According to Fortes et al. [4],
women have lower lean body mass, fewer sweat glands, a smaller heart, lower blood
volume and lower concentrations of hemoglobin and hematocrit, which are factors
that influence physical performance. Regarding lung function, there are also marked
differences between the sexes, with men having a larger airway diameter, greater
lung volumes and diffusion surfaces compared to adult women, which confers greater
efficiency in performing the exercise. These sex differences in lung diffusing capacity
are linked to the lower total number of alveoli (lower surface area) and smaller
relative diameter of the airways in women [5].
It is important to emphasize that the
physical and physiological adaptations are caused by physical training, within aspects
of the principles of sports training, in this case the organism adapts to the stimuli,
changing some parameters (physical, physiological, biochemical and biomechanical)
such as muscle hypertrophy, gain lean mass, increased power (mainly aerobic), increased
bone mineral density, increased number and size of mitochondria, increased glycogen
storage, increased myofibrils, increased actin-myosin filaments, sarcoplasmic content,
etc. [6].
The intensity and volume of training
sessions, as well as the recovery time between sessions, have been a major concern
for coaches, physiologists and sports scientists, as they are intervening factors
in performance-oriented sports training, and there is a fine line among them. There
are positive and negative consequences related to the stress of the training load,
mainly for athletes who are always at the physical limits of their bodies. Therefore,
we can describe these factors as overreaching and overtraining, which is the process
that presents a drop in the physical performance of an athlete. The recovery from
overreaching can take up to two weeks and the recovery from overtraining can go
from two weeks and take months [7,8].
Overtraining is caused by an imbalance
between training stress and recovery. Athletes experience mental fatigue and a drop-in
performance. Overtraining has a great impact on the physiological and biochemical
systems. We can mention as a consequence of this imbalance, in the physiological
and biochemical systems, the decrease in muscle strength, coordination, increased
perception of effort and recovery, changes in the lactate profile, sleep, anorexia,
decrease also in muscle glycogen, bone mineral content, testosterone and testosterone/cortisol
ratio above 30%, as well as increase in cortisol and urea [1,9,10,11].
Biochemical markers can be considered
valid parameters to assess the occurrence of overtraining. This syndrome is accompanied
by a marked response to oxidative stress biomarkers that are altered during high-intensity
training and return to normal levels when the load is reduced, suggesting a dose-response
relationship. Several direct and indirect methods have been used to analyze muscle
damage from physical exercise. Indirect methods such as myoglobin, lactate dehydrogenase
(LDH), myosin heavy chain fragment and CK are most commonly used [12].
These molecules can be used as markers
of damage in skeletal muscle tissue due to the fact that they are cytoplasmic and
thus impermeable in the plasmatic membrane. Thus, the increase in the levels of
these molecules in the extracellular fluid may indicate a change in the permeability
of the membrane or its disruption, thus causing loss of performance [13]. Thus,
the study intends, through a theoretical essay in health, to describe the main biochemical
markers that are related to performance in female athletes.
Methods
Methodological design
The study in question is a theoretical
health essay, with a qualitative approach, aiming to bring a discussion, a new look
and insights on issues of current interest [14].
Ethical care
The study was conducted in accordance
with the Committee on Publication Ethics (COPE) guidelines, which contain information
for authors and editors on research ethics [15].
Formulation of the research question
To guide the retrieval of information,
the research question was structured aiming to guarantee not only the internal validity,
but also the power of extrapolation of the results of the theoretical test. The
scientific evidence of safety and efficacy is applicable among populations in different
regions of the world and by the selection of studies in a comprehensive and exhaustive
way, through the adoption of criteria and evaluation of the quality and validity
of the studies retrieved in the searches [16]. Thus, the aforementioned study has
as its guiding question: What are the main biochemical markers that are related
to performance in female athletes?
Definition of eligibility criteria
Inclusion and exclusion criteria for
document selection are detailed in Chart 1.
