Rev Bras Fisiol Exerc.
2024;23(3):e235602
ORIGINAL ARTICLE
Screening for RED-S in female street runners: an alert about relative
energy deficiency in sport
Triagem para RED-S em
corredoras de rua: um alerta para deficiência energética relativa no esporte
Marcos Lira Feitosa da
Silva, João Henrique Gomes, Renata Rebello Mendes
Universidade Federal de
Sergipe, São Cristovão, SE, Brazil
Received: August 22, 2024; Accepted:
October 17,2024.
Correspondence: Renata Rebello Mendes, remendes@academico.ufs.br
How to cite
Silva MLF, Gomes JH, Mendes RR. Screening for RED-S in female street runners: na alert about relative
energy deficiency in sport. Rev Bras
Fisiol Exerc. 2024;23(30:e235602.
doi: 10.33233/rbfex.v23i3.5602
Abstract
Introduction: The Relative Energy Deficiency in Sport (RED-S)
syndrome has become a significant issue for endurance athletes, with low energy
availability (LEA) being its main cause. There is no gold standard for
diagnosis, but in 2023, the 3rd consensus on the subject proposed a new
protocol. Objective: The objective was to evaluate the risk of LEA in
female street runners to screen athletes at risk for RED-S, and to characterize
weekly training volume. Methods: This is a cross-sectional observational
study conducted with 34 female street runners (33.3 ± 5.8 years old, 6.2 years
of training experience, BMI 23.2 ± 2.9), whose LEA risk was assessed by the Low
Energy Availability in Females Questionnaire (LEAF-Q). The cutoff for risk
classification consists of ≥ 8 total score, with emphasis on ≥ 2
score for the injuries subscale, ≥ 2 score for the gastrointestinal
function subscale, and ≥ 4 score for the menstrual function subscale. Results:
The prevalence of LEA risk was 23.5%; among the eight athletes identified at
risk, 75% had high scores above cutoffs for more than one subscale. Menstrual
dysfunction had a score ≥ 4 in 75% of those classified at risk. Although
no significant correlation was found between LEA risk and training volume, the
highest prevalence of risk was identified among athletes with volumes between
41-45 km weekly. Conclusion: The results indicate a high prevalence of
LEA risk among endurance runners, suggesting the importance of screening for
RED-S and the need to continue diagnostic processes in this population.
Keywords: relative
energy deficiency in sport; running; energy intake; menstrual cycle; bone
density; digestive system
Resumo
Introdução: A síndrome de Deficiência de Energia
Relativa no Esporte (RED-S) tornou-se problema relevante para atletas de endurance, sendo a baixa disponibilidade de energia (LEA)
sua principal causa. Não há padrão ouro para diagnóstico, mas em 2023 o 3º
consenso internacional sobre o tema sugeriu novo protocolo. Objetivo:
Objetivou-se avaliar o risco de LEA em corredoras de rua para triar atletas em
risco para RED-S, e caracterizar volume semanal de treinamento. Métodos:
Estudo observacional transversal realizado com 34 mulheres corredoras de rua
(33,3 ± 5,8 anos de idade, 6,2 anos de experiência em treinamento, IMC 23,2 ±
2,9), cujo risco de LEA foi avaliado pelo Low
Energy Availability in Females
Questionnaire (LEAF-Q). O corte para
classificação de risco consiste em ≥ 8 de pontuação total, com destaque
para pontuação ≥ 2 para a subescala de lesões, ≥ 2 para a subescala
de função gastrointestinal, e ≥ 4 para a subescala de função menstrual. Resultados:
A prevalência de risco de LEA foi 23,5%; dentre as oito atletas identificadas
com risco, 75% apresentaram elevadas pontuações para mais de uma subescala. A
disfunção menstrual apresentou pontuação ≥ 4 em 75% das classificadas com
risco. Embora não tenha sido encontrada correlação significativa entre o risco
de LEA e volume e frequência de treinamento, as maiores prevalências de risco
foram identificadas entre atletas com volume semanal entre 41-45 km. Conclusão:
Os resultados indicam elevada prevalência de risco de LEA entre as corredoras
de endurance, sugerindo a importância da triagem para
RED-S e a necessidade de dar continuidade aos processos diagnósticos nessa
população.
