Rev
Bras Fisiol Exerc. 2025;24:e245616
doi: 10.33233/rbfex.v24i1.5616
ORIGINAL
ARTICLE
Is
self-perception enough to predict cardiorespiratory fitness?
A autopercepção é suficiente para
predizer a aptidão cardiorrespiratória?
Vinicius
de Oliveira Damasceno, Laura Cabral Cruz Lopes da Silveira, Gustavo Bernardes Fanaro, Helder Guerra de Resende, Paula Morisco
de Sá
Universidade
da Força Aérea – UNIFA, Rio de Janeiro, RJ, Brazil
Received: December 16, 2024; Accepted: January 2, 2025.
Correspondence: Vinicius de Oliveira
Damasceno, viniciusvod@fab.mil.br
How to cite
Damasceno VO, Silveira LCCL, Fanaro GB, Resende
HG, Sá PM. Is self-perception enough to predict cardiorespiratory fitness? Rev Bras Fisiol
Exerc. 2025;24(2):e245616. doi:
10.33233/rbfex.v24i1.5616
Abstract
Introduction: This study investigated the validity of
self-perceived cardiorespiratory fitness as a tool for assessing physical
fitness in military personnel of the Brazilian Air Force. Objectives: The
objective was to determine the correlation between self-reported fitness and
objectively measured VO2max, exploring its potential as an
alternative or complement to traditional methods. Methods: The study
employed a cross-sectional design, using a convenience sample of 72 aspirants
to the officer cadre of the Brazilian Air Force (47 females, 25 males). Data
were collected using a self-report questionnaire to assess perceived
cardiorespiratory fitness and a 12-minute Cooper run test to measure V̇O2max.
Statistical analyses included descriptive statistics, t-tests, ANOVA,
correlation analysis, and k-means clustering. Results: The results
showed a significant positive correlation between self-reported fitness and VO2max,
suggesting that self-report and objective measures are in reasonably good
agreement. However, the analyses revealed some discrepancies, with potential
biases in self-report observed at different fitness levels and between genders.
Although self-report showed promise as a complementary tool, it was not a
perfect substitute for objective assessment. Conclusion: The study
concluded that self-perceived cardiorespiratory fitness has potential as a
large-scale, cost-effective screening tool for the Brazilian Air Force.
Keywords: surveys and questionnaires; physical fitness;
cross-sectional studies; exercise test; military personnel
Resumo
Introdução: Este estudo investigou a validade da
aptidão cardiorrespiratória autopercebida como uma ferramenta para avaliar a
aptidão física de militares da Força Aérea Brasileira. Objetivos: O
objetivo foi determinar a correlação entre aptidão autorrelatada e VO2máx
medido objetivamente, explorando seu potencial como uma alternativa ou
complemento aos métodos tradicionais. Métodos: O estudo empregou um
delineamento transversal, utilizando uma amostra de conveniência de 72 Aspirantes
ao Quadro de Oficiais da Força Aérea Brasileira (47 mulheres, 25 homens). Os
dados foram coletados usando um questionário de autorrelato que avaliou a
aptidão cardiorrespiratória percebida e um teste de corrida de Cooper de 12
minutos para medir o V̇O2máx. As análises estatísticas
incluíram estatísticas descritivas, testes t, ANOVA, análise de correlação e
agrupamento de k-means. Resultados: Os
resultados demonstraram uma correlação positiva significativa entre aptidão
autorrelatada e VO2máx, sugerindo que a autopercepção se alinha
razoavelmente bem com medições objetivas. No entanto, as análises revelaram
algumas discrepâncias, com potenciais vieses observados na autoavaliação em
diferentes níveis de aptidão e entre gêneros. Embora a autopercepção tenha se
mostrado promissora como uma ferramenta complementar, ela não foi um substituto
perfeito para a avaliação objetiva. Conclusão: O estudo concluiu que a
aptidão cardiorrespiratória autopercebida tem potencial como uma ferramenta de
triagem de grande escala e custo-benefício para a Força Aérea Brasileira,
complementando, mas não substituindo totalmente, os métodos de avaliação
direta. Pesquisas adicionais com amostras maiores e mais diversas são
necessárias.
Palavras-chave: inquéritos
e questionários; aptidão física; estudos transversais; teste de exercício;
militares.
