Rev Bras Fisiol Exerc. 2024;23(2):e235589
doi: 10.33233/rbfex.v23i2.5589ORIGINAL ARTICLE
Impact of different training protocols on muscle synergism in maximal and
submaximal strength tests in bench press exercise
Impacto de diferentes
protocolos de treinamento no sinergismo muscular, em testes de força máxima e
submáxima no exercício supino reto
Daniel Cesar Teixeira1,
André Gustavo Pereira de Andrade1, Hugo Cesar Martins-Costa1,2,
Lucas Tulio Lacerda1, Mateus Camargos Gomes1, Mauro
Heleno Chagas1, Rodrigo César Ribeiro Diniz1, Fernando
Vitor Lima1
1Universidade Federal de Minas Gerais, Belo Horizonte, MG,
Brazil
2Pontifícia Universidade Católica de Minas Gerais, Belo
Horizonte, MG, Brazil
Received: April 19, 2024; Accepted:
July 20, 2024.
Correspondence: Fernando Vitor Lima, erlima@eeffto.ufmg.br
How to cite
Teixeira DC, Andrade AGP,
Martins-Costa HC, Lacerda LT, Gomes MC, Chagas MH, et al. Impact of
different training protocols on muscle synergism in maximal and submaximal
strength tests in bench press exercise. Rev Bras Fisiol
Exerc. 2024;23(2):e235589. doi:
10.33233/rbfex.v23i2.5589
Abstract
Objective: This study analyzed the activation of pectoralis major
and triceps brachii muscles in strength tests in bench press after 10 weeks of
training. Methods: Thirty-three untrained individuals were divided into
two experimental and one-control groups. Protocols were matched by intensity
(50-55% of one repetition maximum - 1RM), frequency (3 times a week), pause
between sets (3 minutes), number of sets (3 to 4 sets), and time under tension
in each set (36 seconds), but with different repetition number and duration (12
repetitions vs. 3seconds / 6repetitions vs. 6seconds). Results: In
strength endurance test both experimental groups increased amplitude of
Electromyography (EMG) signal in comparison to control group, but with no
difference between them. Activation was higher for triceps brachii than for
pectoralis major and thus the pectoralis major/triceps brachii activation ratio
significantly decreased for both groups, but with no difference between them.
In the 1RM and maximum voluntary isometric contraction tests, EMG signal
amplitude, activation ratio and analysis of cross-correlation did not exhibited
any changes when comparing the experimental and control groups. Conclusion:
The results showed that the fact that the protocols used dynamic actions, as
well as the same time under tension (TUT), and the differences between single
and multiple repetition tests, determined the responses verified.
Keywords: electromyography; muscle strength, pectoralis muscles;
skeletal muscle.
Resumo
Objetivo: Este estudo analisou a ativação dos
músculos peitoral maior (PM) e tríceps braquial (TB) em testes de força no
supino após 10 semanas de treinamento. Métodos: Trinta e três indivíduos
não treinados foram divididos em dois grupos experimentais e um grupo controle.
Os protocolos foram equiparados em termos de intensidade (50-55% de uma
repetição máxima - 1RM), frequência (3 vezes por semana), pausa entre as séries
(3 minutos), número de séries (3 a 4 séries) e tempo sob tensão em cada série
(36 segundos), mas com número de repetições e duração diferentes (12 repetições
vs. 3 segundos / 6 repetições vs. 6 segundos). Resultados: No teste de
resistência de força, ambos os grupos experimentais aumentaram a amplitude do
sinal eletromiográfico (EMG) em comparação com o
grupo controle, mas sem diferença entre eles. A ativação foi maior para o
tríceps braquial do que para o peitoral maior e, portanto, a relação de
ativação do peitoral maior/tríceps braquial diminuiu significativamente em
ambos os grupos, mas sem diferença entre eles. Nos testes de 1RM e de contração
isométrica voluntária máxima, a amplitude do sinal EMG, a relação de ativação e
a análise de correlação cruzada não apresentaram nenhuma alteração na
comparação entre os grupos experimental e de controle. Conclusão: Os
resultados mostraram que o fato de os protocolos utilizarem ações dinâmicas,
bem como o mesmo tempo sob tensão (TST) e as
diferenças entre os testes de repetição única e múltipla, determinaram as
respostas verificadas.