Palavras-chave: deficiência de energia relativa no
esporte; corrida; ingestão de energia; ciclo menstrual; densidade óssea;
sistema digestório.
Introduction
The syndrome known as Relative Energy Deficiency in
Sport (RED-S) has been considered a significant problem for endurance athletes, who generally
have a high training volume, high caloric
expenditure, gastrointestinal difficulties
for adequate energy intake during exercise,
need to be
light to achieve better results in competitions and training, and a greater risk
of restrictive eating habits, especially among women [1,2,3,4].
The main etiological factor of this syndrome is low
energy availability (LEA), a situation observed when the daily caloric intake
is not sufficient to satisfy both the demand of physical exercise and the
energy needs of all the physiological systems of the body at rest [5]. For
women, LEA has been suggested as energy availability (energy available only for
extra-workout moments) of less than 30.0 calories per day per kg of lean mass,
and when this situation is maintained for prolonged periods, a decline in sports
performance and clinical complications may occur, such as changes in menstrual
and bone functions, reductions in metabolic rate, immunity and protein
synthesis, and damage to cardiovascular and psychological health, among others
[6,7,8,9].
Understanding the complexity of RED-S, its risk factors,
and complications is essential for implementing effective preventive and
intervention strategies to ensure the health and performance of these athletes,
and the first step is diagnosis [10]. However, diagnosing RED-S is still
challenging for health professionals, as there isn't a gold standard protocol
for this purpose.
Until 2023, studies used very different protocols to
diagnose RED-S and sometimes mistakenly adopted the terms LEA and RED-S as
interchangeable, resulting in prevalences between 23 and 79.5% in women and 15
and 70% in men [3]. However, in September 2023, the 3rd international consensus
on this syndrome was published [8], which proposed a three-stage assessment
model. First, the application of screening questionnaires to detect possible
symptoms of low energy availability; for this stage, one of the recommended
questionnaires for women who exercise is the Low Energy Availability in Females
Questionnaire (LEAF-Q), recently translated and validated into Brazilian
Portuguese [11]. The following steps involve anamnesis and evaluations by a
multidisciplinary team, which may or may not confirm the diagnosis of RED-S
and, if necessary, guide appropriate treatment.
The scarcity of studies that have applied the RED-S
assessment method suggested by the 2023 consensus makes it difficult to compare
and generalize epidemiological data on this syndrome. Therefore, there is an
urgent need for more studies that follow the recommendations of the 2023
consensus to assess the prevalence and impact of RED-S in different sporting
contexts, especially in endurance athletes [6]. Thus, the present study aimed
to evaluate the risk of LEA in female runners of long-distance road races to
screen athletes at risk for RED-S development.
Methods
Experimental design
This observational, cross-sectional, quantitative study
was carried out in three stages [1]. After the approvement of the research
project by the Research Ethics Committee, the first meeting happened virtually;
on this occasion, the aim was to present the objectives and procedures related
to the study to coaches and runners; the terms of free and informed consent
(TCLE) were also presented to the runners, for later reading and signing by
those who met the inclusion criteria and were interested in participating [2].
One week after the initial presentations, interested runners were instructed on
how to fill out the questionnaires, and any possible doubts were clarified [3].
Finally, the LEAF-Q questionnaire was completed online, with questions
necessary to characterize the participants.
Participants
Thirty-four female street runners engaged in training
programs, whose objective was to complete street races longer than 21.1 km
(half marathon), were included. Recruitment was carried out by contacting the
coaches responsible for prescribing running training at the six main running
clubs in the city of Aracaju.
The main inclusion criteria were to currently have or
have had in the last 12 months an average weekly training volume greater than
35 km and to be over 18 years of age. The exclusion criteria were: (a) having
locomotor system diseases capable of increasing the risk of injuries,
regardless of caloric intake; (b) having diseases capable of causing changes in
intestinal rhythm and/or menstrual cycles, regardless of caloric intake; (c)
not having chronic thyroid problems; (d) not being pregnant or lactating.
