Rev
Bras Fisiol Exerc. 2025;24:e245622
doi: 10.33233/rbfex.v24i1.5622
REVIEW
Resistance exercise combined with aerobic exercise in
hypertensive individuals: systematic review and meta-analysis
Exercício
resistido combinado com exercício aeróbico em indivíduos hipertensos: revisão
sistemática e meta-análise
Guilherme Costa Ferreira,
Lucas Bispo Ferreira, Guilherme Santana de Freitas, André Luiz Lisboa Cordeiro
Centro Universitário Nobre, Feira de Santana, BA, Brasil
Received: February
14, 2025; Accepted: April 4, 2025.
Correspondence: André
Luiz Lisboa Cordeiro, andrelisboacordeiro@gmail.com
How to cite
Ferreira GC, Ferreira LB, Freitas GS, Cordeiro
ALL. Resistance exercise combined with aerobic
exercise in hypertensive individuals: systematic review and meta-analysis. Rev Bras Fisiol Exerc. 2025;24(1);e245622. doi: 10.33233/rbfex.v24i1.5622
Abstract
Introduction: Systemic arterial
hypertension (SAH) is one of the most common cardiovascular diseases.
Sedentarism and physical inactivity may contribute to worsening this condition,
increasing treatment costs and decreasing rehabilitation chances and life
expectancy. Combined exercise practice may be an alternative to address this
health issue, offering excellent cost-effectiveness. Objective: To review the effect of combined exercise (aerobic
exercise associated with resistance exercise) on rehabilitating patients with
SAH. Methods: This is a
systematic review using the PICO strategy, with searches conducted in the PubMED, OVID, Web of Science, PEDro,
LILACS, and SciELO databases, using the following
descriptors: arterial hypertension, elevated blood pressure, heart disease,
hypertensive individuals, resistance exercise, aerobic exercise, combined
exercise, resistance activities, and strength training, combined with the
Boolean operators "AND" and "OR". Results: Five studies were included after
selection. The combined exercise was effective in reducing blood pressure in
patients, with a mean reduction of systolic blood pressure -0.73 mmHg; 95% CI,
-1.12 to –0.34 and diastolic blood pressure -0.67 mmHg; 95% CI, -1.06 to –0.29.
Conclusion: Combined training proved to be
effective in treating patients with SAH.
Keywords:
arterial hypertension; resistance
exercise; aerobic exercise; combined exercise.
Resumo
Introdução: A hipertensão arterial sistêmica (HAS) é uma das doenças
cardiovasculares mais comuns. O sedentarismo e a inatividade física podem
contribuir para o agravamento dessa condição, aumentando os custos do
tratamento e diminuindo as chances de reabilitação e a expectativa de vida. A
prática de exercício combinado pode ser uma alternativa para lidar com esse
problema de saúde, oferecendo excelente relação custo-benefício. Objetivo:
Revisar o efeito do exercício combinado (exercício aeróbico associado ao
exercício resistido) na reabilitação de pacientes com HAS. Métodos:
Trata-se de uma revisão sistemática utilizando a estratégia PICO, com buscas
realizadas nas bases de dados PubMED, OVID, Web of Science, PEDro, LILACS e
SciELO, utilizando os seguintes descritores: hipertensão arterial, pressão
arterial elevada, doença cardíaca, indivíduos hipertensos, exercício resistido,
exercício aeróbico, exercício combinado, atividades resistidas e treinamento de
força, combinados com os operadores booleanos "AND" e "OR".
Resultados: Após a seleção, cinco estudos foram incluídos. O exercício
combinado foi eficaz na redução da pressão arterial dos pacientes, com uma
redução média da pressão arterial sistólica de -0,73 mmHg; IC 95%, -1,12 a
-0,34, e da pressão arterial diastólica de -0,67 mmHg; IC 95%, -1,06 a -0,29. Conclusão:
O treinamento combinado mostrou-se eficaz no tratamento de pacientes com HAS.
Palavras-chave: hipertensão arterial; exercício
resistido; exercício aeróbico; exercício combinado.
Introduction
Systemic arterial hypertension (SAH)
is a common chronic condition that affects millions of people worldwide, being
responsible for various functional limitations, such as reduced physical
capacity and increased cardiovascular risk [1]. Hypertensive individuals often
experience difficulty performing daily activities due to impairment of the
cardiovascular system and muscle function [2]. Regular physical exercise,
especially resistance exercise and aerobic exercise, has been identified as an
effective intervention to improve cardiovascular function and quality of life
in these patients [3,4].