Introduction
Cardiorespiratory fitness "is
the capacity to execute dynamic exercises involving large muscle groups at
moderate to high intensity for prolonged durations" [1], with maximal
oxygen uptake (V̇O2max) serving as the most valid and
extensively accepted measure representing the capacity of the cardiorespiratory
system [2].
Traditionally, to obtain V̇O2max,
the scientific and professional community in the health area uses tests
classified as direct, indirect, and effortless methods [2,3]. Direct evaluation
methods involve using an ergometer (treadmill, bicycle, among others) and a gas
analyzer capable of quantifying in real-time, breath by breath, the amount of
oxygen metabolized during the test [1,4]. Generally, these methods involve
gradually increasing the intensity of the exercise (speed and/or incline) until
the volunteer is exhausted [2,3,4].
Indirect methods can be performed
using ergometers or in the field, but generally at submaximal intensities [2].
These methods use the heart rate (HR) response to a submaximal intensity [5]
(e.g. Åstrand test) or, in some cases, the distance
traveled in a unit of time in equations that predict V̇O2max [1,2]
(e.g. 1-mile test). The indirect method is related to using V̇O2max
prediction equations without subjecting the individual to exercise [1,2].
Although direct assessment methods
are considered more valid and reliable for obtaining V̇O2max,
indirect methods offer advantages such as lower cost (acquisition and
maintenance of equipment), greater practicality, and less need for trained
personnel to operate equipment [6], in addition to allowing large-scale
assessments.
Another method with potential for
estimating general physical fitness (cardiorespiratory fitness, strength,
localized muscular endurance, flexibility, and body composition) is the
measurement of self-perception. In practice, self-perception consists of asking
the individual to declare how he or she perceives his or her general physical
fitness. There are different approaches to measuring general physical fitness
based on self-reports. Some use a single general question [7,8], such as
"How do you perceive your general physical fitness?". Other
approaches use several questions separated by component (cardiorespiratory
fitness, strength, localized muscular endurance, flexibility, and body
composition) [9,10].
The
Brazilian Armed Forces conduct periodic physical fitness assessments of their
military personnel to ensure health and adequate professional and operational
performance [11,12,13]. Applying these assessments requires distinct planning and
logistics, considering the different infrastructure realities (facilities and
equipment) among the military organizations distributed throughout the
Brazilian territory.
This diversity of situations
demands flexibility and adaptations in implementing physical assessment
programs, ensuring that all military personnel can be assessed effectively and
consistently, regardless of location and existing conditions. In particular, in
the Brazilian Air Force, the Physical Fitness Assessment Test [11] is carried
out twice a year, involving two stages. The PAR-Q Questionnaire is completed,
the resting heart rate, body mass, height, and waist circumference are measured
in the first stage. In the second stage, the military personnel perform the
Ground Push-Up Test, Abdominal Test, and the 12-minute Run. In other words,
carrying out these tests requires time and the presence of a large number of
specialized professionals to meet the needs of all military organizations [14].
Aandastad [6] highlights that self-perception instruments are
practical and economical tools for collecting data on physical fitness in large
groups. These instruments are particularly useful in population surveys, health
assessments, and selection processes for demanding physical activities, as in
the Armed Forces.
Considering this scenario,
self-perception of cardiorespiratory fitness emerges as a promising
alternative. Rather than relying exclusively on a standardized physical test,
it would be possible to use the assessment that military personnel themselves
make of this component of physical fitness. Since military personnel are
familiar with the criteria for passing physical tests, they may have a more appropriated
perception of their cardiorespiratory capacity. This hypothesis suggests that
self-perception could complement traditional tests, optimizing the evaluation
process and allowing military personnel to dedicate more time to their support
or operational duties. Given the above, the objective of this study was to
evaluate the feasibility and accuracy of self-perception of cardiorespiratory
fitness as an alternative or complement to direct testing in military
personnel.
Methods
Type and design of the study
According to Thomas, Nelson & Silverman [15] this
is an observational study with a cross-sectional design.