Assessment instruments
For the evaluation of the participants, the Low Energy
Availability Questionnaire in Women (LEAF-Q) was adopted, consisting of a
self-administered questionnaire originally presented in English (2015) and
recently translated into Portuguese [11]. It consists of items related to
menstrual and gastrointestinal status and the occurrence of injuries, that is,
factors associated with persistent energy deficiency that allow the
identification of the risk of low energy availability when the score is ≥
8.0. Additionally, partial cutoff points can be adopted; as follows: ≥
2.0 for the section on questions about injuries; ≥ 2.0 for the section on
gastrointestinal changes; ≥ 4.0 for the section on menstrual function.
According to Logue et al. [3], the LEAF-Q is an
easy-to-administer instrument, validated for use in endurance-trained women to
investigate the risk of LEA, alleviating some of the challenges associated with
the direct measurement of energy availability, as well as being considered an
adequate screening tool for RED-S among young female athletes [12].
Finally, a semi-structured questionnaire was developed to
characterize the participants regarding their training routine, experience in
the sport, age, and anthropometry.
Statistical analysis
Descriptive statistics were used, with some data
presented as mean, standard deviation, minimum, and maximum, and others as
absolute and relative frequency. To test possible correlations between
variables, data normality and homogeneity were initially tested using the
Shapiro-Wilk and Levene tests, respectively. Depending on the results, Spearman
or Friedman correlation tests were used for nonparametric and parametric data,
respectively. All analyses were performed using SPSS-22.0 software (IBM, SPSS
Inc., Chicago, IL, USA). Significance was set at p < 0.05.
Results
Table I – Characterization of participants regarding age,
anthropometry, weekly frequency of running training, and weekly training volume
(n = 34)
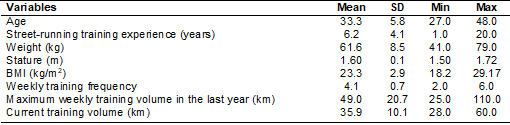
Table II shows that most participants are training
volumes between 25 and 30 km per week, followed by volumes between 31 and 35
km, and those who train between 46-50 km.
Table II - Distribution of participants according to current
weekly running training volume
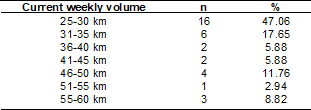
Table III - Total and subscale scores that make up the LEAF-Q
(n = 34)

Figure 1 demonstrates a predominance of runners without
risk of LEA; however, among those screened with risk of LEA (LEAF-Q with a
total score equal to or higher than 8 points - Figure 2), it is noted that most
of the runners presented high scores (higher than the cut-off scores) for more
than one LEAF-Q subscale, with a predominance of menstrual dysfunctions.
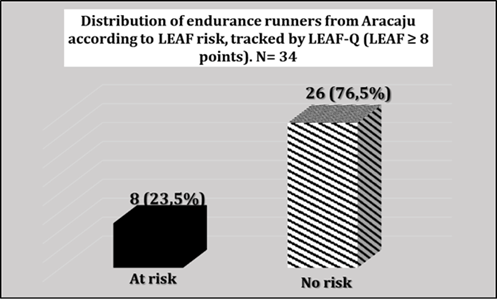
Figure 1 - Distribution of endurance runners from Aracaju
according to LEA risk, tracked by LEAF-Q. N = 34
Col 1: Runners with scores above the LEA risk score on
all scales (menstrual function ≥ 4 points; injuries ≥ 2 points; and
gastrointestinal function ≥ 2 points).
Col 2:Runners with scores above the LEA risk score for
two subscales: (menstrual function ≥ 4 points; injuries ≥ 2
points).
Col 3: Runners with scores above the LEA risk score only
for the menstrual function subscale (≥ 4 points).
Col 4: Runners with scores above the LEA risk score only
for the injury subscale (≥ 2 points).
Col 5: Runners with scores above the LEA risk score for
two subscales (gastrointestinal function ≥ 2 points; injuries ≥ 2
points).