Functional limitations in
hypertensive individuals develop primarily due to increased arterial stiffness,
endothelial dysfunction, and loss of muscle mass, processes that compromise the
efficiency of the cardiovascular and muscular systems [5]. Additionally,
hypertension can trigger a vicious cycle of sedentary behavior, further
exacerbating these limitations and increasing the risk of comorbidities such as
stroke and heart failure [6,7]. The progression of these limitations is often
silent, making early diagnosis and effective management of the condition more
challenging.
Aerobic exercise improves
cardiovascular capacity and the efficiency of the circulatory system in
hypertensive individuals, helping to reduce blood pressure levels and increase
physical endurance [8]. On the other hand, resistance exercise contributes to
increased muscle strength, improved body composition, and enhanced muscle
functionality, which are essential for functional independence [9]. The
combination of these two types of exercises has shown promising results in
improving both cardiovascular health and the overall functional capacity of
hypertensive individuals [10].
This study is justified by the need
to gain a deeper understanding of the combined effects of resistance and
aerobic exercise on the functionality and cardiovascular health of hypertensive
individuals. Although there is evidence highlighting the benefits of each type
of exercise separately, few studies have investigated the efficacy of a
combined protocol. The aim of this study is to review the impacts of combining
resistance and aerobic exercises on the blood pressure of individuals with systemic
arterial hypertension.
Methods
Study type and registration
This systematic review was conducted
following the guidelines of the Preferred Reporting Items for Systematic
Reviews and Meta-Analyses (PRISMA)
[11]. This study was registered in the International Prospective Register of
Systematic Reviews (PROSPERO)
under the number CRD42025633308.
Eligibility criteria
For this systematic review, the PICOS strategy was used, where the
population studied consisted of patients with systemis arterial hypertension. The intervention involved performing both aerobic and resistance training, in
comparison with patients who did not engage in any of these activities or
performed only one of them. The outcomes were related to blood pressure, lean body
mass, strength, and cardiorespiratory function.
Randomized clinical trials were
used, with no restrictions on language or year. To be eligible, the clinical
trial had to study aerobic exercise combined with resistance training in
individuals of both sexes, aged over 18 years, and diagnosed with systemic
arterial hypertension. The studies were excluded if the patients had
comorbidities other than systemic hypertension, if diuretics or beta-blockers
were used with the exercise, if only aerobic or resistance exercise was
assessed individually, or if blood pressure was assessed at a time other than
pre- and post-training, for example during sleep.
Sources of information
We conducted a computer-based search,
consulting PubMED, OVID, Web of Sciences,
Physiotherapy Evidence Database (PEDro), Latin American and Caribbean Health
Sciences Literature (LILACS), and Scientific Electronic Library Online
(SciELO). We also searched the reference lists of previous systematic reviews
and eligible clinical trials for this review. The search for articles was
completed in December 2024.
Search
The research was based on the
previously described PICOS strategy and the Boolean operators AND and OR. The search strategy is presented in Supplement 1.
Data collection process
For the extraction of selected
articles, titles were reviewed (first stage), followed by abstracts (second
stage), and full-text reading (third stage). Subsequently, an exploratory
reading of the selected studies was conducted, followed by a selective and
analytical reading. The data extracted from the articles were summarized by
author, journal, year, title, and conclusions to gather key information for the
research.
The assessment of the methodological
quality of the studies was conducted by two independent reviewers. In cases of
disagreement between them, the article was read in fully for reevaluation. If
the disagreement persisted, a third reviewer assessed the study and made the
final decision.