Chart 1 - Description of inclusion and exclusion
criteria for selection of studies
Source: authors 2023.
Selection of studies
The terms and interterms were defined
from consultations, by the changed index, in DeCS, from
which the descriptors in Portuguese and their respective MeSH
were extracted, submitted to subsequent research to identify their interterms, in
the databases Pubmed, Scielo,
Web of Science and Scopus. The search for the definition of these terms and interterms
was carried out in January 2023.
Strategies were listed to guide the
identification and screening of studies. First, it was decided that the research
period would be free to cover the largest volume of information. Second, the electronic
search was carried out in the following databases: Pubmed,
Scielo, Web of Science and Scopus. This choice was made
to ensure greater coverage of peer-reviewed articles and to include a variety of
journals with higher impact factors [17].
The keywords and Boolean operators chosen
were “woman athlete”, “biochemical markers”, “performance”, using the Boolean operators
AND/OR, as well as their synonyms, having as search scope the respective terms in
the title, abstract and words of articles published in journals. This choice is
due to a previous evaluation in the literature, in which the correlation between
them and the frequency with which they are used in studies was verified.
Results and discussion
Therefore, the results presented by
the theoretical essay in question propose a discussion based on scientific evidence,
aiming to elucidate the anatomical-physiological effects of training and the main
biochemical parameters for female athletes and, in this way, serve as a basis for
future research on the subject, since there are still clinical gaps about the main
biochemical markers that are related to performance in female athletes.
Thus, we chose to section the discussion
of the theoretical essay addressing the following themes: anatomical-physiological
effects of training in female athletes and biochemical markers in female athletes.
Anatomical-physiological effects of training in women athletes
In relation to structural and anatomical
differences, women are 10 to 15 centimeters smaller than men, on average, and 10
to 20 kg lighter. The woman has a smaller muscle mass and, consequently, has a lower
maximum strength, with lower tissue density, ligaments and muscles, which are more
elastic and flexible [18].
According to cardiovascular dimensions,
women have a smaller heart, lower blood volume and lower hemoglobin concentrations.
Because her heart is smaller, end-diastolic volume, stroke volume, and cardiac output
are smaller. Regarding the respiratory system, women have smaller nasal cavities,
trachea, bronchi and lungs than men and smaller capillary volumes, resulting in
lower pulmonary ventilation [19].
During aerobic exercises, a lower maximum
oxygen consumption is observed in women compared to men, and the main hemodynamic
mechanism involved is the lower cardiac output due to the lower systolic volume,
a characteristic that, in turn, is consequent to the lower mass and volume ventricles
in women, in addition, the oxygen-carrying capacity (due to a lower mean hemoglobin
level resulting from menses) is lower in women [20].
Batlouni et
al. [21] highlighted that during the transition from rest to exercise, systolic
volume decreases more in women than in men, which explains why cardiac output, which
is a product of systolic volume by heart rate, is directly related to Maximum VO2,
therefore, the maximum consumption of oxygen is lower in females. Although adaptability
to training is similar, these factors combine to cause women's athletic performance
to be 6% to 15% lower than men.
Regarding flexibility, women's ligaments
and muscles are more elastic and flexible, and through strength training, women's
strength can be increased by about 20% to 40%. Because of estrogen's antioxidant
effects, women have less muscle mass and less testosterone, which is very important
in muscle hypertrophy, so there is less cell damage, but in terms of muscle fiber
composition, they are similar and in women, the volume of each fiber, type I or
type II, is greater than in men. These characteristics give men greater strength
and muscular endurance than women [22].
Testosterone is considered a hormone
that is related to the synthesis and reduction of muscle protein degradation. It
is a predominantly male hormone, with anabolic and androgenic function, produced
by Leydig cells in the testicles and also a small amount is secreted by the adrenal
glands [23]. In women, the ovaries and adrenal glands are responsible for producing
testosterone. Testosterone is more produced and released by males, which does justice
to its function, greater muscle mass and characteristics such as more hair, deeper
voice, sperm production, etc. Testosterone is also present in the female system
in smaller amounts, and is dependent on glucocorticoid biosynthesis, in which the
adrenal cortex secretes androgenic steroids that can be converted to testosterone
[24].