Sample
This study was conducted with a group of
Aspirants to the temporary officer cadre of the FAB who were completing the
Technical Adaptation Internship (EAT) at the Guarnição
de Aeronáutica dos Afonsos
(GUARNAE-AF) in the first half of 2024. The sample group comprised 72 military
personnel of both sexes (47 women and 25 men). All individuals who voluntarily
agreed to participate in the research participated. At the same time, those who
did not fill out the form or did not take the physical fitness test were excluded.
Procedures and instruments
In the first stage, the Candidates were
gathered to answer a questionnaire about their self-perception of
cardiorespiratory fitness. After presenting the research and signing the free
and informed consent form, the participants answered, "How do you perceive
your cardiorespiratory fitness?". The answers were recorded on a 5-point
Likert scale, ranging from "very bad" to "very good". For
analysis purposes, the option "very good" was considered 100%, and
the other options were proportionally adjusted.
In the second stage, 24 and 48 hours
after the first stage, the Aspirants performed the 12-minute Cooper test on the
official GUARNAE-AF athletics track. In this test, participants ran the longest
distance possible in 12 minutes, maintaining a constant speed. With two minutes
remaining, the Aspirants were notified that the time was nearing the end. At
the end of the test, the Aspirants remained on the spot, and the distance
covered was recorded.
To convert the distance into V̇O2max the following equation [16] was used:
Statistical analysis
Data analysis involved the application
of descriptive and inferential statistics. Student's t-test and Cohen's effect
size calculation were used to compare demographic characteristics between
genders. The relationship between self-perception of cardiorespiratory fitness
and V̇O2max was investigated using Pearson's correlation coefficient.
For analysis purposes, the "very good" option was considered 100%
(1.0), and the other options were proportionally adjusted using a simple rule
of three.
To verify whether there were significant
differences in the mean values of V̇O2max between the different categories of self-perception, a
one-way ANOVA with Scheffé's post hoc test was
performed. The simple agreement measure assessed the agreement between
self-perception and the categories generated by the k-means method. The
criteria proposed by Mukaka [18] and Cohen [19], respectively, were adopted to
interpret the magnitude of Pearson's correlation and Cohen's effect size.
All statistical analyses were performed
using JASP (JASP Team. 2024. ver. 0.19.3) and Knime
software (Bertold et al. [20]), while
graphs were constructed using GraphPad Prism 9.0 (GraphPad Software, San Diego,
CA). A significance level of 5% (p < 0.05) was considered for all
statistical tests.
Ethics committee
This study was submitted to the Galeão Air Force Hospital Research Ethics Committee and
approved under Protocol No. 2.486.972.
Results
Table I shows the general
characteristics of the sample. All the variables showed homogeneous values
except for VO2max.
Table I - Sample characteristics (n = 72)

BMI
= body mass index
Table II shows the characteristics
stratified by gender. Significant mean differences were observed between men
and women for the variables body mass, height, and V̇O2max, according
to the t-test, with the effect size considered high for body mass, height, and V̇O2max.
Table II - Sample characteristics stratified by gender
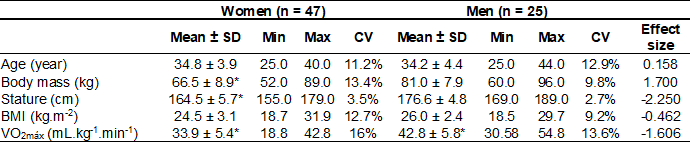
*significant difference between
groups; p < 0.05
Figure 1 shows the correlations between V̇O2max
and self-perceived cardiorespiratory fitness for both sexes (Figure 1a) and
stratified by sex (Figure 1b and 1c). Significant values were found for all
correlations. For the overall relationship, the correlation values were
considered high (r = 0.717; p < 0.001) (Figure 1a) and moderate for women (r
= 0.690, p < 0.001) (Figure 1b) and men (r = 0.573; p < 0.05) (Figure
1c).