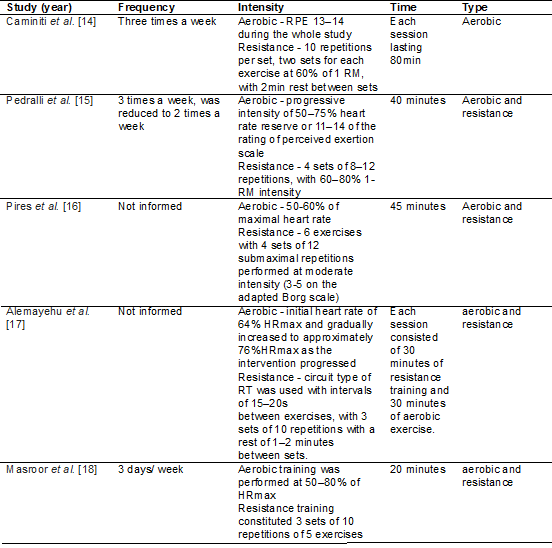
Data items
Four authors independently extracted
data from the published reports using a standardized data extraction process,
considering study population aspects such as mean age, sex, number of patients,
and diagnosis, as well as aspects of the intervention performed, including
sample size, type of inspiratory muscle training, presence of supervision,
intensity, frequency, and duration of each session. Additionally, follow-up,
loss to follow-up, outcome measures, and reported results were analyzed.
Quality of each study
The methodological quality was assessed
using the PEDro scale, which scores 11 items: (1) eligibility criteria, (2)
random allocation, (3) concealed allocation, (4) baseline comparison, (5)
blinding of participants, (6) blinding of therapists, (7) blinding of
assessors, (8) adequate follow-up, (9) intention-to-treat analysis, (10)
between-group comparisons, and (11) point estimates and variability. Items are
scored as present (1) or absent (0), resulting in a maximum total score of 10
points, as the first item is not included in the final score.
Synthesis of results
The presence of heterogeneity was
evaluated using the Chi2 test and the I2 statistic. This statistic illustrates
the percentage of variability in effect estimates from heterogeneity rather
than sampling error.
Statistical assessment
The mean difference between groups
and the respective 95% confidence intervals were calculated and used to
quantify the effect of continuous outcomes. For the meta-analyzes in which the
studies used the same scales, the results were presented as mean difference
(MD) and 95% confidence intervals. Otherwise, the effects were calculated using
standardized mean difference (SMD) and 95% confidence intervals. The effect
size of the interventions was defined as small (MD < 10% of the scale or SMD
< 0.4); moderate (MD = 10% to 20% of the scale or SMD = 0.41 to 0.7) or
large (MD > 20% of the scale or SMD > 0.7).
Results
Selection and characteristics
of the studies
According to the data presented in the
article selection flowchart (Figure 01), the database search yielded a total of
866 articles. Initially, 543 were excluded based on title screening. Then, out
of the 189 articles evaluated based on abstract reading, 165 were considered
not directly related to the topic of this study. Thus, 24 articles were
selected for full-text reading. Of these, 10 were excluded for using only
aerobic activity as a treatment for hypertension, and 9 for not evaluating both
aerobic and resistance activities together. Therefore, this systematic review
included 5 articles that met the eligibility criteria for inclusion in the
present review.
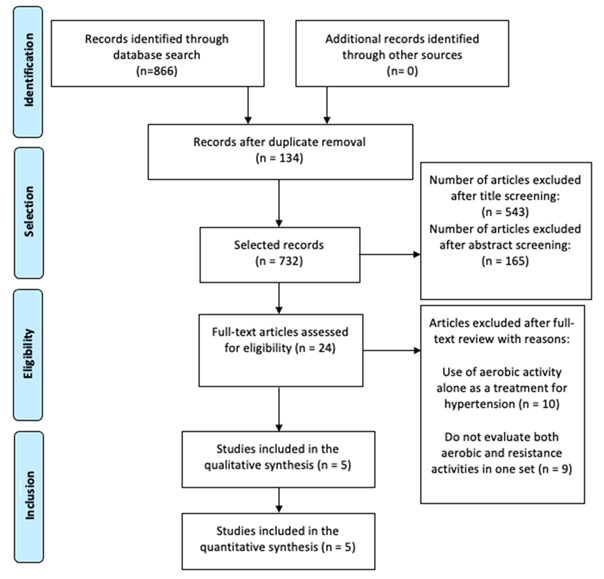
Figure 1 – Research strategy flowchart
Methodological quality results
According
to the PEDro scale, four studies
were classified as having moderate methodological quality, and only one was
rated as high quality. All studies already had their scores available on the
PEDro website. The criteria assessed by the PEDro scale and the scores obtained
by each study are detailed below in Table I.