The menstrual cycle influences a woman's
performance. In the luteal phase, fat oxidation is greater and in the follicular
phase, carbohydrate oxidation is greater. Catecholamines have more significant responses
in the follicular phase [25]. Women use more fat as a source of substrate, therefore,
blood glucose during exercise is higher than that of men, and carbohydrate consumption
is lower in women [19].
The GH, also known as growth hormone
or somatotropin, is the most abundant hormone secreted by the anterior pituitary,
and there are two main genes involved in growth hormone synthesis: the normal GH
gene expressed in the pituitary and the variant GH gene (GH-V or GH-2) expressed
in the placenta, detectable in the circulation only during pregnancy or lactation,
essential for a series of metabolic processes and growth of various tissues, including
muscle [26,27].
During human development, GH secretion
in both sexes reaches maximum concentrations during growth periods, mainly in adolescence,
soon after that, both the frequency and the intensity of secretion are reduced,
as for example an individual with about 20 years who secrete more than twice the
amount of GH per day as older people. It should be noted that several factors can
influence GH secretion, including nutritional status, amount of sleep and body fat,
stress and physical activity or training level, etc. [28,29,30,31].
When we analyze the mechanism of action
of GH in our body, we can describe it as an anabolic effect related to stimulating
tissue growth and metabolism, altering the flow, oxidation and metabolism of almost
all nutrients in circulation, which can be divided into direct and indirect effects.
The direct effects are mediated by intracellular signaling cascades triggered by
the binding of GH to its receptors on the plasmatic membrane, and the indirect effects
are mediated mainly by the regulation of the synthesis of growth stimulated by physical
exercise [27].
Many of the effects promoted by physical
activity are affected by GH, including the reduction of protein catabolism and glucose
oxidation, while increasing the mobilization of more free fatty acids (FFAs) in
adipose tissue for energy production. These facts suggest that GH is an important
hormone released in several stressful situations, however, studies have shown that
GH also has anabolic effects, including promoting positive protein balance and increasing
mass and IGF-1 release, involved in stimulating the muscular hypertrophy process
[28,32,33].
Biochemical markers in women athletes
Biochemical markers can be considered
significant parameters in evaluating the occurrence of overtraining. This syndrome
is accompanied by a significant response of biomarkers of oxidative stress, which
are altered during periods of intense training and return to normal levels when
the load decreases, indicating a dose-response relationship, that is, volume x intensity
of training. Many direct and indirect methods have been used in the analysis of
muscle damage resulting from physical exercise [12,35].
Indirect methods such as myoglobin,
lactate dehydrogenase (LDH), myosin heavy chain fragment, and CK are most commonly
used. These molecules can be used as markers of skeletal muscle tissue injury because
they are cytoplasmic and therefore cannot penetrate the plasma membrane. Therefore,
increased levels of these molecules in the extracellular fluid may indicate changes
in membrane permeability or membrane rupture [13,36].
CK plays a key role in muscle cell energy
formation, as it is an enzyme within the muscle responsible for maintaining adequate
ATP levels during muscle contractions. It is known that the use of this marker to
control the training load and the diagnosis of overtraining is still under discussion,
and that changes in CK activity after exercise vary with different exercise conditions,
clinical evaluation of induced muscle damage the exercise is very difficult. But
CK can be a marker of fatigue and overload in non-athletes [11].
Prolonged and vigorous physical exercise
increases CK levels, and the magnitude of this increase is directly related to the
intensity and duration of the activity. It is believed that the effects of prolonged
continuous exercise can trigger mechanisms that induce CK extravasation into the
blood, where CK measurements seem to be sensitive and reliable parameters to assess
the increase in muscle stress or exercise tolerance in individuals. The total CK
value above 500 UI/L has been used as a parameter to indicate damage to the muscle
tissue [37,38].