I = Injury subscale; MF = Menstrual function subscale; GF
= Gastrointestinal function subscale
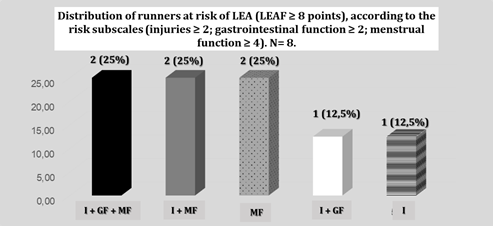
Figure 2 - Distribution of runners at risk of LEA (LEAF ≥
8 points), according to the risk subscales (injuries ≥ 2;
Gastrointestinal function ≥ 2; Menstrual function ≥
4). N = 8
Figure 2 shows that among the participants screened for
LEA risk (LEAF-Q with a total score equal to or greater than 8 points), the
majority presented scores higher than the risk score for more than one
subscale, and menstrual dysfunction appears prominently among 75% of
participants at risk for LEA.
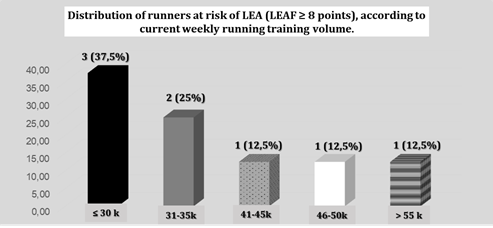
Figure 3 - Distribution of runners at risk of LEA (LEAF ≥
8 points), according to the current weekly running training volume
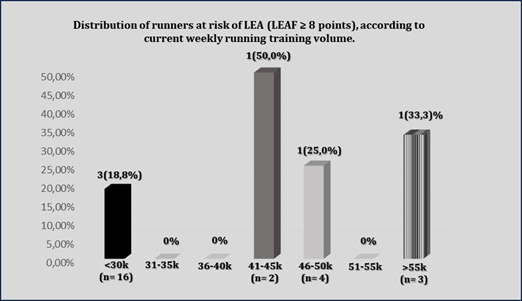
Figure 4 - Prevalence of LEA risk (LEAF-Q ≥ 8
points) in each category of runners, considering the current weekly training
volume
Figure 3 shows that among the participants screened for
LEA risk (LEAF-Q with a total score equal to or higher than 8 points), the
majority were subjected to a running training volume less than or equal to 30
km per week, followed by athletes with a volume between 31 and 35 km per week.
However, Figure 4 shows that, when correcting the frequency of athletes with
LEA risk according to the number of participants in each category of weekly
training volume, it is noted that the emphasis is on athletes with volumes
between 41 and 45 km and greater than 55 km.
Correlations
After thoroughly analyzing all
variables, no correlation was found between them in this study. However, it is
worth noting that even without any correlations being observed, this does not
necessarily rule out the possibility of relationships between the variables but
only that it was not possible to identify statistically significant
associations between them. Therefore, it is suggested that future research in
this regard is necessary.
Discussion
This study aimed to evaluate the risk of LEA in female
endurance runners as a way of screening for risk and RED-S, as well as to
describe the weekly training volume and test the correlation between these
variables. The main findings were that 23.5% of the participants were at risk
for LEA, according to the total LEAF-Q score, with an average of 6.06 total
points. The menstrual dysfunction subscales stood out, and there was a higher
frequency of LEA risk for those who had a weekly running volume between 41 and
45 km. However, there was no statistically significant correlation between the
risk of LEA and training volume. Regarding the prevalence of LEA risk through
the LEAF-Q instrument, it is possible to observe similarity with the data
mentioned in the 3rd RED-S consensus, which reports a risk of LEA and RED-S
between 23% and 79.5% in female athletes. However, the biggest criticism
mentioned in this consensus is precisely the fact that the terms LEA and RED-S
are used as if they refer to the same phenomenon, which is not true. Not all
athletes with low energy availability will develop relative energy deficiency
syndrome in sports, with its characteristic symptoms in performance and/or
health [8]. Adopting a common analogy in the area of nutrition, it can be said
that LEA is for iron deficiency, just as RED-S would be for iron deficiency
anemia; that is, not every athlete with iron deficiency will develop iron
deficiency anemia, just as not every athlete at risk of LEA will develop RED-S.