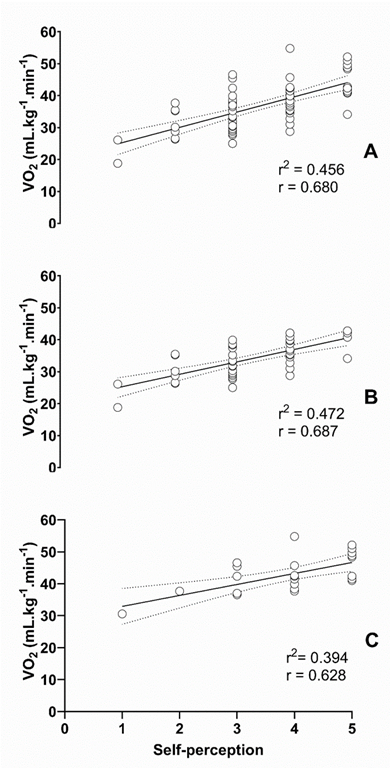
Figure
1 - Correlation between V̇O2MAX and
self-perceived cardiorespiratory fitness, total sample (a), female (b), male
(c)
Figure 2 shows the mean V̇O2max
values grouped by categories of self-perceived cardiorespiratory fitness. In
Figure 2a, no significant differences were found between groups 2 and 3. In
Figure 2b, a significant difference was found between groups 3 and 4, while in
Figure 2c, no significant differences were found between groups 4 and 5.
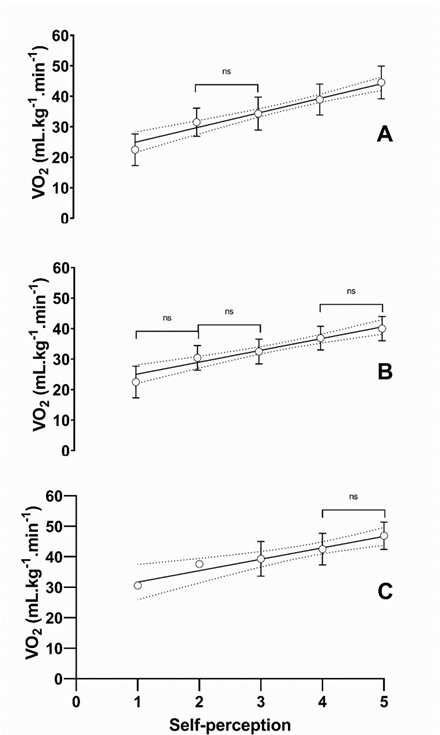
Figura 2 - Mean V̇O2max values grouped by categories of self-perceived
cardiorespiratory fitness, general (a), female
(b), male (c)
Figure 3 shows the distribution of V̇O2max
values grouped by self-perceived cardiorespiratory fitness. In Figure 3a
(female), the group that rated themselves as "excellent" had the
highest V̇O2max values, confirming the classification proposed
by Heardy and Caixeta [17]. On the other hand, the other groups showed a
distribution of values that exceeded the limits established for the
classification of V̇O2max. In Figure 3b (males), all groups
showed distributions that exceeded the limits proposed for the classification
of V̇O2max.
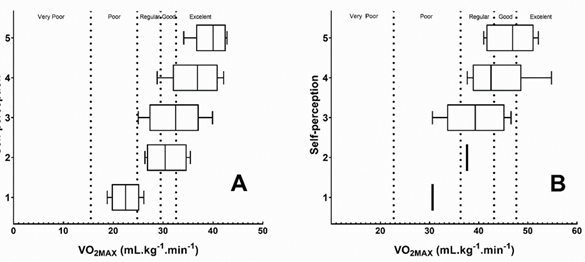
Figure
3 - Distribution of V̇O2max values grouped
by self-perception and classified according to Heardy; Caixeta [17], female (a)
and male (b)
Figure 4 shows the dispersion between
cluster classification and self-perceived cardiorespiratory fitness, separately
for women (Figure 4a) and men (Figure 4b). In both groups, approximately half
of the aspirants (≈53% of women and 44% of men) showed agreement between
the two assessments. Women tended to overestimate their cardiorespiratory
fitness in clusters 2 and 4, whereas men tended to overestimate in cluster 1
and underestimate in clusters 3 and 4.