In athletes, the study of CK at rest
and after exercise can be an important tool for technicians and physicians. Athletes
have higher levels of CK at rest when compared to untrained individuals, probably
due to greater muscle mass and daily synthesis, however, after exercise, serum CK
activity depends on the athlete's training level, although athletes have greater
muscle soreness when compared to untrained individuals, the peak serum activity
is lower [39].
Serum CK concentration peaks 1 to 4
days after exercise and remains elevated for several days. Thus, athletes who participate
in daily training have higher resting values than non-athletes, although this response
to training is attenuated by the so-called repeated attack effect, that is, the
repetition of an exercise after several days or even weeks causes less damage to
muscle fibers than that caused by the previous exercise [40].
For athletes, the reference interval
for CK is different for each gender, with the upper reference limit for men being
more than twice as high as for women; in addition, it is in agreement with the existence
of reference intervals for the Sex-specific CK in the general population. These
differences can be explained by the higher amount of CK in male muscle than in female
muscle, although other factors such as muscle membrane permeability, CK clearance
rate and lymphatic activity cannot be excluded [40,41].
According to Hecksteden
et al. [42], CK is an important marker related to muscle recovery and muscle
soreness, being essential in adjusting the daily physical training load. In this
case, we must take into account when evaluating this biochemical marker, the individual
differences of each athlete in relation to the group, performing individualized
reference intervals in order to optimize the monitoring of muscle recovery.
In addition to CK, we also have LDH
(lactate dehydrogenase), an enzyme present in cells that is responsible for glucose
metabolism in the body. This enzyme can be found in various organs and tissues,
so its elevation is not very specific and requires additional tests to make a diagnosis,
and usually, its elevation indicates organ or tissue damage. This is because, as
a result of cellular damage, intracellular LDH is released and circulates in the
blood, and its concentration is assessed by blood tests [43]. It is worth noting
that several factors influence the increase in CK and LDH after physical exercise,
such as age, sex, type of exercise performed, physical conditioning and the volume
x intensity of exercise performed [44,45].
Another important biochemical marker
in the process of assessing muscle wasting is C-reactive protein (CRP), which is
a protein synthesized by the liver. Its levels increase in response to inflammation,
so it is a reactive protein in the acute phase of training, having interleukin-6
(IL-6) as the main inducer, which influences the protein transcription process during
the acute phase of an inflammatory or infectious process. An important role played
by PCR is the recognition of pathogens or damaged cells [46].
In acute conditions of physical exercise,
CRP concentrations increase during the first 6 to 8 hours after inflammation or
tissue injury, and may reach up to thousands of times above the normal level in
approximately 48 hours. CRP is a clinical marker of great value due to its analytical
stability, in addition to showing reproducible results, high sensitivity and good
precision [47,48].
Together with the markers mentioned
above, we have the analysis of the red series, which include the quantification
of erythrocytes (RBCs), hematocrit, hemoglobin dosage and hematimetric
indices (VCM, HCM, CHCM, RDW), as well as the microscopic examination of the erythrocyte
morphology. These sets of analyzes provide subsidies for the diagnosis of the main
causes of anemia [49].
It is worth emphasizing that the biochemical
markers have differences in their classifications in view of sex, since there are
anatomical-physiological differences that cause the concentrations of these markers
to vary greatly, taking into account aspects such as the menstrual cycle and body
composition [50]. In chart 2, we present the main biochemical markers related to
the performance of female athletes.