Palavras-chave: eletromiografia; força muscular,
músculos peitorais; músculo esquelético.
Introduction
Among the determinants of strength performance, the
synergistic activation of two or more muscles can be adjusted for greater
efficiency in situations of sports performance and rehabilitation. Such
determinants should be considered according to the exercise [1,2], training
status [3,4], degrees of freedom of the exercise [5] the training-related
variables [4,6] and exercise technique [1]. Marchetti et al. [1]
analyzed the activation ratio between upper and lower portions of the rectus
abdominis during isometric trunk and hip flexion with maximal and submaximal
intensity and found significantly higher values with trunk flexion. Kristiansen
et al. [7] compared the EMG of pectoralis major (PM) and triceps brachii
(TB) in three sets at 60% of 3RM, between powerlifters and untrained
individuals and suggested that different training loads and exercise techniques
can result in muscle activation changing in diverse ways.
Different time under tension (TUT) can produce different
results in EMG [8] and this has been manipulated by changing both the number
and the duration of repetitions in training programs developed by coaches and
in physical rehabilitation protocols. In bench press exercise, the PM and TB
muscles may present different activation patterns and this can be verified
between sets when performing this exercise with the same TUT but different
number and duration of repetitions [8,9]. Sakamoto et al. [10] showed
that PM and TB may differ in activation at different intensities and repetition
durations in BP exercise.
Although in situations of maximum strength performance in
single-joint exercises, muscles could be expected to reach maximum activation
or close [11], it would be necessary to understand if the synergism could be
changed differently in strength performance tests after training with different
protocols in multi-joint exercises. In addition, it should be investigated
whether synergism can be altered in dynamic and isometric maximal strength
tests when only one repetition is performed compared to a test with multiple
repetitions, where, in principle, a longer duration of the task could allow
differentiated adjustments of muscle activations throughout of the sets to
produce the best performance. This is necessary because training to improve
strength performance in different manifestations (maximum and
strength-endurance), aiming for maximum and/or adequate activation of the
muscles is carried out with different multiple repetition protocols, with
different repetitions number and duration and also different configurations of
TUT. Therefore, this study aimed to investigate the effect of 10 weeks of
training with protocols matched by TUT but with different number and duration
of repetitions, on the activation of the PM and TB muscles in isometric and
dynamic strength tests.
Methods
Sample
Thirty-three men participated in the study (age 24.1 ±
4.8 years old; body mass = 75.9 ± 10.4 kg; height 175.6 ± 6.4 cm). The sample
size calculation was performed using the software G Power (version 3.1.9.2),
considering an effect size of 0.48, obtained by the pre- and post-test values
of the PM muscle EMG signal in young adults in the Baker et al. [12]
study. Individuals who did not perform strength training in the last six months
and did not have wrist, elbow and shoulder joint injuries were selected. This
study was approved by the local Ethics Committee, and received registration and
identification as a clinical trial (https://doi.org/10.17605/OSF.IO/BGJCV). All
procedures were conducted according to the Declaration of Helsinki. Subjects
were informed about the study aims, procedures, and risks and signed an
informed consent form.
Experimental design
All tests and training procedures were carried out in the
BP exercise on a Smith machine (MASTER®, Brazil). A rotary-encoder-type
position sensor (BOURNS, United States; 1.2-mm precision) was coupled to the
equipment and the data obtained were transformed from analog to digital signals
by a converter board (BIOVISION, Germany), directed to the computer (frequency
of 4,000 Hz sampling), subsequently filtered (10hz low-pass Butterworth filter,
2nd order) and analyzed using specific software (DASYLAB 11.0, United States).
Volunteers lay down on the bench and placed their hands on the bar at a
distance corresponding to twice the biacromial distance, using the middle
finger as a reference. To ensure the same positioning in all sessions,
measuring tapes were fixed on the bar and on the bench, which served as a
reference to reproduce the hand and head locations.