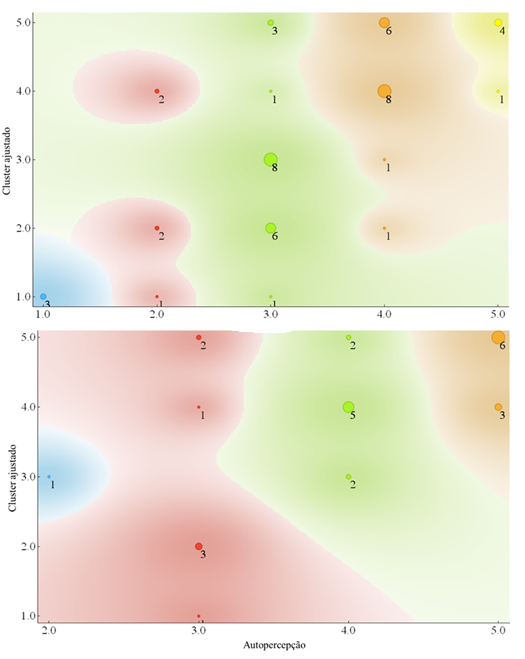
Figure 4 - Scatter
plot between adjusted cluster and self-perception, female (a) and male (b)
Discussion
The main
objective of this study was to analyze the validity of self-perception of
cardiorespiratory fitness as a measurement instrument in a sample of candidates
for the Temporary Officers' Cadre of the Brazilian Air Force. To this end, a
comparison was made between the self-perception data and an objective indicator
of cardiorespiratory fitness, being, to date, the first study to explore this
relationship in this specific context.
This research showed positive and
significant correlations between self-perception of cardiorespiratory fitness
and V̇O2max in a sample of Military Candidates. Specifically, a
moderate correlation was observed between these variables in both the female
and male groups. These findings suggest that the participants demonstrated
considerable coherence in the self-assessment of their cardiorespiratory
capacity since the increase in V̇O2max was related to the elevation of the individual
perception of physical fitness (Figure 1). It is important to highlight that
the scientific literature presents few studies that investigated the relationship
between objective and subjective measures of cardiorespiratory fitness, with
emphasis on the works of Aandstad [6], Petersen et al. [7], Martin et al.
[21] and Knapik et al. [22].
Of the five studies identified in the
literature, only the study by Petersen et
al. [7] has a similar methodology but with some important differences. This
study [7] included a sample with a wide age range (18 to 85 years) and used a
general question about general physical fitness, whereas the present study
focused specifically on self-perceived cardiorespiratory fitness. Participants
(n = 3,441) answered a question about their self-rated physical fitness on a
five-point Likert scale, and objective physical fitness was assessed using a
submaximal test on a bicycle ergometer. Comparing the results, the correlation
coefficients between self-rated and objective cardiorespiratory fitness were
higher in this study for both women (r = -0.52 vs. r = 0.69) and men (r = -0.52
vs. r = 0.57). This discrepancy may be due to differences in sample
characteristics, measurement devices, and cultural issues.
Studies
conducted with non-military populations but with an age range similar to that
of the sample in this study, such as those by Petersen et al. [7], Obling et al.
[23], Jensen et al. [24], and Jones et al. [25] also presented correlation
coefficients similar to those found in the present study. These results support
that self-perceived physical fitness is moderately related to objective
physical fitness in different populations.
In
comparison, the method used in the studies by Aandstad [6], Martin et al. [20], and Jones et al. [25] differs somewhat from the
current one. Although all studies aimed to compare objective and subjective
measures of cardiorespiratory fitness in military personnel, the way subjective
data were collected differed. While the present study used Likert-type scales,
the aforementioned studies asked participants to report their fitness test
results in a quantitative manner, such as the exact time in minutes for the
3-mile test.
Aandstad
[6] assessed 14,166 Norwegian military personnel using a 3,000-meter running
test and then asked the participants to estimate online the time they would be
able to complete the same test. The results showed a strong negative
correlation between self-perception and actual performance on the running test,
with correlation coefficients similar to those found in the present study for
the total group (r = -0.73 vs. r = 0.71) and the male group (r = -0.60 vs. r =
0.57). However, compared to our results, the correlation was slightly lower for
the female group (r = -0.51 vs. r = 0.69). It is important to note that the
negative sign of the correlation is because the shorter the time, the higher
the V̇O2max.
The studies by Martin et al. [21] and Jones et al. [25], which included only male
military personnel, showed even higher correlation coefficients between
self-perception and actual performance (r = 0.87 and r = 0.85, respectively).
These results suggest a high degree of agreement between self-report and objective
performance in these specific groups of male military personnel.