Table I - Classification of articles on the PEDro
Scale

Items on the PEDro Scale: (1) Eligibility criteria were specified (* - this item is not used to calculate
the PEDro score); (2) Subjects were randomly allocated to groups; (3)
Allocation of subjects was concealed; (4) Groups were initially similar
concerning the most important prognostic indicators; (5) All subjects
participated in the study blindly; (6) All therapists administering the therapy
did so blindly; (7) All assessors measuring at least one key outcome did so
blindly; (8) Measurements of at least one key outcome were obtained in more
than 85% of the subjects initially allocated to the groups; (9) All subjects
from whom outcome measurements were obtained received the treatment or control
condition as allocated, or when this was not the case, data analysis was
performed for at least one outcome by intention-to-treat; (10) Results of
statistical inter-group comparisons were reported for at least one key outcome;
(11) The study presents both precision measures and variability measures for at
least one key outcome. Abbreviations: 1 = Item present; 0 = Item not present
Sistolic blood pressure
Four studies analyzed the impact of exercise on systolic
blood pressure. For the meta-analysis of this comparison, a random model was
used (I2 = 92%, df = 3, p < 0.00001), in which
there was a statistically significant difference between the groups in the
comparison between the exercise and the control (difference between the means
-0.73 mmHg; 95% CI, -1.12 to –0.34; Fig. 2).

Figure 2 - Forest plot of the results of the meta-analysis
Diastolic blood pressure
Four studies analyzed the impact of exercise on
diastolic blood pressure. For the meta-analysis of this comparison, a random
model was used (I2 = 91%, df = 3, p < 0.00001), in
which there was a statistically significant difference between the groups in
the comparison between the exercise and the control (difference between the
means -0.67 mmHg; 95% CI, -1.06 to –0.29; Fig. 3).

Figure 3 - Forest plot of the results of the meta-analysis
Discussion
The literature on the effects of physical exercise in
reducing blood pressure in hypertensive
individuals is extensive and consistently highlights the efficacy of both aerobic exercise and resistance exercise,
whether performed separately or in combination. Although the magnitude of the
response may vary depending on the type of exercise, the duration of the
program, and the characteristics of the studied population, the findings
suggest that physical exercise, in general, provides substantial benefits in
hypertension management.
The reduction in blood pressure
observed in the reviewed studies aligns with what is widely reported in the
literature, where both aerobic and resistance exercise have positive effects on BP. Caminiti et al. [14], for
example, observed significant BP reductions after 12 weeks of training, with no
differences between groups that performed aerobic exercise followed by
resistance training. This lack of difference between modalities can be
explained by the mechanics of exercise, where both aerobic and resistance
training contribute to BP reduction through distinct but complementary
mechanisms. Aerobic exercise, by improving crdiorespiratory fitness, helps decrease peripheral vascular resistance and enhances endothelial function.
Meanwhile, resistance training, by increasing muscle mass may reduce arterial stiffness and
promote better regulation of the autonomic nervous system. These combined effects may be responsible for the
overall BP reduction observed, regardless of the exercise order.
On the other hand, the study by Pedralli et al. [15], which investigated
different training modalities (aerobic, resistance, and combined), indicated
that aerobic exercise had a stronger impact on systolic blood pressure, with a reduction of 5.1 mmHg, while the
resistance group experienced a decrease of 4.0 mmHg. This finding is consistent
with previous studies suggesting that aerobic exercise has a more pronounced
effect on SBP due to increased blood volume
and improved cardiac and vascular function,
facilitating a reduction in pressure during physical exertion. The underlying
mechanism involves cardiovascular adaptations that decrease arterial stiffness and
enhance endothelial function,
both critical factors in blood pressure regulation. Additionally, Alemayehu et al. [17] observed a more significant reduction in
their participants after 12 weeks of combined exercise, with a drop of 17.75
mmHg in SBP and 12.5 mmHg in diastolic blood pressure. This could be explained by the broader range
of physiological adaptations promoted by combined training, which impacts both
the cardiovascular system and increases in muscle mass and
strength—two factors that may interact to enhance BP control more effectively.