Strength tests
Strength endurance (SE) test consisted of the maximum
number of repetitions (MNR) in a single set with mass corresponding to 70% of
one repetition maximum (1RM). 1RM test was performed according to the procedure
used by Lacerda et al. [13] To determine the range of motion (ROM) in
the maximum voluntary isometric contraction (MVIC) test, the bar was fixed in a
position corresponding to 50% of the maximum linear displacement, which also
corresponded to approximately 90° of elbow flexion; then, the volunteer should
apply maximum force against the bar for 5s. Two maximum contractions were
carried out, with 2-minutes rest interval.
Training sessions
Protocols were performed for 10 weeks, matched by the TUT
in each set (36s), intensity (50-55% 1RM), training frequency (3 times a week
with intervals of 48 to 72 hours between sessions), 3 min rest between sets and
different duration and number of repetitions (Figure 2). Initially, three sets
were performed at 50% 1RM, adding one set in the fourth week, and the intensity
of 55% 1RM was adopted in the sixth week. 1RM test was performed every two
weeks to adjust the intensity, 10 minutes before the protocol was started [14].
Control group was instructed not to change their daily habits throughout the
study.
Electromyography
For the recording of the EMG signal, bipolar surface
electrodes (Ag/AgCl) were positioned according to the procedures described by
Lacerda et al. [9]. In PM, they were positioned horizontally at the
point of greatest muscle belly with the arm positioned close to the trunk [15].
For TB, SENIAM´s (Surface Electromyography for the Non-Invasive Assessment of
Muscles) guidelines were followed, determining a point corresponding to half
the distance between the posterior crest of the acromion and the olecranon.
After acquisition, data were amplified 500 times and then stored. They were
later filtered by a second order Butterworth bandpass filter (20-500 Hz) and
rectified to calculate the signal amplitude with the root mean square (RMS). In
the 1RM test, the RMS of the entire repetition was used, and in the MVIC test,
the 1-s RMS around the peak of activation of each muscle was considered.
Raw EMGRMS values of 1RM and MVIC tests were standardized
by the average EMGRMS of two 5s MVIC attempts. To check the reliability of
these measures, intraclass correlation coefficients (ICC) were calculated in
two ways: intrasession ICC (two intrasession MVIC attempts) and intersession
ICC (mean of the two measures recorded in the group’s pre-test and post-test,
together with the Standard Error of Measurement (SEM) [16], shown in table I.
Table I - Reliability of MVIC measurements
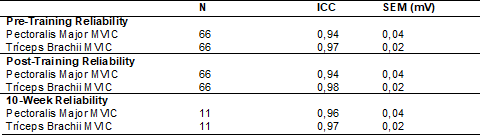
n = number of measurements (2 MVIC attempts); ICC =
intraclass correlation coefficient; SEM (mV) = standard error of measurement in
millivolts; MVIC = maximum voluntary isometric contraction test
In the SE test, a dynamic normalization procedure was
used with two repetitions, each one with 4s (2s concentric: 2s eccentric) and
intensity of 70% 1RM, according to the procedure performed by Sakamoto and
Sinclair [10] and Lacerda et al. [9,13]. Mean EMGRMS of the repetitions
was used as a reference for the measurements performed during the test. To
check if the EMGRMS values between the sessions were reproducible, the
intersession reliability during the normalization test that was performed in
the second and thirteenth weeks was checked by calculating the intraclass
correlation coefficient (ICC) together with the SEM [16]. Reliability and SEM
data are shown in table II. Considering that in this test each volunteer
performed a different NMR, to perform the analysis of the normalized EMGRMS,
the first, median and last repetitions of each volunteer were used.
Table II - Reliability of EMGRMS intersession measures of the
normalization test in the bench press exercise

n = number of measurements; ICC = intraclass correlation
coefficient; SEM (mV) = absolute standard error of measurement; PM = pectoralis
major; TB = triceps brachii
Measured variables
Pre- and post-training EMG amplitude analysis was
performed to identify the influence of the protocols on muscles activation
during strength tests. PM/TB ratio was determined with a mathematical ratio, by
dividing the normalized EMGRMS values of PM by the TB. In this study, cross
correlation analysis correlated two time-variable signals comparing each other.