When V̇O2max
values were analyzed by self-perception category (Figure 2), significant
differences were observed between groups 1 (very poor) and 2 (poor) (F (4.67) =
14.71, p < 0.001; t (67) = -2.15; Scheffé p =
0.34) and between groups 2 (poor) and 3 (moderate) (t (67) = -1.28; Scheffé p= 0.80). However, when the analysis was performed
separately by gender, it was found that women did not show significant
differences between the self-perception categories, indicating homogeneity in V̇O2max values between the female groups.
On the
other hand, males showed significant differences only between groups 4 (good)
and 5 (very good) (F (2,36) = 8.78, p < 0.001; t (36) = -1.38; Scheffe p = 0.40).
Although the analysis of variance indicated significant differences between
these two groups, the post hoc tests revealed no significant differences
between the means. The results suggest that despite the tendency for V̇O2max to increase with increasing self-perception category,
there were no statistically significant differences between the means of the
adjacent male groups.
These
results suggest that men and women may be biased in their self-perceptions of
cardiorespiratory fitness. Both men and women may tend to overestimate their
ability in the lower self-perception groups ("very poor" and
"poor") and underestimate it in the higher self-perception groups
("good" and "very good"). This tendency may explain the
higher dispersion of the data in these groups and the lack of significant
differences between the means of adjacent groups. Data analysis did not reveal
a consistent pattern of underestimation or overestimation of cardiorespiratory
fitness between men and women. The results suggest that the discrepancy between
the perception and reality of physical fitness may be more related to the
self-perception category selected by the participants than to biological sex [26].
Contrary to the results found here, the scientific literature presents divergent results on the self-perception of physical fitness between men and women, with some studies suggesting that men overestimate their abilities compared to women [27,28].
This study examined the agreement
between self-perceived cardiorespiratory fitness and the criteria proposed by
Heardy and Caixeta [17]. When analyzing the female gender, it can be seen that
all participants who rated themselves as having "very good"
cardiorespiratory fitness (group 5) were classified as "excellent"
according to the external criteria. However, for the other levels of
self-perception, the distribution of results was wider, with participants
falling into two or three different categories. A similar pattern was found for
males, except Group 5, where 50% of the participants were classified as
"very good" according to the objective criteria.
To
further analyze the relationship between self-perception and cardiorespiratory
fitness, k-means clustering was used to create more homogeneous categories
based on V̇O2max values. When these categories were compared with
participants' self-perceptions, agreement was moderate, with approximately 53%
of women and 44% of men correctly classifying themselves. This analysis
highlights the complexity of self-perception, which is influenced by various
cognitive and emotional factors and individual physiological characteristics.
Recognizing the inherent error in
objective and subjective measures is imperative. Although objective measures
are expected to have a smaller margin of error, both random and systematic,
compared to subjective measures and gold standards, it is important to
emphasize that all measuring instruments are subject to error, quantified by
the standard error of estimation. Given this scenario, the question arises as
to whether it would be equally appropriate to consider a standard error of
estimate for subjective measurements. For example, if it were possible to
assign a standard error to a Likert scale of 1 to 5, it would theoretically be
possible to achieve levels of agreement between self-perception and objective
classification of around 100% for women and 96% for men. Using more detailed
visual scales, such as a 0 to 10 scale, could significantly contribute to a
better understanding of the magnitude of error in self-reporting and,
consequently, to identify effective strategies for improving the accuracy of self-reporting.
One of the main limitations of this
study is the small sample size and possibly the homogeneity of the V̇O2max
values, which limits the robustness of the statistical analyses. In addition,
the estimation of cardiorespiratory fitness using a submaximal field test, such
as the 12-minute Cooper test, which has a correlation coefficient between 0.29
and 0.90, may affect the accuracy of the results.
However, proposing a substantial
increase in sample size and using direct methods to measure cardiorespiratory
fitness is a contradiction. Therefore, it is prudent to propose maintaining the
current sample size combined with using a direct measure of cardiorespiratory
fitness in a group that is homogeneous in terms of age and has a wide
variability in fitness. This scenario would be the most appropriate approach
for further analysis.