Chart 2 - Main biochemical markers related
to the performance of female athletes
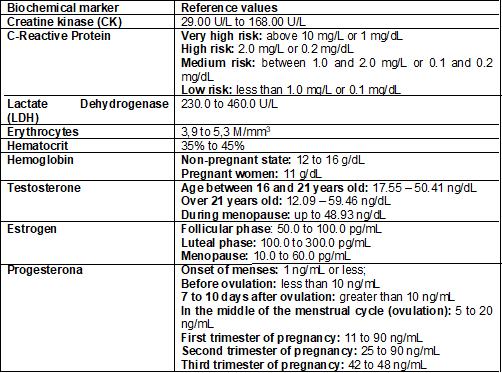
Source: Cortez, Sousa Neto and
Gomes (2023)
Conclusion
With the increase in the number of women participating in different sports and with the advancement of sports science, we can then analyze, with more biological parameters, the physiological and biochemical differences between male and female athletes and how they interfere with performance. These differences, presented in the study in general, do affect the female performance in relation to the male. Factors such as a smaller heart, smaller ejection volume, smaller number of pulmonary alveoli, as well as a smaller production of testosterone - a hormone directly related to the lean mass gain, a very important variable within performance -, in addition to other hormonal changes caused by the menstrual cycle, among others, make women have different physiological and biochemical responses.The scientific evidence presented during the study described the main anatomical-physiological and biochemical differences between men and women and how they directly interfere, from the performance process in the training system to performance. Therefore, the application of biochemical markers is of great importance throughout the process, emphasizing that they must be used together and during all phases of training, to be more reliable in their results, in addition to creating biochemical parameters, in order to avoid overtraining and loss of performance.
Another important fact is that there
is no consensus on physiological parameters and specific biochemical markers for
female athletes, and these variables are extremely important for physiologists and
sports coaches. Thus, it is necessary to monitor exercise physiologists throughout
the training process, creating an information system aimed at evaluating each athlete
separately, respecting their biological individualities, aiming to create their
specific physiological and biochemical parameters, avoiding overtraining and performance
loss. Thus, we conclude the need for the development of experimental research that
addresses the theme in question, in order to establish physiological and biochemical
parameters aimed at female athletes, aiming at monitoring the training action, mainly
related to the biochemical markers that directly reveal their effects on the body
female referring to training actions and competitions in which they participate.
Conflict of interest
The authors report that there are no
conflicts of interest
Financing source
The present study was carried out without
funding.
Authors' contribution
Research conception and
design: Cortez ACL, Sousa Neto AB,
Gomes AC; Data analysis and interpretation: Cortez ACL, Sousa Neto AB; Statistical analysis: Cortez ACL, Sousa Neto AB; Writing of the manuscript: Cortez ACL, Sousa
Neto AB, Gomes AC; Critical review of the manuscript
for important intellectual content: Cortez ACL, Gomes AC.
References
- Brandão MRF,
Casal H. Mulheres-atletas e o esporte de rendimento: a questão de gênero. Mulher
e esporte: mitos e verdades. Barueri: Phorte; 2003. p.155-163.
- Smith LL.
Overtraining, excessive exercise, and altered immunity. Sports Med. 2003;33(5):347-364. https://doi.org/10.2165/00007256-200333050-00002 [Crossref]
- Pardini DP. Alterações hormonais da mulher atleta.
Arq Bras Endocrinol. 2001;45(4):343-51. https://doi.org/10.1590/S0004-27302001000400006 [Crossref]
- Fortes MSR, Marson RA, Martinez EC. Comparação de desempenho físico entre homens
e mulheres: revisão de literatura. Revista Mineira de Educação Física. [Internet].
2015 [cited 2022 mar 15];23(2):54-69. Available from: https://periodicos.ufv.br/revminef/article/view/9964
- Harms CA. Does gender affect pulmonary function and exercise capacity? Respir Physiol Neurobiol. 2006;151(2-3):124-31. https://doi.org/10.1016/j.resp.2005.10.010 [Crossref]
- Raso V, Greve
JMD, Polito MD. in Pollock, ed.: Fisiologia clínica do exercício.