In fact, in the last consensus on RED-S, the term adaptive LEA was adopted for
the first time, with benign effects and mild and rapidly reversible changes in
biomarkers of several body systems, but which, if maintained chronically, could
become a problematic LEA, culminating in RED-S [8].
For these reasons, it is essential that the prevalence of
LEA found in the present study, using the LEAF-Q, be compared to data obtained
using the same instrument. Therefore, in our searches, we found some recent
studies that used the same instrument to verify the risk of LEA [12,13,14,15,16,17,18,19,20,21], but
few were conducted with endurance runners [15,18,21], which makes the
contribution of the present study explicit.
Black et al. [22] evaluated 38 female recreational
athletes (mean age 22 years) who performed between 2.5 and 5 hours of
moderate-intensity exercise per week, or 1.25 to 2.5 hours of vigorous exercise
per week, or an equivalent combination of both types of exercise, regardless of
the modality. The authors found a prevalence of LEA risk of 63.2%, with a mean
of 8.9 points on the LEAF-Q. Civil et al. [14] also found a high
prevalence of LEA risk (65% with LEAF-Q ≥ 8) when evaluating 20 students
in professional ballet training in Scotland, which is an aesthetic modality
and, therefore, with a bigger concern related to thinness and dietary
restriction. With similar results, Łuszczki et al. [12] found
a prevalence of 64.7% of LEA risk in adolescent soccer players; this age group
also being considered at high risk for LEA and RED-S [23].
Meng et al. [16] evaluated women in aesthetic
modalities, comparing elite athletes (n = 52) with recreational athletes (n =
113), and found a prevalence of LEA risk (LEAF-Q ≥ 8) of 55.8% and 35.1%,
respectively. Similar results were found by Slater et al. [17], who
evaluated 109 women who practiced recreational exercises in gyms and fitness
spaces and found a 45% prevalence of LEA risk through the LEAF-Q.
Among the studies carried out with running and LEAF-Q,
Kyte et al. [21] evaluated amateur endurance runners and obtained a
prevalence of 44.0% of LEA risk through LEAF-Q, while Dambacher et al.
[16] found 54.5% in a study carried out with 156 of the same type of athlete.
Among elite runners, Heikura et al. [15] found that among those who
presented energy availability between 30 and 45 kcal/kg MMg, the average LEAF-Q
was 9.04 points, and in those with low energy availability (< 30 kcal/kg
MMg), 11.04. However, the authors did not report the prevalence of LEA risk
based on this instrument.
Although the risk in our study (23.5%) is relatively
lower than the risks observed in the studies described above, it is important
to highlight that the prevalence of LEA risk found in our study is still
considered high, according to Mountjoy et al. [8], since practically a
quarter of the sample studied has a chance of developing RED-S, which can
culminate in serious health problems and performance impairments.
In the same sense, although our average total LEAF-Q
score (6.06) was lower than that of the study by Heikura et al. [15]
(between 9.04 and 11.04), probably due to the difference in training level
[18], it is essential to highlight that the athletes we identified as at risk
should be referred to the next stages of evaluation, to investigate possible
clinical symptoms of RED-S and the need for treatment [20].
Concerning training volume, the study by Meng et al.
[16] showed that elite Chinese athletes with higher training volumes and
frequencies than amateur athletes had a higher risk of developing LEA with
menstrual and bone disorders. Slater et al. [17] also found that for
each extra hour of weekly exercise practiced by recreational athletes, there
was a 1.13-fold increase in the risk of LEA. However, in the present study, no
correlations were found between training volume and frequency and the risk of
LEA. The absence of this correlation in the present study may be related to two
possible factors: a) regardless of the training volume, the energy intake of
athletes at risk of LEA should be evaluated because even if the training volume
is reduced, if the energy availability is very low, menstrual and
gastrointestinal symptoms and the emergence of injuries may occur; that is, it
is not only how much you train that matters, but also how you replace the
energy expended over the 24 hours; b) reduced sample in the categories with the
highest weekly volume (in the present study), demonstrating the relevance of
future research involving larger groups, with different training volumes and
frequencies.