Conclusion
This
study investigated the validity of self-perceived cardiorespiratory fitness as
an alternative or complement to direct testing in a sample of aspirants to the
temporary officer cadre of the Brazilian Air Force. High positive and
significant correlations were observed between self-perceived fitness and V̇O2MAX,
suggesting a considerable degree of consistency in self-assessment of
cardiorespiratory capacity. This finding suggests that as V̇O2MAX
increases, so does the individual's perception of their fitness level.
Although
significant differences were found between some categories of self-perception
in the overall analysis and the male group, analyses stratified by gender
revealed nuances. Women showed no significant differences between
self-perception categories about V̇O2max, indicating group homogeneity. Men showed significant
differences only between the "good" and "very good"
categories, but post hoc tests revealed no statistically significant
differences between adjacent groups. The current results highlight potential
biases in self-perception: both men and women may overestimate fitness in lower
self-perception groups and underestimate it in higher groups.
The k-means cluster analysis showed
moderate agreement between self-perceived and objectively assessed
cardiorespiratory fitness in about half of the participants (53% of women and
44% of men), demonstrating that self-perceived and objective measures correlate
well but do not overlap perfectly. More research is needed to explore the
reasons for these discrepancies, which may be due to factors other than
physiological ability, such as cognitive and emotional factors.
Conflict of interest
None
Sources of funding
None
Authors' contributions
Concepção e desenho da pesquisa: Damasceno VO, Fanaro GB; Coleta de dados: Fanaro GB, Resende HG, Silveira LCCL, Sá PM; Análise e interpretação dos dados: Damasceno
VO; Análise estatística: Damasceno
VO; Redação do manuscrito: Damasceno VO, Sá PM, Fanaro GB, Rezende
HG, Silveira, LCCl; Revisão crítica do manuscrito quanto ao
conteúdo intelectual importante: Damasceno
VO
References
- Bayles
MP. ACSM's exercise testing and prescription. Philadelphia: Lippincott Williams
& Wilkins; 2023.
- Balady GJ, Weiner DA. Exercise testing for sports and
the exercise prescription. Cardiol Clin.
1987;5(2):183-96. PMID: 3555796
- Myers
J, Froelicher VF. Exercise testing. Procedures and implementation. Cardiol Clin. 1993;11(2):199-213. PMID: 8508447.
- Balady
GJ, Weiner DA. Exercise testing for sports and the exercise prescription. Cardiol Clin. 1987 May;5(2):183-96. PMID: 3555796.
- Bennett
H, Parfitt G, Davison K, Eston R. Validity of submaximal step tests to estimate
maximal oxygen uptake in healthy adults. Sports Med. 2016;46(5):737-50. doi: 10.1007/s40279-015-0445-1 [Crossref]
- Aandstad A. Relationship between self-reported and objectively measured physical fitness in young men and women. Eur J Sport Sci. 2023;23(2):301-9. doi: 10.1080/17461391.2021.2012597 [Crossref]
- Petersen CB, Eriksen L, Dahl-Petersen IK, Aadahl M, Tolstrup JS. Self-rated physical fitness and measured cardiorespiratory fitness, muscular strength, and body composition. Scand J Med Sci Sports. 2021;31(5):1086-95. doi: 10.1111/sms.13918 [Crossref]
- Štefan L, Paradžik P, Sporiš G. Sex and age correlations of reported and estimated physical fitness in adolescents. PLoS One. 2019;14(7):e0219217. doi: 10.1371/journal.pone.0219217 [Crossref]
- Mikkelsson L, Kaprio J, Kautiainen H, Kujala UM, Nupponen H. Associations between self-estimated and measured physical fitness among 40-year-old men and women. Scand J Med Sci Sports. 2005;15(5):329-35. doi: 10.1111/j.1600-0838.2004.00429.x [Crossref]
- Ortega FB, Ruiz JR, España-Romero V, Vicente-Rodriguez G, Martínez-Gómez D, Manios Y, et al. HELENA study group. The International Fitness Scale (IFIS): usefulness of self-reported fitness in youth. Int J Epidemiol. 2011;40(3):701-11. doi: 10.1093/ije/dyr039 [Crossref]
- Brasil.
Comando da Aeronáutica. Teste de Avaliação do Condicionamento Físico no
Comando da Aeronáutica:
NSCA 54-3. Publicado no BCA n° 087, de 21 de maio de 2020. Brasília, DF:
COMGEP; 2020a.