São Paulo: Manole; 2013.
- Borin JP, Gomes AC, Santos LG. Preparação desportiva: aspectos do controle da carga de treinamento nos jogos coletivos. Journal of Physical Education. 2007;18(1):97-105. https://doi.org/10.4025/reveducfisv18n1p97-105 [Crossref]
- Gleeson M. Biochemical and immunological markers of overtraining.
J Sports Sci Med. [Internet] 2002 [cited 2023 Jul
21];1(2):31-41. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3963240/
- Baumert M, Brechtel L, Lock J, Hermsdorf M, Wolff R, Baier V, Voss A. Heart rate variability, blood pressure variability, and barorelex sensitivity in overtrained athletes. Clin J Sports Med. 2006;16(5):412-7. https://doi.org/10.1097/01.jsm.0000244610.34594.07 [Crossref]
- Purge P, Jürimäe J, Jürimäe T. Hormonal and psychological adaptation in elite male rowers during prolonged training. J Sports Sci. 2006;24(10):1075-82. https://doi.org/10.1080/02640410500432516 [Crossref]
- Hartmann U, Mester J. Training and overtraining markers in selected sport events. Med Sci Sports Exerc. 2000;32(1):209-215. https://doi.org/10.1097/00005768-200001000-00031 [Crossref]
- Foschini D, Prestes J, Charro MA. Relação entre exercício físico, dano muscular
e dor muscular de início tardio. Rev Bras Cineantropom Desempenho Humano.
[Internet]2007;[cited 2023 Jul
21]9(1):101-6. Available from: https://periodicos.ufsc.br/index.php/rbcdh/article/view/4038
- Totsuka M, Nakaji S, Suzuki K. Break point of serum creatine kinase release after endurance exercise. J Appl Physiol. 2022;93(4):1280-6. https://doi.org/10.1152/japplphysiol.01270.2001 [Crossref]
- Magna CO.
Gênero Textual Ensaio Acadêmico - Suas especificidades e regularidades [Internet].
2014. [cited 2022 Mar 12]. Disponível em: https://trilhante.com.br/trilha/fdrp/sobre/ensaio-academico
- COPE. Committee on Publication
Ethics [Internet]. 2023. [cited 2022 mar 12]. Available from: https://publicationethics.org/
- Brasil. Ministério
da Saúde. Secretaria de Ciência, Tecnologia e Insumos Estratégicos. Departamento
de Ciência e Tecnologia. Diretrizes metodológicas: elaboração de revisão sistemática
e metanálise de ensaios clínicos randomizados. (Série
A: Normas e Manuais Técnicos). Brasília, DF: Ministério da Saúde; 2012.
- Prayag G, Ozanne LK. A systematic review of peer-to-peer (P2P) accommodation sharing research from 2010 to 2016: progress and prospects from the multi-level perspective. Journal of Hospitality Marketing & Management. 2018;27(6):649-78. https://doi.org/10.1080/19368623.2018.1429977 [Crossref]
- Weineck J. Biologia do esporte. 7ª ed. Barueri:
Manole; 2005. 768p.
- Robergs RA, Roberts SO. Adaptações neuroendócrinas
ao exercício. In: Robergs RA, Roberts SO. Princípios fundamentais
de fisiologia do exercício: para aptidão, desempenho e saúde. São Paulo: Phorte; 2002. p.184-205.
- Leitão MB,
Lazzoli JK, Oliveira MABD, Nóbrega ACLD, Silveira GGD,
Carvalho TD, et al. Posicionamento oficial da Sociedade Brasileira de Medicina do
Esporte: atividade física e saúde na mulher. Revista Brasileira de Medicina do Esporte
2000;6:215-20.
- Batlouni M, Schwartz HJ, Ghorayeb
N. Eletrocardiograma. In: Ghorayeb N, Dioguardi GS,
eds. Tratado de cardiologia
do exercício e esporte. São Paulo: Atheneu; 2007.