Another important aspect observed in
the studies was the favorable response of exercise in managing more resistant
cases of hypertension, as seen in
the study by Pires et al. [16], which focused on
patients with resistant hypertension. After eight weeks of aerobic, resistance, and combined
exercise, participants showed a significant reduction in ambulatory blood pressure, a particularly relevant finding since patients with
resistant hypertension often struggle to control BP despite using multiple
medications. In these cases, exercise may help not only by reducing peripheral vascular resistance but also by improving function and modulating
the sympathetic nervous system, both of which are often dysregulated in resistant
hypertensive patients. These findings are supported by Masroor et al. [17], who observed a significant BP reduction in
sedentary women with hypertension after just four weeks of combined training,
reinforcing the idea that even short-term exercise programs can provide
substantial benefits.
The reduction in blood pressure (BP)
observed after exercise can be explained by several physiological mechanisms.
Aerobic exercise improves the efficiency of the cardiovascular system by
increasing the heart's ability to pump blood and promoting the dilation of
blood vessels, mainly through the improvement of endothelial function, which
increases the release of nitric oxide, promoting vasodilation [19].
Additionally, aerobic exercise increases plasma volume, reducing blood
viscosity and facilitating blood flow, which contributes to a decrease in
peripheral vascular resistance [20]. On the other hand, resistance exercise
increases muscle mass, creating a larger "reservoir" of blood in the
muscles, which reduces peripheral resistance and, consequently, BP [21]. It
also improves endothelial function and decreases sympathetic nervous system
activation, reducing vasoconstriction and contributing to BP control [22]. The
combination of both types of exercise results in a more robust response,
affecting both the cardiovascular and musculoskeletal systems, with adaptations
that help effectively control BP [23].
Studies focusing on populations with resistant hypertension, such as Pires et al. [16], indicate that exercise can be a
particularly valuable intervention, especially when combined with
pharmacological therapy. Resistant hypertension is often associated with
vascular control imbalances, impaired renal function, and
heightened sympathetic nervous system activity, and exercise may help mitigate these
effects. The activation of the parasympathetic nervous system and the reduction in sympathetic activity during
exercise appear to be key factors contributing to the observed improvements in blood pressure.
The main limitations of this study
include high heterogeneity among the studies selected for the meta-analysis,
which may have influenced the consistency of the results and the interpretation
of the data. Variability in methods, populations, and interventions across the
included studies makes it difficult to generalize the conclusions and may
reduce the precision of the estimates. Additionally, the number of volunteers
in the studies does not necessarily guarantee robustness in the findings, as
there is the possibility of statistical errors leading to spurious results.
These errors may occur due to uncontrolled variabilities or flaws in study
design, affecting the validity of the conclusions. These limitations suggest
that the results should be interpreted with caution, and further research with
standardized methodologies is needed to confirm the findings.
Conclusion
In summary, the reviewed studies
reinforce the importance of physiscal exercise in hypertension
management, emphasizing aerobic and resistance modalities, particularly combined training, which
appears to offer the greatest benefits. The physiological response to exercise
involves cardiovascular and musculoekeletal
adaptations that work synergistically to lower blood pressure.
Although aerobic exercise seems to have a more pronounced effect on reducing systolic blood pressure, combined training provides additional
benefits, especially for individuals with more severe or resistant hypertension.
Thus, the prescription of physical exercise should be considered an effective
therapeutic strategy in hypertension treatment, serving as an alternative or
complement to traditional pharmacological treatments.
Conflict of interest
The authors declare no conflict of interest.
Sources of funding
The authors declare that they have not received funding.
Author’s contribution
Conception and design of the research: Cordeiro
AL, Costa G, Freitas G, Bispo L; Data
collection: Costa G, Freitas G, Bispo L; Data analysis and interpretation: Cordeiro
AL, Statistical analysis: Cordeiro
AL; Manuscript writing: Costa G,
Freitas G, Bispo L, Critical revision of
the manuscript for important intellectual content: Cordeiro AL
References
- Kreutz R, Brunström M, Burnier M, Grassi G,
Januszewicz A, Muiesan ML,
et al. 2024 European Society of Hypertension clinical practice guidelines for
the management of arterial hypertension. Eur J Intern
Med. 2024;126:1-15. doi: 10.1016/j.ejim.2024.05.033 [Crossref]
- Madden BP, Shaw EJ.