The presence of menstrual dysfunction in most
participants in this study corroborates many studies that evaluate LEA, since
the time when the female athlete triad was evaluated [8]. According to Mendes et
al. [5], the menstrual disorder related to LEA is based on the relationship
between the insufficient arrival of metabolic fuels to meet the needs of the
brain and the interruption of the pulsatility of the gonadotropin-releasing
hormone (GnRH) in the hypothalamus. Consequently, there are changes in the
release of luteinizing hormone (LH) and follicle-stimulating hormone (FSH) by
the pituitary gland and a drop in blood concentrations of estradiol and
progesterone [22]. Such changes can culminate in subclinical menstrual
disorders (anovulatory cycles) up to long menstrual cycles and
primary/secondary amenorrhea (functional hypothalamic amenorrhea).
The lesions scored in the LEAF-Q, especially the bone
ones, as observed in the present study, have been justified by a decrease in
bone mineral density caused by multifactorial conditions related to LEA, such
as hypoestrogenism, decrease in blood concentrations of leptin, insulin,
insulin-like growth factor 1 (IGF-1), and increased cortisol. Such factors are
associated with reduced osteoblast activity and reduced synthesis of type I
collagen, culminating in bone demineralization and increased risk of stress
fractures [5,24].
With regard to changes in gastrointestinal function, also
scored in the present study, it is possible to report that LEA is usually
accompanied by insufficient iron intake, as well as training sessions capable
of promoting an increase in interleukin-6 and hepcidin, culminating in reduced
intestinal iron absorption. Given the lower bioavailability of iron, it is
possible that there will be less synthesis of thyroxine and a decrease in its
conversion to triiodothyronine, thus increasing the risk of developing
hypothyroidism, which in turn can cause changes in intestinal rhythm [5,25].
After the diagnosis of LEA risk (LEAF-Q score ≥ 8),
the recommended referral is a comprehensive and holistic multidisciplinary
approach to investigate possible cases of RED-S, categorize severity, and, if
necessary, define treatment strategies [8].
It is worth noting that the continuity of the diagnostic
process, in addition to screening via LEAF-Q, is essential, as this is a
complex syndrome that can become serious. In addition to the injuries and
menstrual and gastrointestinal dysfunctions addressed in LEAF-Q, other changes
are also observed in athletes diagnosed with RED-S, such as changes in glucose
and lipid metabolism, impairment of cardiovascular and endothelial function,
impairment of the immune system, impairment of sleep quality and general well-being.
From a mental point of view, some women have difficulty motivating themselves,
as well as developing anxiety, addiction or dependence on training, and
depression [6]. Thus, the consequences of RED-S syndrome are devastating,
serious, and even fatal, ranging from an unwillingness to train to extreme
complications, such as suicide [8]. The most reported consequences of athletic
performance are decreased response to training, loss of strength, reduced
recovery capacity, and a general impairment in endurance events and exercises
[8].
Therefore, according to Witkoś et al. [20],
carrying out screening processes for RED-S may represent a fundamental strategy
for identifying and treating this syndrome to avoid extreme complications,
improving not only the athletic performance of this athlete but also her
quality of life.
Conclusion
A high prevalence of LEA risk was found among endurance
runners (23.5%), with a predominance of menstrual dysfunctions (75%) among
athletes at risk and a higher relative prevalence among runners with a weekly
training volume between 41 and 55 km, demonstrating the need to continue the
diagnostic processes for RED-S in this population.