This process involves repeatedly shifting one signal back and forth in time
with the other fixed signal, with each time variation of one of the signals
generating a comparison and R value for correlation. By decomposing these
values, a final correlation or similarity value between the two signals was
obtained [17].
Statistical analysis
Initially, a descriptive data analysis was carried out.
Normality and homogeneity were verified by using the Shapiro-Wilk and Levene
tests respectively, and all study variables were shown as mean and standard
deviation. Analysis of the EMG signal amplitude values of PM and
TB was carried out using an ANOVA three way mixed
with repeated measures (Factor 1 – Time; Factor 2 – Muscle;
Factor 3 – Protocol). Two other ANOVA’s two
way with repeated measures (factors 1 – Time and 2 – Protocol) were carried out, one for activation ratio (PM/TB) and another for cross-correlation analysis. In the
presence of a significant value of F, it was applied as post hoc of Bonferroni.
For each ANOVA, the eta squared (η2) was
determined. Statistical procedures used were performed using the SPSS
statistical package (version 22.0). Significance level adopted for all analyses
was p < 0.05.
Results
EMG Signal Amplitude
In the SE test, ANOVA three-way with repeated measures
checked for an interaction between the factors: Time vs. protocol vs. muscle
(F2.46 = 4.93, p = 0.011, power = 0.78, η2 = 0.026).
Post hoc showed no differences in normalized EMGRMS between the experimental
groups in the pre-test and significant increase in the post-test but with no
differences between them. Values were similar between muscles in all groups in
pre-test, whereas the values in TB were higher than PM in post-test for
experimental groups (Figure 1).

*Post-test > Pre-test; # TB > PM; $ Protocols A and
B > control; PM = Pectoralis major; TB = Triceps brachii; Protocol A =12
repetitions, 3s; Protocol B = 6 repetitions, 6s
Figure 1 - Normalized EMGRMS of strength endurance test
between protocols, pre- and post-training
EMGRMS values of the 1RM test presented no changes in
experimental groups in the interactions between the factors time, muscle, and
protocol. The analysis of the main effects found a significant effect of the
Time factor (F1; 9 = 6.10; p = 0.036; η2 = 0.026;
power = 0.726), and according to the post hoc of Bonferroni, the post-test was
higher than the pre-test, as shown in Figure 2. Muscle and protocol factors
showed no changes. Also, no changes in the EMGRMS signal amplitude in both
muscles in neither of the main factors nor in the interaction between the
factors was verified in MVIC test.
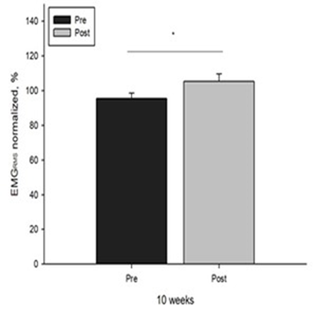
EMGRMS normalized % = normalized electromyography values
through root mean square shown in percentage; * = values different from each
other with a 10-week training interval (p < 0.05)
Figure 2 - Main effect 1RM test time
Activation ratio
In the SE test, ANOVA three-way with repeated measures
checked for an interaction between the factors protocol vs. time (F2.46 = 4.02,
p = 0.024, power = 0.69, η2 = 0.05);
post hoc pointed out no significant differences in the pre-test between the
groups; in the post-test, only experimental groups significantly decreased the
activation ratio, but with no differences between them (Figure 3). There was no
significant difference in the PM/TB ratio in the 1RM and MVIC post-tests. ANOVA
two way did not detect significant differences in the main factors and their
interactions.
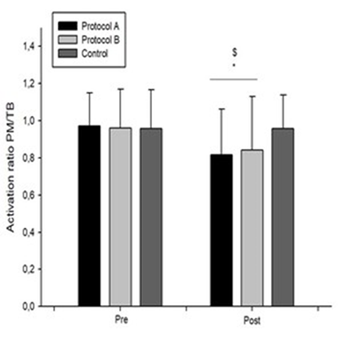
* PM/TB activation ratio Post < Pre; $ Protocols A and
B < control; Protocol A = 12 repetitions, 3s; Protocol B = 6 repetitions, 6s
Figure 3 - PM/TB activation ratio between pre- and
post-training protocols in the strength endurance test
Cross-correlation
Cross-correlation analysis in SE test found no
interactions between the factors: protocol vs. time (F2.20 = 0.998, p = 0.386,
power = 0.199, η2 = 0.021).