Skeletal muscle exercise training in pulmonary arterial hypertension. Int J Cardiol. 2017;246:59-60. doi: 10.1016/j.ijcard.2017.03.017 [Crossref]
- Dibben GO, Faulkner
J, Oldridge N, Rees K, Thompson DR, Zwisler AD, Taylor RS. Exercise-based
cardiac rehabilitation for coronary heart disease: a meta-analysis. Eur Heart J. 2023 Feb 7;44(6):452-469. doi: 10.1093/eurheartj/ehac747 [Crossref]
- Hansen D, Abreu A,
Ambrosetti M, Cornelissen V, Gevaert A, Kemps H, et al. Exercise intensity
assessment and prescription in cardiovascular rehabilitation and beyond: why
and how: a position statement from the Secondary Prevention and Rehabilitation
Section of the European Association of Preventive Cardiology. Eur J Prev Cardiol. 2022 Feb
19;29(1):230-245.doi: 10.1093/eurjpc/zwab007
[Crossref] Erratum in: Eur J Prev Cardiol.
2024 Sep 20;31(13):e102. doi: 10.1093/eurjpc/zwad397 [Crossref]
- Lopes
S, Afreixo V, Teixeira M, Garcia C, Leitão C, Gouveia
M, et al. Exercise training reduces
arterial stiffness in adults with hypertension: a systematic review and
meta-analysis. J Hypertens. 2021;39(2):214-222.doi: 10.1097/HJH.0000000000002619 [Crossref]
- Mills KT,
Stefanescu A, He J. The global epidemiology of hypertension. Nat Rev Nephrol.
2019;15(1):45-57. doi: 10.1038/s41581-018-0093-4 [Crossref]
- Pescatello LS,
Franklin BA, Fagard R, et al. Exercise and
hypertension: American College of Sports Medicine position stand. Med Sci
Sports Exerc. 2022;54(6):1077-1095.doi: 10.1249/MSS.0000000000002762 [Crossref]
- Tanaka H, Monahan
KD, Seals DR. Age-predicted maximal heart rate revisited. J Am Coll Cardiol. 2020;75(5):500-10. doi: 10.1016/j.jacc.2019.11.052 [Crossref]
- Fyfe JJ, Hamilton
DL, Daly RM. Minimal-dose resistance training for improving muscle mass,
strength, and function: a narrative review of current evidence and practical
considerations. Sports Med. 2022;52(3):463-79. doi: 10.1007/s40279-021-01605-8 [Crossref]
- Saeidi M, Ravanbod R. Effects of resistance added on aerobic training
on autonomic function in cardiac patients. Anatol J Cardiol.
2022;26(2):80-89. doi: 10.5152/AnatolJCardiol.2021.215 [Crossref]
- Maher D, Liberati
A, Tetzlaff J, Altman DG, The PRISMA Group. Preferred Reporting Items for
Systematic Reviews and Meta- Analyses: The PRISMA Statement. PLoS Med.2009;6(7):e1000097
- Santos CMC, Pimenta
CAM, Nobre MRC. The PICO strategy for the research question construction and
evidence search. Rev Lat-Am Enfermagem.
2007;15(3):508-11. doi: 10.1590/S0104-11692007000300023 [Crossref]
- Maher CG,
Sherrington C, Herbert RD, Moseley AM, Elkins M. Reliability of the PEDro scale for rating quality of randomized controlled
trials. Phys Ther 2003; 83:713-21. PMID: 12882612
- Caminiti G, Iellamo F, Mancuso A, Cerrito A, Montano M, Manzi V, Volterrani M. Effects of 12 weeks of aerobic versus
combined aerobic plus resistance exercise training on short-term blood pressure
variability in patients with hypertension. J Appl Physiol
(1985). 2021;130(4):1085-92. doi: 10.1152/japplphysiol.00910.2020 [Crossref]
- Pedralli ML, Marschner RA, Kollet DP, Neto SG, Eibel B,
Tanaka H, Lehnen AM. Different exercise training modalities produce similar
endothelial function improvements in individuals with prehypertension or
hypertension: a randomized clinical trial Exercise, endothelium and blood
pressure. Sci Rep. 2020 May 6;10(1):7628. doi: 10.1038/s41598-020-64365-x [Crossref] Erratum in: Sci Rep. 2020 Jun 24;10(1):10564. doi: 10.1038/s41598-020-67586-2 [Crossref]
- Pires NF,
Coelho-Júnior HJ, Gambassi BB, Faria APC, Ritter AMV,
Barboza CA, et al. Combined aerobic and resistance exercises evokes longer
reductions on ambulatory blood pressure in resistant hypertension: a randomized
crossover trial. Cardiovasc Ther. 2020;2020:8157858. doi: 10.1155/2020/8157858 [Crossref]
- Alemayehu A, Teferi
G. Effectiveness of aerobic, resistance, and combined training for hypertensive
patients: a randomized controlled trial. Ethiop J Health Sci.