- Brasil. Marinha
do Brasil. Normas sobre treinamento
físico militar e testes de avaliação física na Marinha do Brasil:
CGCFN-108. Rio de Janeiro, RJ: CGCFN; 2020b.
- Brasil.
Exército Brasileiro. Diretriz para a Avaliação Física do Exército
Brasileiro: EB20-D-03.053.
Publicado no Boletim do Exército no 36, de 9 de setembro de 2022. Rio de
Janeiro, RJ: CCFEx; 2022.
- Rosado AL, Resende HG, Damasceno VO.
Diretrizes e parâmetros para o treinamento físico militar: um estudo comparado
dos documentos normativos das Forças Armadas Brasileiras. In: Anais do V
Workshop de Leituras Exploratórias em Desempenho Humano Operacional; 2023 Oct 09-10; Rio de Janeiro, RJ. Rio de Janeiro: EDUNIFA;
2024. p. 8-21.
- Thomas JR, Nelson JK, Silverman SJ. Métodos
de pesquisa em atividade física. 6ª ed. Porto Alegre: Artmed; 2012.
- Cooper KH. A means of assessing maximal oxygen intake.
Correlation between field and treadmill testing. JAMA. 1968;203(3):201-204. PMID: 5694044
- Herdy AH, Caixeta A. Brazilian cardiorespiratory fitness classification based on maximum oxygen consumption. Arq Bras Cardiol. 2016;106(5):389-95. doi: 10.5935/abc.20160070 [Crossref]
- Mukaka MM. Statistics corner: A guide to appropriate
use of correlation coefficient in medical research. Malawi Med J.
2012;24(3):69-71. PMID: 23638278
- Cohen J. Statistical power analysis for the behavioral
sciences. 2nd ed. Mahwah (NJ): Lawrence Erlbaum Associates; 1988.
- Berthold MR, Cebron N, Dill F, Gabriel TR, Kötter T, Meinl T, et al. KNIME: The Konstanz Information Miner. In:
Preisach C, Burkhardt H, Schmidt-Thieme L, Decker R. (eds). Data Analysis,
Machine Learning and Applications, Studies in Classification, Data Analysis and
Knowledge Organization. Springer Berlin Heidelberg; 2008.
- Martin RC, Grier T, Canham-Chervak M, Anderson MK, Bushman TT, DeGroot DW, et al. Validity of self-reported physical fitness and body mass index in a military population. J Strength Cond Res. 2016;30(1):26-32. doi: 10.1519/JSC.0000000000001026 [Crossref]
- Knapik
JJ, Jones BH, Reynolds KL, Staab JS. Validity of self-assessed physical
fitness. Am J Prev Med. 1992;8(6):367-72. PMID: 1482577
- Obling KH, Hansen AL, Overgaard K, Normann K, Sandbaek A, Maindal HT. Association between self-reported and objectively measured physical fitness level in a middle-aged population in primary care. Prev Med Rep. 2015;2:462-66. doi: 10.1016/j.pmedr.2015.05.010 [Crossref]
- Jensen KG, Rosthoj S, Linneberg A, Aadahl M. The association between self-rated fitness and cardiorespiratory fitness in adults. Int J Sports Med. 2018;39(6):419-25. doi: 10.1055/s-0044-102128 [Crossref]
- Jones SB, Knapik JJ, Sharp MA, Darakjy S, Jones BH. The validity of self-reported physical fitness test scores. Mil Med. 2007;172(2):115-20. doi: 10.7205/milmed.172.2.115 [Crossref]
- Bill T, Richard MR, Michael AR, Joseph D. Relationship between perceived physical ability and indices of actual physical fitness. J Sport Psychol. 1987;9(3):295-300. doi: 10.1123/jsp.9.3.295 [Crossref]
- Delignières D, Marcellini A, Brisswalter J, Legros P. Self-perception of fitness and personality traits. Percept Mot Skills. 1994;78(3Pt1):843-51. doi: 10.1177/003151259407800333 [Crossref]
- Lamb KL, Morris PG. Leisure-time physical activity as a determinant of self-perceived fitness. Percept Mot Skills. 1993;76(3 Pt1):1043-47. doi: 10.1539/joh.45.286 [Crossref]