There were also no main effects of time (F1.10 = 0.571, p = 0.467, power =
0.105, η2 = 0.007)
and protocol (F2.20 = 1.823, p = 0.187, power = 0.335, η2 = 0.119)
(Figure 4).
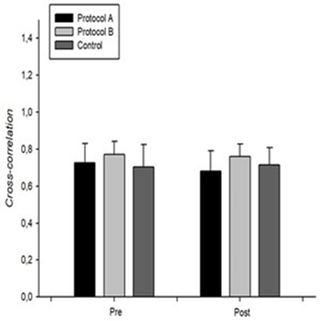
Protocol A = 12 repetitions, 3s; Protocol B = 6
repetitions, 6s
Figure 4 - Cross-correlation analysis of the strength
endurance test shown as mean and standard deviation
Figure 5 shows the
cross-correlation results of 1RM and MVIC tests, respectively. Mean values of
all groups were 0.83 (SD = 0.08) in the pre-test, and 0.80 (SD = 0.08) in the
1RM post-test; and 0.90 (SD = 0.11) in the pre-test and 0.92 (SD = 0.04) in the
MVIC post-test, with no differences in any of the analyses. ANOVA’s two way
found no significant differences in the main factors time and protocol and in
their interactions in the 1RM test. No significant differences were identified
in the main factors and interactions in the MVIC test.
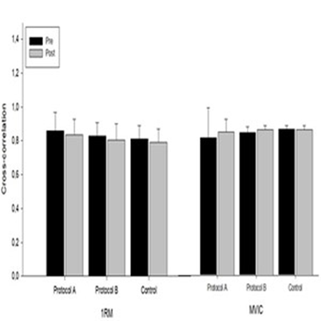
Protocol A = 12 repetitions, 3s; Protocol B = 6 repetitions, 6s
Figure 5 - Cross-correlation analysis of 1RM and MVIC tests
shown as mean and standard deviation; Shape analysis of the gross
electromyographic signal of pectoralis major and triceps brachial muscles
Discussion
This study investigated changes in EMG signals in
different strength tests after 10 weeks of training with two different
protocols matched by the TUT and different number and duration of repetitions.
SE test showed a significant increase in EMGRMS values in
the post-test with no differences between the protocols. Our study observed a
significant increase in MNR in post-test in both protocols and this can result
in a greater EMG amplitude, especially when repetitions until muscle failure
are performed [18]. To compensate for the drop in nerve impulse conduction
speed due to fatigue, more motor units (MU) tend to be recruited [18]. It was
not verified differences in muscle activation in pre-training situation between
groups of untrained individuals for SE testing, but training can change it
regardless of the number an duration of repetitions if the TUT is equalized.
However, activation in TB increased more than in PM. Stastny et al. [19]
demonstrated that the TB is more sensitive than PM to changes in training load,
thus presenting greater variability in its activation. Although Lacerda et
al. [9] did not make comparisons between muscles, they verified higher
variations in TB than in PM after three sets in BP exercise. Van Den Tillar et
al. [20] verified a higher capacity to produce force at the beginning of
the concentric action in BP until it reaches the sticking point, and PM does
not change activation throughout ROM, but TB presents continuous increase in
activation. TB muscle has greater pennation angles and, consequently, a greater
capacity to produce torque throughout the concentric ROM [21], and could remain
more activated at this muscle action. This difference in favor of TB can
explain the decrease in PM/TB ratio in SE, indicating a change in relative
activation of TB compared to PM; activation ratio is commonly used to estimate
the relative activation between muscles in an exercise [1,22]. However, no
difference was found between protocols, suggesting that the similar TUT between
the protocols was decisive in this response, despite the different number and
duration of repetitions.