2023;33(6):1063-1074. doi: 10.4314/ejhs.v33i6.17 [Crossref]
- Masroor S, Bhati P,
Verma S, Khan M, Hussain ME. Heart rate variability following combined aerobic
and resistance training in sedentary hypertensive women: a randomised
control trial. Indian Heart J. 2018;70(Suppl 3):S28-S35. doi: 10.1016/j.ihj.2018.03.005 [Crossref]
- Li C, Wu S, Lei B,
Zang W, Tao X, Yu L. Effect of aerobic exercise on endothelial function in
hypertensive and prehypertensive patients: a systematic review and
meta-analysis of randomized controlled trials. J Hypertens.
2025 May 1;43(5):727-38. doi: 10.1097/HJH.0000000000003980 [Crossref]
- Dawson EA, Green
DJ, Cable NT, Thijssen DH. Effects of acute exercise
on flow-mediated dilatation in healthy humans. J Appl Physiol
(1985). 2013 Dec;115(11):1589-98. doi: 10.1152/japplphysiol.00450.2013 [Crossref]
- Ratajczak M,
Krzywicka M, Szulińska M, Musiałowska
D, Kusy K, Karolkiewicz J. Effects of 12-week
combined strength and endurance circuit training program on insulin sensitivity
and retinol-binding protein 4 in women with insulin-resistance and overweight
or mild obesity: A randomized controlled trial. Diabetes Metab Syndr Obes. 2024;17:93-106. doi: 10.2147/DMSO.S432954 [Crossref]
- Akins JD, Washio T,
Fu Q. Autonomic control of blood pressure in women: The roles of hypertension
and aging. Auton Neurosci. 2025;260:103274. doi: 10.1016/j.autneu.2025.103274 [Crossref]
- Pescatello LS,
Franklin BA, Fagard RH, Farguhar
WB, Kelley GA, et al. American College of Sports Medicine position stand.
Exercise and hypertension. Med Sci Sports Exerc.
2015;47(9):1973-83.
Annex 1
(("hypertense"[All
Fields] OR "hypertension"[MeSH Terms] OR
"hypertension"[All Fields] OR "hypertension s"[All Fields]
OR "hypertensions"[All Fields] OR "hypertensive"[All
Fields] OR "hypertensive s"[All Fields] OR
"hypertensives"[All Fields] OR ("hypertension"[MeSH Terms] OR "hypertension"[All Fields] OR
("blood"[All Fields] AND "pressure"[All Fields] AND
"high"[All Fields]) OR "blood pressure high"[All Fields])
OR ("hypertension"[MeSH Terms] OR
"hypertension"[All Fields] OR ("blood"[All Fields] AND
"pressures"[All Fields] AND "high"[All Fields]) OR
"blood pressures high"[All Fields]) OR ("hypertension"[MeSH Terms] OR "hypertension"[All Fields] OR
("high"[All Fields] AND "blood"[All Fields] AND
"pressure"[All Fields]) OR "high blood pressure"[All
Fields]) OR ("hypertension"[MeSH Terms] OR
"hypertension"[All Fields] OR ("high"[All Fields] AND
"blood"[All Fields] AND "pressures"[All Fields]) OR
"high blood pressures"[All Fields])) AND ("exercise"[MeSH Terms] OR "exercise"[All Fields] OR
"exercises"[All Fields] OR "exercise therapy"[MeSH Terms] OR ("exercise"[All Fields] AND
"therapy"[All Fields]) OR "exercise therapy"[All Fields] OR
"exercising"[All Fields] OR "exercise s"[All Fields] OR
"exercised"[All Fields] OR "exerciser"[All Fields] OR
"exercisers"[All Fields] OR ("exercise"[MeSH
Terms] OR "exercise"[All Fields] OR ("exercise"[All Fields]
AND "physical"[All Fields]) OR "exercise physical"[All
Fields]) OR ("exercise"[MeSH Terms] OR
"exercise"[All Fields] OR ("exercises"[All Fields] AND
"physical"[All Fields]) OR "exercises physical"[All