- Costill DL, Wilmore JH.
Fisiologia do Esporte e do Exercício. 2ª ed. São Paulo: Manole; 2001. 728p.
- Araújo MR. A influência do treinamento de força e do treinamento aeróbio sobre as concentrações hormonais de testosterona e cortisol. Motricidade 2008;4(2):67-75. https://doi.org/10.6063/motricidade.4(2).513 [Crossref]
- Gerlinger-Romero F, Caperuto
EC, Maia AF, Guimarães-Ferreira L. Bases moleculares das ações da testosterona,
hormônio do crescimento e igf-1 sobre a hipertrofia muscular esquelética e respostas
ao treinamento de força. Revista Mackenzie de Educação Física e Esporte [Internet].
2014;12(2). [cited 2023 Fev 12]. Available from: https://editorarevistas.mackenzie.br/index.php/remef/article/view/2100
- Åstrand P, Rodahl
K, Dahl HÁ, Strømme SB. Tratado de fisiologia do trabalho. 4ª ed.
Porto Alegre: Artmed; 2006. 560p.
- Baumann G. Growth hormone-binding proteins: state of the art. J. Endocrinol 1994;141:1-6. https://doi.org/10.1677/joe.0.1410001 [Crossref]
- Strobl JS, Thomas MJ. Human growth hormone. Pharmacol Rev. [Internet]. 1994;46:1-34.
[cited 2023 Fev 12]. Available from: https://pubmed.ncbi.nlm.nih.gov/8190748/
- Adams GR. Insulin-like growth factor in muscle growth and potential abuse by athletes. Br J Sports Med. 2000;34:412-3. https://doi.org/10.1136/bjsm.34.6.412 [Crossref]
- Rosen CJ. Growth hormone and aging. Endocrine. 2000;12:197-201. https://doi.org/10.1385/ENDO:12:2:197 [Crossref]
- Rennie MJ. Claims for the anabolic effects of growth hormone: a case of the Emperor's new clothes? Br J Sports Med. 2003;37:100-5. https://doi.org/10.1136/bjsm.37.2.100 [Crossref]
- Gomes MR, Pires I, Castro IA, Tirapegui J. Effect of moderate physical exercise on plasma and tissue levels of insulin-like growth factor-1 (IGF-1) in adult rats. Nutr Res. 2004;24:555-64. https://doi.org/10.1016/j.nutres.2004.04.003 [Crossref]
- Lange KHW. Fat metabolism in exercise - with special reference to training and growth hormone administration. Scand J Med Sci Sports. 2004;14:74-99. https://doi.org/10.1111/j.1600-0838.2004.381.x [Crossref]
- Machida S, Booth FW. Insulin-like growth factor 1 and muscle growth: implications for satellite cell proliferation. Proc Nutr Soc. 2004;63:337-40. https://doi.org/10.1079/PNS2004354 [Crossref]
- Petibois C, Cazorla G, Déleris G. The biological and metabolic adaptations to 12 months training in elite rowers. Int J Sports Med. 2003;24(1):36-42. https://doi.org/10.1055/s-2003-37194 [Crossref]
- Margonis K, Fatouros IG, Jamurtas AZ, Nikolaidis MG, Douroudos I, Chatzinikolaou A, et al. Oxidative stress biomarkers responses to physical overtraining: implications for diagnosis. Free Radic Biol Med. 2007;43(6):901-7. https://doi.org/10.1016/j.freeradbiomed.2007.05.022 [Crossref]
- Rogero MM, Mendes RR, Tirapegui J. Aspectos neuroendócrinos e nutricionais em atletas com overtraining. Arq Bras Endocrinol Metab. 2005;49(3):359-68. https://doi.org/10.1590/S0004-27302005000300006 [Crossref]
- Varlet-Marie E, Gaudard
A, Mercier J, Bressolle F, Brun J-F. In the feeling of heavy legs in overtrained