Higher EMGRMS values in 1 RM post-test corroborates
Sampson and Groeller [23] who verified, after 12 weeks of training with
different repetition durations, an increase in EMG in 1RM test of elbow flexors
but without differences between protocols. Van der Tillaar et al. [20]
verified greater muscle activation in the dynamic 1RM test compared to another
isometric test, but pointed out that it was not possible to explain this
result. The highest values in this study may be related to greater recruitment
and MU synchronization to produce the higher strength performance in post-test.
However, this did not occur with MVIC in both studies, which suggests that
these changes are due to the dynamic nature of training and would not be
carried over to an isometric action. Clark et al. [24] also did not see
changes in EMG signal in PM and TB during MVIC after 5 weeks of training in
bench press exercise in different ROM.
No differences were verified in PM/TB ratio in both 1RM and CVIM tests. Van der Tillaar et al.
[20] found that the EMG activity were higher in 1RM compared to isometric
acute test, but this was
the only difference verified in EMG activity between these two different
tests. Our study analyzed two muscles in two different joints in
the same exercise. According to Prilutsky [25], the analysis of synergism must
consider the differences between exercises that require muscles with different
actions in different joints and others with more than one muscle acting in two
joints. This author states that during the control of the force exerted on a
proximal or distal segment, or when external resistance is applied to two or
more joints, the activation of multi-joint muscles seems to strongly depend on
the direction of the moments of force on the joints. Although training can
induce adjustments in the coordinated activation of the muscles aiming at
greater efficiency, this does not seem to be the case in our study. It can be
suggested that in only one repetition, dynamic or isometric, there would be
little time for adjustments in the coordination between the muscles, even more
so in situations of maximum strength and muscle activation demands.
No significant differences were found in the
cross-correlation analysis, both between pre- and post-test and between
protocols. The effect of 5 weeks of training on the synergism of 13 muscles,
including PM and TB, in BP exercise were analysed and no differences was
verified in cross-correlation between the experimental and control groups [4].
High cross-correlation value with no differences between two tasks was verified
in two portions of rectus abdominis muscle, identifying a common pattern in the
activation of these portions [1]. In the same way and considering that the
cross correlation measure refers to the variation of activation over time, in
our study, it appears that regardless of the demand, when the muscles are
jointly producing force there seems to be some constant pattern of activation
along time and this happens regardless if the performance is short with only
one repetition or longer with multiple repetitions, and this may not be
influenced by some different training protocols that induce strength gain, even
in multi joint exercise. Furthermore, it must be considered that there would be
differences in muscle coordination patterns depending on strength demand. For
example, in situations of maximum effort, not all muscles can be activated to
their maximum, that is, even the muscles that can contribute to maximum force
production may not be activated to their full potential [26].
This study showed the impact of training on the
activation ratio between the PM and TB muscles in a strength test with multiple
repetitions but not in the tests of only one repetition. It is unknown whether
these differences arise from the variability of the adjustments in the degrees
of freedom of the elbow during movement, which could occur in multiple
repetitions. Moreover, it could be considered that the limited degrees of
freedom of the Smith machine would not have allowed significant changes in trajectories
of elbows in both protocols, whether single or multiple sets, also contributing
to the smaller differences verified in the results. However, in a 1RM test, the
EMGRMS recorded no differences in the comparison between these two equipments
[27]. In a similar study, Schick et al. [28] analyzed the EMG of PM
using Smith machine and free weights in two strength tests (70% and 90% 1RM)
and found no differences in the amplitudes of the EMG signal. Perhaps, the
difference observed only in the SE test is closer to the similarity with the
training protocols than to a possible variability in the movement between
repetitions.
Conclusion
The results showed that the fact that the protocols used
dynamic actions, as well as the same TUT in both protocols and the differences
between single and multiple repetition tests, appeared to play a significant
role in the responses.
The complexity of understanding synergism may require
additional analyzes beyond those performed in the present study. In addition,
performance can also be evaluated in different ways, as well as in different
exercises with different combinations of muscle groups. Thus, it appears that
care must be taken when interpreting these results and further studies should
be carried out before concluding information on this topic.
Academic affiliation
This article represents part of Daniel Cesar Teixeira's
master's thesis, supervised by professor Dr. Fernando Vitor Lima (UFMG)
Conflict of interest
The authors declare no conflicts of interests.