Conflicts of interest
There are no conflicts of interest
Sources of funding
There was no funding
Authors' contributions
Conception and design of the research: Silva MLF, Gomes JH, Mendes RR; Data collection: Silva MLF, Mendes
RR; Data analysis and interpretation: Silva MLF, Mendes RR; Statistical
analysis: Gomes JH; Manuscript writing: Silva MLF, Mendes RR; Critical
revision of the manuscript for important intellectual content: Silva MLF,
Gomes JH, Mendes RR
References
- Drew M, Vlahovich N, Hughes D, Appaneal R, Burke LM, Lundy B, et al.
Prevalence of illness, poor mental health and sleep quality and low energy
availability prior to the 2016 Summer Olympic Games. Br J Sports Med.
2018;52(1):47-53. doi: 10.1136/bjsports-2017-098208 [Crossref]
- Hackney AC, Zieff GH, Lane AR, Register-Mihalik JK. Marathon running and sexual libido in adult men: exercise training and racing effects. J Endocrinol Sci. 2022;4(1):10-12. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC9442612/pdf/nihms-1832624.pdf
- Logue DM, Madigan SM, Melin A, Delahunt E, Heinen M, Donnell SM, Corish CA. Low energy availability in athletes 2020: an updated narrative review of prevalence, risk, within-day energy balance, knowledge, and impact on sports performance. Nutrients. 2020;12(3):835. doi: 10.3390/nu12030835 [Crossref]
- Melin AK, Areta JL, Heikura IA, Stellingwerff T, Torstveit MK, Hackney AC.
Direct and indirect impact of low energy availability on sports performance.
Scand J Med Sci Sports. 2024;34(1):e14327. doi: 10.1111/sms.14327 [Crossref]
- Mendes RR, Bevilacqua M, Rossi L. Relative Energy Deficiency in Sport
(RED-S). Capítulo 48. In:
Tratado de Nutrição e Dietoterapia. 2a ed. Rio de Janeiro: Guanabara Koogan:
2023. p.1-3.
- Langbein RK, Martin D, Allen-Collinson J, Crust L, Jackman PC. "I'd
got self-destruction down to a fine art": a qualitative exploration of
relative energy deficiency in sport (RED-S) in endurance athletes. J Sports
Sci. 2021;39(14):1555-64. doi: 10.1080/02640414.2021.1883312 [Crossref]
- Mountjoy M, Sundgot-Borgen JK, Burke LM, Ackerman KE, Blauwet C, Constantini N, et al. IOC consensus statement on relative energy deficiency in sport (RED-S): 2018 update. Br J Sports Med. 2018;52(11):687-97. doi: 10.1136/bjsports-2018-099193 [Crossref]
- Mountjoy M, Ackerman KE, Bailey DM, Burke LM, Constantini N, Hackney AC, et
al. 2023 International Olympic Committee's (IOC) consensus statement on
Relative Energy Deficiency in Sport (REDs). Br J Sports Med.
2023;57(17):1073-97. doi: 10.1136/bjsports-2023-106994. Erratum in: Br J Sports
Med. 2024; 58(3):e4. doi: 10.1136/bjsports-2023-106994corr1 [Crossref]
- Stellingwerff T, Heikura
IA, Meeusen R, Bermon S, Seiler S, Mountjoy ML, Burke LM. Overtraining
Syndrome (OTS) and Relative Energy Deficiency in Sport (RED-S): shared
pathways, symptoms and complexities. Sports Med. 2021;51(11):2251-80. doi: 10.1007/s40279-021-01491-0 [Crossref]
- Nattiv A, Souza MJ, Koltun KJ, Misra M, Kussman A, Williams NI, et al. The Male Athlete Triad-A Consensus Statement From the Female and Male Athlete Triad Coalition Part 1: definition and scientific basis. Clin J Sport Med. 2021;31(4):335-48. doi: 10.1097/JSM.0000000000000946 [Crossref]
- Maria UM, Juzwiak CR. Cultural adaptation and validation of the low energy
availability in females questionnaire (LEAF-Q). Rev Bras Med Esporte. 2021;27(2):184-8. doi: 10.1590/1517-869220212702223889 [Crossref]
- Łuszczki E, Jagielski P, Bartosiewicz A, Kuchciak
M, Dereń K,
Stolarczyk A, Pakosz P, et
al. The LEAF questionnaire is a good screening tool for the identification of
the Female Athlete Triad/Relative Energy Deficiency in Sport among young
football players. Peer J. 2021;3;9:e12118. doi: 10.7717/peerj.12118 [Crossref]
- Black K, Slater J, Brown RC, Cooke R. Low energy availability, plasma
lipids, and hormonal profiles of recreational athletes. J Strength Cond Res.