Fields]) OR ("exercise"[MeSH Terms] OR
"exercise"[All Fields] OR ("physical"[All Fields] AND
"exercise"[All Fields]) OR "physical exercise"[All Fields])
OR ("exercise"[MeSH Terms] OR
"exercise"[All Fields] OR ("physical"[All Fields] AND
"exercises"[All Fields]) OR "physical exercises"[All
Fields]) OR ("exercise"[MeSH Terms] OR
"exercise"[All Fields] OR ("physical"[All Fields] AND
"activity"[All Fields]) OR "physical activity"[All Fields])
OR ("exercise"[MeSH Terms] OR
"exercise"[All Fields] OR ("activities"[All Fields] AND
"physical"[All Fields]) OR "activities physical"[All
Fields]) OR ("exercise"[MeSH Terms] OR
"exercise"[All Fields] OR ("activity"[All Fields] AND
"physical"[All Fields]) OR "activity physical"[All Fields])
OR ("exercise"[MeSH Terms] OR
"exercise"[All Fields] OR ("physical"[All Fields] AND
"activities"[All Fields]) OR "physical activities"[All
Fields]) OR ("exercise"[MeSH Terms] OR
"exercise"[All Fields] OR ("exercise"[All Fields] AND
"aerobic"[All Fields]) OR "exercise aerobic"[All Fields])
OR ("exercise"[MeSH Terms] OR
"exercise"[All Fields] OR ("aerobic"[All Fields] AND
"exercise"[All Fields]) OR "aerobic exercise"[All Fields])
OR ("exercise"[MeSH Terms] OR
"exercise"[All Fields] OR ("aerobic"[All Fields] AND
"exercises"[All Fields]) OR "aerobic exercises"[All
Fields]) OR ("exercise"[MeSH Terms] OR
"exercise"[All Fields] OR ("exercises"[All Fields] AND
"aerobic"[All Fields]) OR "exercises aerobic"[All Fields])
OR ("exercise"[MeSH Terms] OR
"exercise"[All Fields] OR ("exercise"[All Fields] AND
"isometric"[All Fields]) OR "exercise isometric"[All
Fields]) OR ("exercise"[MeSH Terms] OR
"exercise"[All Fields] OR ("exercises"[All Fields] AND
"isometric"[All Fields]) OR "exercises isometric"[All
Fields]) OR ("exercise"[MeSH Terms] OR
"exercise"[All Fields] OR ("isometric"[All Fields] AND
"exercises"[All Fields]) OR "isometric exercises"[All
Fields]) OR ("exercise"[MeSH Terms] OR
"exercise"[All Fields] OR ("isometric"[All Fields] AND
"exercise"[All Fields]) OR "isometric exercise"[All
Fields]) OR ("exercise"[MeSH Terms] OR
"exercise"[All Fields] OR ("acute"[All Fields] AND
"exercise"[All Fields]) OR "acute exercise"[All Fields]) OR
("exercise"[MeSH Terms] OR
"exercise"[All Fields] OR ("acute"[All Fields] AND
"exercises"[All Fields]) OR "acute exercises"[All Fields])
OR ("exercise"[MeSH Terms] OR
"exercise"[All Fields] OR ("exercise"[All Fields] AND
"acute"[All Fields]) OR "exercise acute"[All Fields]) OR
("exercise"[MeSH Terms] OR
"exercise"[All Fields] OR ("exercises"[All Fields] AND
"acute"[All Fields]) OR "exercises acute"[All Fields]) OR
("exercise"[MeSH Terms] OR
"exercise"[All Fields] OR ("exercise"[All Fields] AND
"training"[All Fields]) OR "exercise training"[All Fields])
OR ("exercise"[MeSH Terms] OR
"exercise"[All Fields] OR ("exercise"[All Fields] AND
"trainings"[All Fields]) OR "exercise trainings"[All
Fields]) OR ("exercise"[MeSH Terms] OR
"exercise"[All Fields] OR ("training"[All Fields] AND
"exercise"[All Fields]) OR "training exercise"[All Fields])
OR ("exercise"[MeSH Terms] OR
"exercise"[All Fields] OR ("trainings"[All Fields] AND
"exercise"[All Fields])))) AND (clinicaltrial[Filter])