Funding
There was no funding.
Authors’ contributions
Conception and experimental design: Teixeira DC, Lima FV, Chagas
MH, Martins-Costa HC, Lacerda LT, Diniz RCR; Data acquisition:
Teixeira DC, Gomes MC; Data analysis and interpretation: Teixeira
DC, Gomes MC, Andrade AGP, Diniz RCR, Martins-Costa HC; Statistical analysis: Teixeira DC, Andrade AGP; Manuscript writing: Teixeira DC, Lima FV; Critical revision of the manuscript and intellectual content: Lima FV, Chagas MH
References
- Marchetti PH, Kohn AF,
Duarte M. Selective activation
of the rectus
abdominis muscle during low-intensity and fatiguing tasks
(Ativação seletiva do músculo reto abdominal durante tarefas de baixa
intensidade e fadiga). J Sports Sci Med. 2011;10:322-27.
- Jaberzadeh S, Yeo D, Zoghi M. The effect of altering knee
position and squat depth on VMO: VL EMG durante
exercícios de agachamento. Physiother Res Int 2015;21(3):164-73. doi: 10.1002/pri.1631 [Crossref]
- Kutch JJ, Kuo AD, Bloch AM, Rymer WZ. As flutuações de força do ponto final revelam padrões flexíveis, em vez de sinérgicos, de cooperação muscular. J Neurophysiol. 2008;100:2455-71. doi: 10.1152/jn.90274.2008 [Crossref]
- Kristiansen M, Samani A, Madeleine P, Hansen, EA. Effects of 5 weeks of bench press training on muscle synergies: a randomized controlled study. J Strength Cond Res. 2015;30(7):1948-59. doi: 10.1519/JSC.0000000000001282 [Crossref]
- Kornecki S, Kebel A, Siemienski A. Muscular co-operation during joint stabilization, as reflected by EMG. Eur J Appl Physiol. 2001;84:453-61. doi: 10.1007/s004210100401 [Crossref]
- Wong YM, NG G. Resistance training alters the sensorimotor control of vasti muscles. J Electromyogr Kinesiol. 2010;20:180-84. doi: 10.1016/j.jelekin.2009.02.006 [Crossref]
- Kristiansen, M, Madeleine P, Hansen EAM, Samani A. Inter-subject variability of muscle synergies during bench press in power lifters and untrained individuals. Scand J Med Sci Sports. 2013;25:89-97. doi: 10.1111/sms.12167 [Crossref]
- Martins-Costa HC, Diniz RCR, Lima FV, Machado SC, Almeida, RSV, Andrade AGP, Chagas MH. Longer repetition duration increases muscle activation and blood lactate response in matched resistance training protocols. Motriz: Rev Educ Fis. 2016;22(1):35-41. doi: 10.1590/S1980-65742016000100005 [Crossref]
- Lacerda L, Martins-Costa H, Diniz R, Lima F, Andrade A, Tourino F, et al. Variations in repetition duration, and repetition numbers influence muscular activation and blood lactate response in protocols equalized by time under tension. J Strength Cond Res. 2016;30:251-58. doi: 10.1519/JSC.0000000000001044 [Crossref]
- Sakamoto A, Sinclair PJ. Muscle activations under varying lifting speeds and intensities during bench press. Eur J Appl Physiol. 2012;112:1015-25. doi: 10.1007/s00421-011-2059-0 [Crossref]
- Noorkoiv M, Nosaka K, Blazevich, AJ. Neuromuscular adaptations associated with knee joint angle-specific force change. Med Sci Sports Exerc. 2014;46(8):1525–37. doi: 10.1249/MSS.0000000000000269 [Crossref]
- Baker D, Wilson G, Carlyon R. Periodização: The effect on strength of manipulating volume and intensity. J Strength Cond Res. 1994;8(4):235-42. doi: 10.1519/00124278-199411000-00006 [Crossref]
- Lacerda L, Marra-Lopes R, Diniz RCR, Lima FV, Rodrigues SA, Martins-Costa H, et al. Is performing repetitions to failure less important than volume for muscle hypertrophy and strength? J Strength Cond Res. 2020;34(5):1237-48. doi: 10.1519/JSC.0000000000003438 [Crossref]
- Wakahara T, Miyamoto N, Sugisaki N, Murata K, Kanehisa H, Kawakami, et al. Association between regional differences in muscle activation in one session of resistance exercise and in muscle hypertrophy after resistance training. Eur J Appl Physiol. 2012;112:1569-76. doi: 10.1007/s00421-011-2121-y [Crossref]
- Lagally KM, McCaw ST, Young GT, Medema HC, Thomas DQ. Ratings of perceived exertion and muscle activity during the bench press exercise in recreational and novice lifters. J Strength Cond Res. 2004;18(2):359-364. doi: 10.1519/R-12782.1 [Crossref]
- Portney LG, Watkins MP. Foundations of clinical research: applications to
practice. 3rd ed. Upper Saddle River: F.A. Davis Company; 2008.