2018;32(10):2816-24. doi: 10.1519/JSC.0000000000002540 [Crossref]
- Civil R, Lamb A, Loosmore D, Ross L, Livingstone K, Strachan F, et al.
Assessment of dietary intake, energy status, and factors associated with RED-S
in vocational female ballet students. Front Nutr. 2019;9(5):136. doi: 10.3389/fnut.2018.00136 [Crossref]
- Heikura IA, Uusitalo ALT, Stellingwerff T, Bergland D, Mero AA, Burke LM.
Low energy availability is difficult to assess but outcomes have large impact
on bone injury rates in elite distance athletes. Int J Sport Nutr Exerc Metab.
2018;28(4):403-11. doi: 10.1123/ijsnem.2017-0313 [Crossref]
- Meng K, Qiu J, Benardot D, Carr A, Yi L, Wang J, Liang Y. The risk of low energy availability in Chinese elite and recreational female aesthetic sports athletes. J Int Soc Sports Nutr. 2020;17(1):13. doi: 10.1186/s12970-020-00344-x [Crossref]
- Slater J, McLay-Cooke R, Brown R, Black K. Female recreational exercisers
at risk for low energy availability. Int J Sport Nutr Exerc Metab. 2016;
26(5):421-7. doi: 10.1123/ijsnem.2015-0245 [Crossref]
- Dambacher L, Pritchett K, Pritchett R, Larson A. Risk of low energy
availability, disordered eating, and menstrual dysfunction in female collegiate
runners. J Athl Train. 2023. doi: 10.4085/1062-6050-0454.23 [Crossref]
- Jesus F, Castela I, Silva AM, Branco PA, Sousa M. Risk of low energy availability among female and male elite runners competing at the 26th European Cross-Country Championships. Nutrients. 2021;13(3):873. doi: 10.3390/nu13030873 [Crossref]
- Witkoś J, Błażejewski G, Gierach M. An Assessment of the early symptoms of energy deficiency as a female athlete triad risk among the polish national kayaking team using LEAF-Q. Int J Environ Res Public Health. 2022;19(10):5965. doi: 10.3390/ijerph19105965 [Crossref]
- Kyte KH, Stensrud T, Berg TJ, Seljeflot I, Hisdal J. Vascular function in
norwegian female elite runners: a cross-sectional, controlled study. Sports
(Basel). 2022;10(3):37. doi: 10.3390/sports10030037 [Crossref]
- Souza MJ, Koltun KJ, Williams NI. The role of energy availability in
reproductive function in the female athlete triad and extension of its effects
to men: an initial working model of a similar syndrome in male athletes. Sports
Med. 2019;49(Suppl 2):125-37. doi: 10.1007/s40279-019-01217-3 [Crossref]
- Gould RJ, Ridout AJ, Newton JL. Relative Energy Deficiency in Sport (RED-S)
in Adolescents - A Practical Review. Int J Sports Med. 2023;44(4):236-46. doi: 10.1055/a-1947-3174 [Crossref]
- Southmayd EA, Mallinson RJ, Williams NI, Mallinson DJ, De Souza MJ. Unique effects of energy versus estrogen deficiency on multiple components of bone strength in exercising women. Osteoporos Int. 201728(4):1365-76. doi: 10.1007/s00198-016-3887-x [Crossref]
- McKay AKA, Peeling P, Pyne DB, Tee N, Whitfield J, Sharma AP, Heikura IA, Burke LM. Six days of low carbohydrate, not energy availability, alters the iron and immune response to exercise in elite athletes. Med Sci Sports Exerc. 2022;54(3):377-87. doi: 10.1249/MSS.0000000000002819 [Crossref]