athletes related to impaired hemorheology? Clin Hemorheol Microcirc. [Internet]. 2003 [cited 2022 Mar 12];28(3):151-9. Available from: https://pubmed.ncbi.nlm.nih.gov/12775897/
- Martínez-Amat A, Boulaiz H, Prados J, Marchal JA, Puche PP, Caba O, et al. Release of a-actin into serum after skeletal muscle damage. Br J Sports Med. 2005;39(11):830-4. https://doi.org/10.1136/bjsm.2004.017566 [Crossref]
- Brancaccio P, Limongelli FM, Maffulli N. Monitoring of sérum enzymes in sport. Br J Sports Med. 2006;40:96-7. https://doi.org/10.1136/bjsm.2005.020719 [Crossref]
- Mougios V. Reference intervals for serum creatine kinase in athletes. Br J Sports Med. 2007;41(10):674-8. https://doi.org/10.1136/bjsm.2006.034041 [Crossref]
- Nikolaidis MG, Protosygellou MD, Petridou A, Tsalis G, Tsigilis N, Mougios V. Hematologic and biochemical profile of juvenile and adult athletes of both sexes: implications for clinical evaluation. Int J Sports Med. 2003;24(7):506-11. https://doi.org/10.1055/s-2003-42014 [Crossref]
- Hecksteden A, Pitsch W, Julian R, Pfeiffer M, Kellmann M, Ferrauti A, et al. A new method to individualize monitoring of muscle recovery in athletes. International J Sports Physiol Perform. 2017;12(9):1137-42. https://doi.org/10.1123/ijspp.2016-0120 [Crossref]
- Farhana A, Lappin SL. Biochemistry, lactate dehydrogenase.
[Updated 2023 May 1]. In: StatPearls [Internet]. Treasure
Island (FL): StatPearls Publishing; 2023 jan. Available from: https://www.ncbi.nlm.nih.gov/books/NBK557536/
- Sahran Y, Sofian AM, Saad AZM. Pre-treatment serum lactate dehydrogenase (LDH) and serum alkaline phosphatase (ALP) as prognostic factors in patients with osteosarcoma. J Cancer Prev Curr Res. 2018;9(2):58-63. https://doi.org/10.15406/jcpcr.2018.09.00320 [Crossref]
- Mohebbi H, Rahmani-Nia F, yar Arabmomeni, A, Riasi A, Marandi M. The effects of interval training and age on blood lactate (La) levels and lactate dehydrogenase (LDH) activity in male Wistar rats. Pars Journal of Medical Sciences. 2015;12(4):37-45. https://doi.org/10.29252/jmj.12.4.4 [Crossref]
- Vanderschueren S, Deeren D, Knockaert DC, Bobbaers H, Bossuyt X, Peetermans W. Extremely elevated C-reactive protein. Eur J Intern Med. 2006;17:430–3. https://doi.org/10.1016/j.ejim.2006.02.025 [Crossref]
- Pepys MB, Hirschfield GM. C-reactive protein: a critical update. J Clin Invest. 2003;111(12):1805-12. https://doi.org/10.1172/JCI18921 [Crossref]
- Koenig W, Khuseyinova N. Biomarkers
of atherosclerotic plaque instability and rupture. Arterioscl Thromb Vasc Biol. 2007;27(1):15–26. https://doi.org/10.1161/01.ATV.0000251503.35795.4f [Crossref]
- Naoum FA, Naoum PC.
Hematologia laboratorial. Leucócitos. São José do Rio Preto: Academia de Ciência
e Tecnologia; 2006.
- Lee EC, Fragala MS, Kavouras SA, Queen RM, Pryor JL, Casa DJ. Biomarkers in sports and exercise: tracking health, performance, and recovery in athletes. J Strength Cond Res. 2017;31(10):2920. https://doi.org/10.1519/JSC.0000000000002122 [Crossref]