- Wren TAL, Do KP, Rethlefsen, SA, Healy, B. Cross-correlation as a method for comparing dynamic electromyography signals during gait. J Biomech. 2006;39:2714-18. doi: 10.1016/j.jbiomech.2005.09.006 [Crossref]
- Looney DP, Kraemer WJ, Joseph MF, Comstock BA, Deneger CR, Flanagan SD,
Newton RU. Electromyographical and perceptual responses to different resistance
intensities in a squat protocol: does performing sets to failure with light
loads produce the same activity? J Strength Cond Res. 2015;30(3):792–99. doi: 10.1519/JSC.0000000000001109 [Crossref]
- Stastny P, Golas A, Blazek D, Maszczyk A, Wilk M, Pietraszewski P, et al. A systematic review of surface electromyography analyses of the bench press movement task. PlosOne 2017;12. doi: 10.1371/journal.pone.0171632 [Crossref]
- Van Den Tillar R, Saeterbakken AH, Ettema G. Is the occurrence of the sticking region the result of diminishing potentiation in bench press? J Sports Sci. 2012;30(6):591-99. doi: 10.1080/02640414.2012.658844 [Crossref]
- Murray WM, Buchanan TS, Delp SL. The isometric functional capacity of muscles that cross the elbow. J Biomech. 2000;33(8):943-52. doi: 10.1016/s0021-9290(00)00051-8 [Crossref]
- Matheson JW, Kernozek TW, Fater DC, Davies GJ. Electromyographic activity and applied load during seated quadriceps exercises. Med Sci Sports Exerc. 2001;33(10): 1713-25. doi: 10.1097/00005768-200110000-00016 [Crossref]
- Sampson JA, Groeller H. Is repetition failure critical for the development of muscle hypertrophy and strength? Scand J Med Sci Sports. 2016;24(4):375-83. doi: 10.1111/sms.12445 [Crossref]
- Clark RA, Humphries B, Hohmann E, Bryant AL. The influence of variable range of motion training on neuromuscular performance and control of external loads. J Strength Cond Res. 2011;25(3):704-11. doi: 10.1519/JSC.0b013e3181c6a0ff [Crossref]
- Prilutsky BI. Coordination of two- and one-joint muscles: funcional consequences and implications for motor control. Motor Control 2000;4:1-44. doi: 10.1123/mcj.4.1.1 [Crossref]
- Wakeling JM, Blake OM, Wong I, Rana M, Lee SSM. Movement mechanics as a determinate of muscle structure, recruitment and coordination. Philos Trans R Soc Lond B Biol Sci. 2011;366(1570):1554-64. doi: 10.1098/rstb.2010.0294 [Crossref]
- Saeterbakken AH, Van Den Tillaar R, Fimland MS. A comparison of muscle activity and 1-RM strength of three chest-press exercises with different stability requiriments. J Sports Sci. 2011;29(5):533-38. doi: 10.1080/02640414.2010.543916 [Crossref]
- Schick EE, Coburn, JW, Brown LE, Judelson DA, Khamoui AV, Tran TT, Uribe BP. A comparison of muscle activation between a Smith machine and free weight bench press. J Strength Cond Res. 2010;24(3):779-84. doi: 10.1519/JSC.0b013e3181cc2237 [Crossref]
